非甲状腺疾病综合征对急诊超高龄患者预后的影响
2016-11-11李永霞杨开超朱晓光李梅芳封启明
李永霞 杨开超 朱晓光 李梅芳 封启明⋆
非甲状腺疾病综合征对急诊超高龄患者预后的影响
李永霞杨开超朱晓光李梅芳封启明⋆
目的 探讨急诊超高龄患者非甲状腺疾病综合征(NTIS)的发生率及其对患者预后的影响。方法 回顾性分析2014年1月至2015年1月≥80岁的急诊内科448例住院患者的临床资料。根据甲状腺素水平将患者分为NTIS组(n=324)与对照组(n=124),比较两组病死率差异。根据患者住院期间是否存活,分为死亡组(n=48)与存活组(n=400),比较两组NTIS发生率差异。应用Logistic回归分析影响超高龄住院患者预后的危险因素。结果 448例患者平均年龄(85.6±4.0)岁,其中男198例,女250例;NTIS发生率66.4%。NTIS组病死率明显高于对照组(13.6% vs 3.2%,P=0.001);死亡组FT3(游离T3)明显低于存活组(2.0% vs 2.9%,P<0.001),死亡组中NTIS发生率明显高于存活组(91.7% vs 70%,P=0.001);FT3<2.75(OR=0.116,95% CI:0.02-0.52)及合并脑梗死(OR=4.49,95%CI:1.83-11.02)是超高龄患者死亡的独立危险因素;FT3对超高龄患者死亡的最佳预测值是2.605Pmol/L。结论 急诊超高龄患者中的NTIS发生率极高,且合并NTIS的急诊超高龄患者预后不良,病死率极高。
非甲状腺疾病综合征 超高龄 发生率 预后
急慢性危重病或饥饿时体内甲状腺激素水平可发生异常,称为非甲状腺疾病综合征(NTIS)。NTIS常表现为低T3综合征,即血清游离T3(FT3)降低,TSH稍降低或正常,反T3(rT3)升高,游离T4(FT4)正常[1]。NTIS临床症状与甲状腺激素水平、疾病种类和病情严重程度密切相关[2-4]。研究表明,老年患者NTIS发生率高,NTIS常反映患者病情危重,预后不良[5],NTIS的发生与病死率增加呈正相关[6]。随着年龄的增长,NTIS发病率亦升高[6-8]。但Corsonello A[9]等发现百岁老人的子孙与同龄人相比甲状腺功能差,甲状腺功能低下者寿命长。本文探讨急诊超高龄患者NTIS的发生率,并分析甲状腺功能对超高龄患者预后的影响。
1 临床资料
1.1一般资料 2014年1月至2015年1月本院急诊室收治危重病患者448例。男198例,女250例;年龄80~100岁,平均年龄(85.6±4.0)岁。根据是否存在NTIS分为正常对照组及NTIS组。其中NTIS组324例,男139例,女185例,年龄80~100岁,平均年龄(85.8±4.1)岁。正常对照组124例,男59例,女65例;年龄80~96岁,平均年龄(85.1±3.7)岁。纳入标准:(1)年龄≥80岁。(2)入院第二天晨即行血清甲状腺素水平测定。排除标准:(1)既往有下丘脑、垂体、甲状腺疾病。(2)<2周有胺碘酮、激素、5-氟尿嘧啶等影响甲状腺功能药物的用药史。
