右足腱鞘巨细胞瘤合并左踝毛细血管瘤一例
2016-09-07牛琳黄遥唐威胡箫
牛琳 黄遥 唐威 胡箫
病例报告
右足腱鞘巨细胞瘤合并左踝毛细血管瘤一例
牛琳 黄遥 唐威 胡箫
巨细胞瘤;血管瘤,毛细管;腱;足
腱鞘巨细胞瘤(giant cell tumour of tendon sheath,GCTTS)是一组起源于关节滑膜、滑囊和腱鞘的病变,至今病因不明,好发于手指,发生于足部者少见。毛细血管瘤主要见于婴幼儿皮肤、皮下或黏膜组织,是一种良性的血管性病变,发生于成年人及下肢者少见。国内文献尚未见足部 GCTTS 合并毛细血管瘤的报道。笔者经治 1 例右足 GCTTS 合并左踝毛细血管瘤病变,现报告如下。
临床资料
患者,男,59 岁,因右足背部肿物 9 年余及左外踝肿物 1 年余入院。患者 9 年前无意中发现右足背肿物,约黄豆大小,无痛性,逐渐增大。1 年前新发现左外踝肿物,约黄豆大小,无痛性,逐渐增大。为进一步治疗就诊于我院,影像学检查:(1)双足 X 线片:右足背第 2~3 跖骨区可见软组织肿物影,大小约 5.0 cm×3.5 cm,边界清楚,骨质未见明确破坏征象;(2)右足 MRI:右足背部肿物,以第 2~3 跖骨为中心,局部与第 2 跖骨关系密切,大小约 4.5 cm×3.2 cm×2.6 cm,T1WI 低信号,T2WI / FS 中高信号,增强扫描不均匀明显强化,可见足底动脉分支进入,考虑恶性肿瘤可能大;左足 MRI:左踝部肿物,局部突起于皮下,大小约 2.7 cm×2.7 cm×1.8 cm,边界清楚,T1WI 稍低信号,T2WI / FS 中高信号,增强扫描呈渐进式强化,考虑为良性或潜在恶性病变。
治疗过程:首先在局麻下行“右足背肿物、左外踝肿物切开活检术”,病理提示:左踝部肿物为毛细血管瘤,右足背肿物形态符合 GCTTS。遂在全麻下行“左外踝肿瘤、右足背肿瘤切除术”,术中见右足背前方第 2、3、4 跖骨表面有一肿物隆起,大小约 6 cm×5 cm×4 cm,包膜完整,质韧,未累及皮肤,包绕第 2、3 趾长伸肌腱和第 2、3 趾短伸肌及其肌腱,深面贴临第 2、3 跖骨和第2、3 跖趾关节囊,并向深面突入第 2、3 跖骨间隙。左外踝肿物:大小约 4.0 cm×3.0 cm×2.0 cm,分叶状,包膜完整,质韧,位于左外踝前方第 3 腓骨肌腱和趾长伸肌腱深面,并包绕前者,肿瘤深面贴邻跟距关节囊、距舟关节囊和跟周关节囊。
左踝部肿物免疫组化提示:CD31(1+),CD34(血管 +),CD68(1+),S-100(-),NF(-),SMA(-),Ki-67(<5%),术后病理回报:左外踝肿物考虑毛细血管瘤,右足背肿物考虑 GCTTS(图 1、2)。
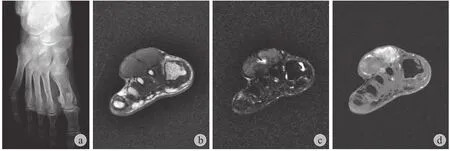
图1 右足腱鞘巨细胞瘤 a:右足X 线片示第 2~3 跖骨区软组织肿物影,边界清楚,未见明确骨质破坏征象;b:T1WI 低信号;c:T2WI / FS 中高信号;d:AXT1+ C 增强扫描不均匀明显强化Fig.1 Tenosynovial giant cell tumor of the right foot a: X-ray showed that a circumscribed tumor between second and third metatarsal bone areas, with no obvious bone destruction; b: The transverse T1-weighted MR image showed low signal intensity; c: The transverse T2-weighted -FS MR image showed slightly hyper signal intensity;d: The transverse T1enhanced-MRimage showed obvious inhomogeneous enhancement
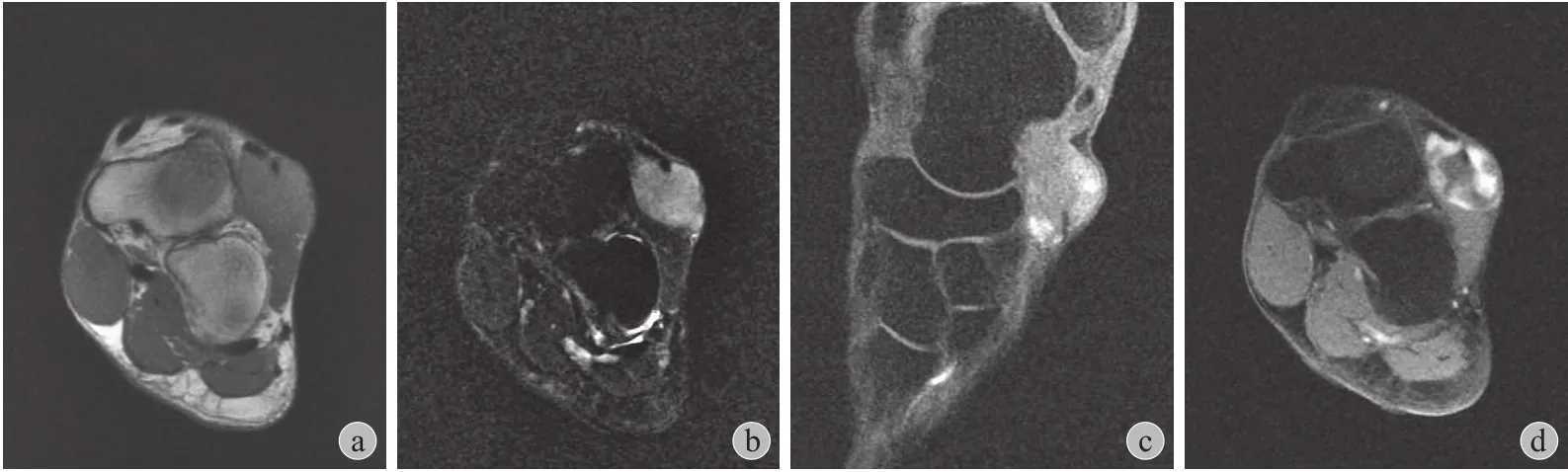