1.2方法 (1)数据收集:所有入选患者信息均由同一组有经验的医师采集。采集信息包括人口学特征、肝肾凝血功能检查记录、合并症、住院时间等。(2)甲状腺功能测定及NITS的诊断:所有患者均于入院后第2天晨空腹采取肘前静脉血。血清TSH、FT4、FT3水平采用电化学发光法检测。参考范围:TSH 0.27~4.2mIU/L;FT4 12~122pmol/L;FT3 3.1~6.8pmol/L。NTIS诊断:血清游离T3(FT3)降低(FT3<3.1pmol/L),TSH稍降低或正常(TSH≤0.27pmol/L),游离T4(FT4)正常。(3)其它生化指标测定:患者于入院当晚禁食,次晨空腹采集静脉血,采用全自动生化仪(日本日立公司)测定血常规、CRP、INR、肝肾功能、pro-BNP等。1.3 统计学方法 采用SPSS 18.0软件。正态分布计量资料用(x±s)表示,非正态分布计量资料用中位数表示,两组计量资料比较,采用两独立样本t检验;计数资料用百分率表示,组间比较用χ2检验或Fisher's exact检验;预后采用Logistic回归;以P<0.05为差异有统计学意义。
2 结果
2.1两组临床资料比较 见表1。
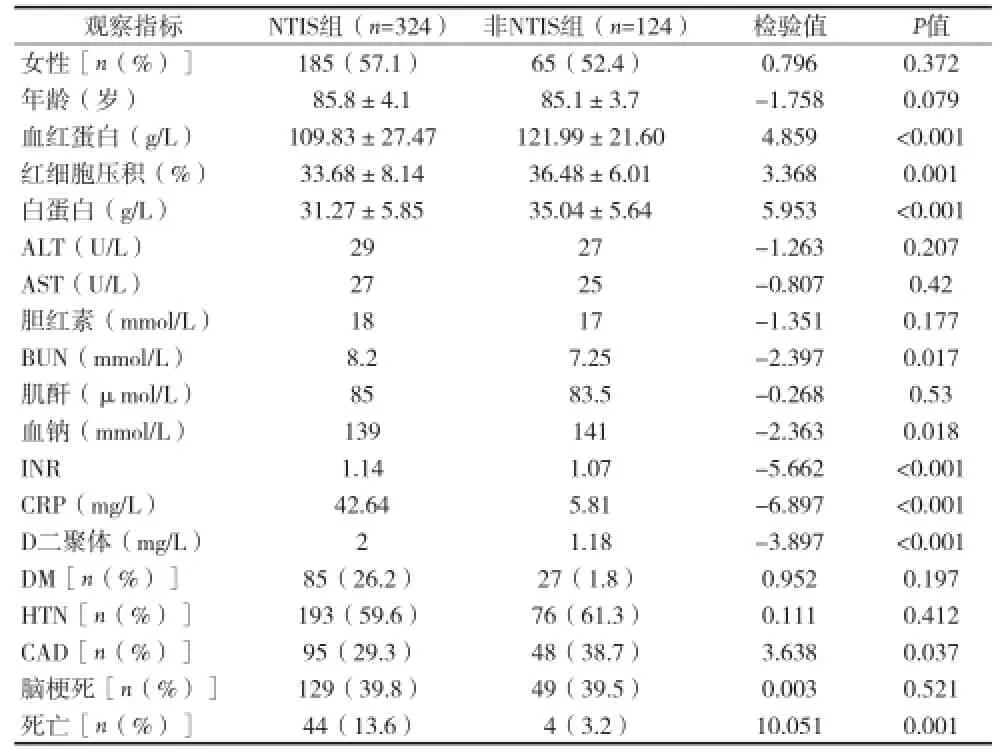
表1 两组临床资料比较(x±s)
2.2死亡组与存活组临床资料比较 住院期间死亡的患者纳入死亡组(n=48),其余患者纳入存活组。死亡组中血清FT3水平低于存活组,胆红素、尿素、INR、CRP、D-二聚体、肌钙蛋白高于存活组。死亡组冠心病、脑梗死及NTIS发生率高于存活组,见表2。
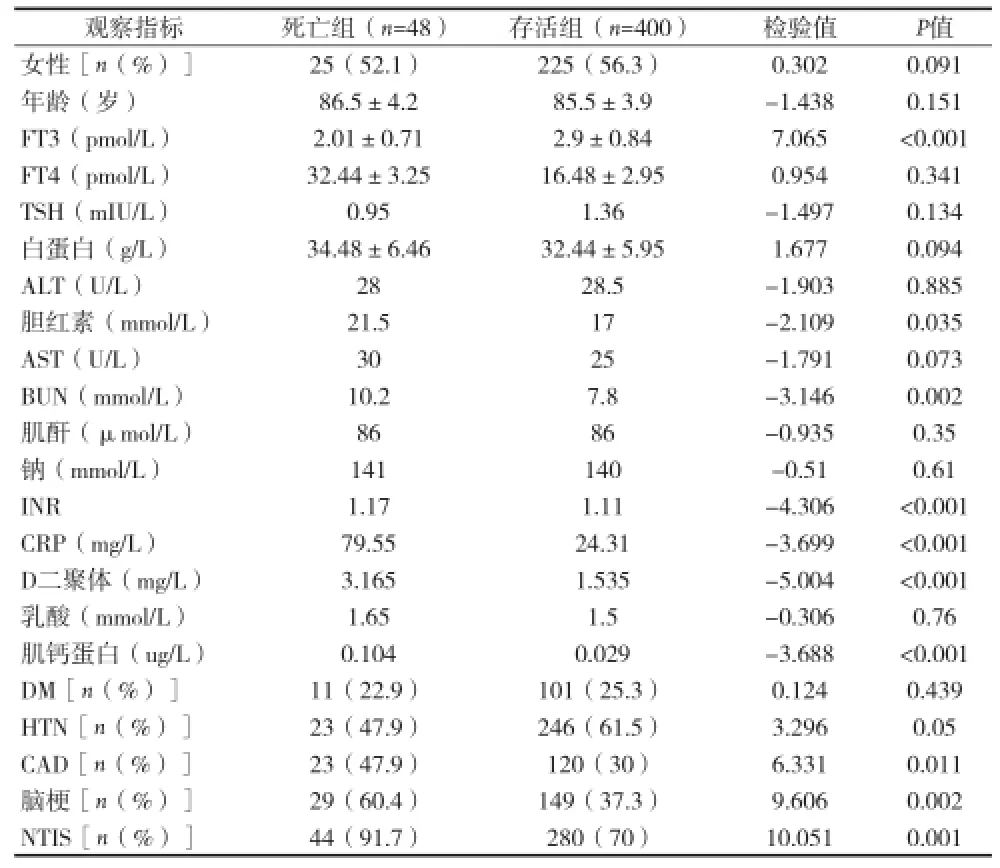
表2 死亡组与存活组临床资料比较(x±s)
2.3Logistic回归分析结果 单因素logistic回归分析显示,pro-BNP>4643ng/L、血尿素氮>10.6mmol/L、冠心病、CRP>54.31mg/L、D-二聚体>2.8mg/L、INR>1.17及 FT3<2.75pmol/L是超高龄患者死亡的危险因素。多因素logistic回归分析结果显示FT3<2.75pmol/L(OR=0.116,95% CI:0.02~0.52)及合并脑梗死(OR=4.49,95%CI:1.83~11.02)是超高龄患者死亡的独立危险因素(见表3)。
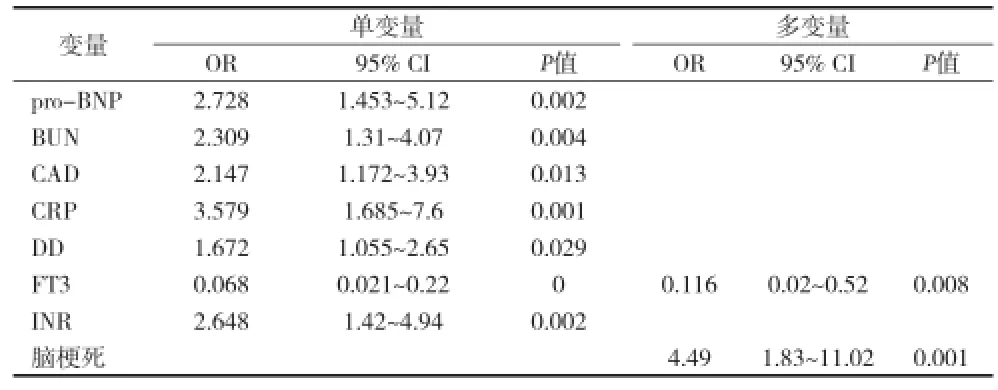
表3 超高龄患者死亡的独立危险因素Logistic回归分析结果
2.4FT3的ROC曲线分析 ROC曲线发现FT3对死亡的最佳预测值是2.605Pmol/L(灵敏度0.56,特异度0.13)。本研究FT3正常参考低值是3.1pmol/L,其灵敏度和特异度分别为:0.318,0.958,见图1。

图1 FT3ROC曲线
3 讨论
既往研究发现急性发病住院80~89岁患者NTIS发病率62%[6],>60岁为65%[8],本资料中急诊超高龄患者NTIS发生率66.4%,与既往研究相一致。超高龄死亡患者NTIS发生率91.7%,与存活组70%比较,差异有统计学意义。目前,血清甲状腺激素水平对死亡的预测各研究不一致[10-14]。研究认为血清FT3是生活自理老年患者死亡的最好预测因子[11],FT3升高被认为是NTIS的早期改变[12]。Tognini S[10]认为,FT3对老年患者死亡有预测作用,但也有研究认为FT4降低的患者病死率最高[13-14]。本资料显示,死亡组中FT3明显低于存活组,表明>80岁老年患者的预后和FT3相关,造成这一现象的原因可能是血清FT3与机体炎症反应状态密切相关[10,15]。本资料显示,死亡组中血清胆红素、尿素、INR、D二聚体、肌钙蛋白水平显著高于存活组,死亡组脑梗死率及NTIS发生率明显高于存活组,表明肝肾功能[16],凝血功能及心功能异常的患者或合并脑梗死的患者预后更差。血清FT3水平对患者预后有很好的预测作用,血清FT3水平越低,患者死亡可能性越大,这与既往多数研究结果一致[10]。同时,合并脑梗死是超高龄患者死亡的独立危险因素。造成这一现象的原因可能与脑梗死并发症多,死亡风险大相关,其具体作用机制还有待进一步研究。
Tognini S等[10]研究认为,炎症反应在NTIS发生中起着重要作用,本资料亦显示NTIS患者CRP明显升高。NTIS患者INR水平明显高于非NTIS者,可能与甲状腺激素影响凝血因子合成及影响甲状腺相关自身免疫过程有关[17]。NTIS组患者血红蛋白及红细胞压积低于对照组,与甲状腺激素尤其是FT3参与红细胞合成有关[18]。NTIS患者尿素高于对照组,表明NTIS患者处于负氮平衡状态[5],NTIS的发生有益于减少机体代谢,降低消耗,保护机体功能。但NTIS一旦发生,即表明疾病程度严重,预后不良,应引起临床医生的高度重视。另外,NTIS患者的钠及白蛋白低于对照组,D二聚体高于对照组,表明营养差及D二聚体高的患者更容易发生NTIS,其机制还有待进一步研究。
综上所述,本文发现急诊超高龄患者的NTIS发生率极高,而且合并NTIS的急诊超高龄患者常提示患者预后不良,血清FT3水平对于急诊超高龄患者短期死亡有预测作用,超高龄患者入院时常规检测甲状腺功能尤其是血清FT3水平,对患者短期预后有重要预测作用;并且合并脑梗是急诊超高龄患者死亡的独立危险因素;造成这一结果的原因可能是脑梗后患者长期卧床并发感染,容易血栓形成等。因此,对超高龄脑梗患者应积极做好三级预防工作,尤其是合并NTIS的急诊超高龄患者;目前对于合并NTIS的急诊超高龄患者来说,甲状腺激素替代治疗的效果仍存在较大争议[5,19],对于这类患者是否需要补充T3有待进一步研究。
[1] Adler SM, Wartofsky L. The Nonthyroidal Illness Syndrome. Endocrinol Metab Clin N Am, 2007(36): 657-672.
[2] den Brinker M, Joosten KF, Visser TJ, et al. Euthyroid sick syndrome in meningococcal sepsis: the impact of peripheral thyroid hormone metabolism and binding proteins. J Clin Endocrinol Metab, 2005,90(10):5613-5620.
[3] Iltumur K, Olmez G, Ariturk Z, et al. Clinical investigation: thyroid function test abnormalities in cardiac arrest associated with acute coronary syndrome.Critical Care,2005,9(4):416-424.
[4] Hennemann G, Krenning EP.The kinetics of thyroid hormone transporters and their role in non-thyroidal illness and starvation. Best Pract Res Clin Endocrinol Metab,2007,21(2):323-338.
[5] 杨丹英,赵咏桔.老年住院患者正常甲状腺功能病态综合征的发生率及临床特点.中华老年医学杂志,2010,29(4):271-275.
[6] Iglesias P, Muñoz A, Prado F, et al. Alterations in thyroid function tests in aged hospitalized patients: prevalence, aetiology and clinical outcome. Clin Endocrinol (Oxf),2009 ,70(6):961-967.
[7] Pisani MA. Considerations in caring for the critically ill older patient. J Intensive Care Med,2009,24(2):83-95.
[8] Simons RJ, Simon JM, Demers LM, et al. Thyroid dysfunction in elderly hospitalized patients. Effect of age and severity of illness. Arch Intern Med, 1990,150(6):1249-1253.
[9] Corsonello A, Montesanto A, Berardelli M, et al. A cross-section analysis of FT3 age-related changes in a group of old and oldestold subjects, including centenarians' relatives, shows that a downregulated thyroid function has a familial component and is related to longevity. Age Ageing.2010,39(6):723-727.
[10] Tognini S, Marchini F, Dardano A, et al. Non-thyroidal Illness syndrome and short-term survival in hospitalised older population. Age Ageing,2010,39(1):46-50.
[11] Forestier E, Vinzio S, Sapin R, et al. Increased reverse triiodothyronine is associated with shorter survival in independently-living elderly: the Alsanut study. Eur J Endocrinol, 2009, 160(2): 207-214.
[12] Van den Beld AW, Visser TJ, Feelders RA,et al. Thyroid hormone concentrations, disease, physical function, and mortality in elderly men. J Clin Endocrinol Metab, 2005 ,90(12): 6403-6409.
[13] Plikat K, Langgartner J, Buettner R, et al. Frequency and outcome of patients with non-thyroidal illness syndrome in a medical intensive care unit. Metabolism,2007,56(2): 239-244.
[14] Van den Berghe G. Endocrinology in intensive care medicine: new insights and therapeutic consequences. Verh K Acad Geneeskd Belg,2002,64(3): 167-187.
[15] Marsik C, Kazemi-Shirazi L, Schickbauer T, et al. C-reactive protein and all-cause mortality in a large hospital-based cohort. Clinical Chemistry, 2008,54(2): 343-349.
[16] de Rooij SE, Govers A, Korevaar JC, et al. Short-term and longterm mortality in very elderly patients admitted to an intensive care unit. Intensive Care Med,2006,32(7):1039-1044.
[17] Li L, Guo CY, Yang J, et al. Negative association between free triiodothyronine level and international normalized ratio in euthyroid subjects with acute myocardial infarction. Acta Pharmacol Sin,2011,32(11):1351-1356.
[18] Bremner AP, Feddema P, Joske DJ, et al. Significant association between thyroid hormones and erythrocyte indices in euthyroid subjects. Clinical Endocrinology(Oxf), 2012 ,76(2):304-311.
[19] Stathatos N, Wartofsky L.The euthyroid sick syndrome:is there a physiologic rationale for thyroid hormone treatment? J Endocrinol Invest, 2003 ,26(12):1174-1179.
Objective To evaluate the prevalence of Non-thyroidal illness syndrome and its impact on short-term survival in hospitalized super elderly patients. Methods 448 Patients aged more than 80 years in the department of emergency in a religious hospital from January 2014 to January 2015 were enrolled. Patients were divided into NTIS group(n=324)and the control group(n=124)by serum concentration of FT3,the mortality of these two group were compared. Patients were divided into death group(n=48)and survival group(n=400),the rate of NTIS was compared between them. Logistic regression analysis was used to analyze the risk factors for the prognosis of very elderly patients. Results A total of 448 patients were enrolled(age mean±SD,85.6±4.0yrs,198 male and 250 female). The incidence of NTIS was 66.4%.The mortality of NTIS group was higher than the control group(13.6% vs 3.2%,P=0.001),serum level of FT3(Free T3)in non-survivors was lower than survivors(2.0% vs 2.9%,P<0.001);The incidence of NTIS in non-survivors was higher than that in survivors(91.7% vs 70%,P=0.001);FT3<2.75(OR=0.116,95% CI:0.02-0.52)and cerebral infarction(OR=4.49,95%CI:1.83-11.02)were independent risk factors of death for very elderly patients;The best predictor of FT3 for death was 2.605Pmol/L. Conclusions The mortality of NTIS group was higher than control group,serum level of FT3 predicts short-term mortality in hospitalized very elderly patients.
Non-thyroidal illness syndrome,NTIS Very elderly patients Short-term Survival
200233 上海交通大学附属第六人民医院急诊科