图2 左踝毛细血管瘤a:左踝部肿物,T1WI 稍低信号;b:T2WI / FS 中高信号;c~d:增强扫描呈渐进式明显强化Fig.2 Capillary hemangioma of the left foot a: A lesion of the left ankle, with slightly low signal intensity in transverse T1-weighted MR image; b: The transverse T2-weighted-FS MR image showed slightly hyper signal intensity; c - d: The enhanced-MR image showed obvious gradual enhancement
讨 论
GCTTS 于 1941 年被首次报道,该病通常是一种起源于腱鞘、滑囊和关节滑膜的良性肿瘤,发病机制及病因目前尚不明确,有学者认为其可能与脂质类代谢异常、关节反复外伤积血、慢性炎症等有关。根据发病部位及生物学行为的不同,GCTTS 分为局灶型和弥漫型两种,局灶型最为常见,约占总数的 85%,好发于 30~50 岁,男女比例为 2∶3,通常表现为无痛性、生长缓慢的肿块,绝大多数发生于指、趾关节附近,最常见于手指,发生于足部者少见[1-5]。毛细血管瘤是良性的血管性病变,好发于头颈部,主要见于婴幼儿皮肤、皮下或黏膜组织,发生于成年人及下肢者少见,而发生于足部者文献报道更不足10 例[6]。本例为男性,59 岁,同时患有右足部 GCTTS 及左踝部毛细血管瘤,十分罕见。
影像学方面,GCTTS 传统 X 线片检查价值有限,约50% 的患者可见软组织肿物影,偶尔可伴发骨质破坏、骨膜反应等,但无法显示关节滑膜以及关节内的情况,而CT 检查对于骨质受累的显示要优于其它影像检查方法,MRI 因为有较高的软组织分辨率,有助于 GCTTS 的诊断,部分病例呈现出 T1、T2特征性低信号,多数学者认为这与含铁血黄素的顺磁性效应有关,由于 GCTTS 是富含毛细血管的肿物,肿瘤反复出血可导致含铁血黄素沉积,进而呈现出特异性的 MRI 信号[3,7]。毛细血管瘤 CT 表现为边界清楚的低密度肿物,增强扫描明显强化,MRI 表现为T1低信号,T2高信号[8],但关于软组织毛细血管瘤的影像学相关文献报道较少,多数病变因发病部位表浅常行手术切除而确诊。本例右足病变骨 X 线片可见软组织肿物影,未见明确骨质破坏征象,MRI 未出现特征性 T2信号,表现不典型;左踝部病变 MRI 表现为 T1低信号,T2中高信号,增强扫描强化较为明显,可符合血管瘤表现。
免疫组化方面,GCTTS 由于富含多种细胞成分因而表现多样,如 desmin、CD68、CD163 及 CD45 等染色均可呈阳性。而毛细血管瘤由于富含血管内皮细胞,而表达多种特异性内皮标志如 CD34 和 CD31 等。本例右足病变未行免疫组化染色,左踝部病变 CD31(+)、CD34(血管 +),与文献报道相符[9]。
尽管两者均为良性病变,但完整的手术切除是必不可少的。文献报道 GCTTS 术后复发率从 4%~44% 不等,完整切除者复发率为 7.70%,次全切除者复发率为 66.75%,因此完整切除已经成为该病公认的最好的治疗方式,可以显著降低复发风险[7]。而皮肤或软组织的毛细血管瘤因常见复发,也需要完整的手术切除[10]。
[1] Di Grazia S, Succi G, Fraggetta F, et al. Giant cell tumor of tendon sheath: study of 64 cases and review of literature. G Chir, 2013, 34(5-6):149-152.
[2] Doita M, Miyamoto H, Nishida K, et al. Giant-cell tumor of the tendon sheath involving the thoracic spine. J Spinal DisordTech, 2005, 18(5):445-448.
[3] Goni V, Gopinathan NR, Radotra BD, et al. Giant cell tumour of peroneus brevis tendon sheath-a case report and review of literature. BMJ Case Rep, 2012, 2012.
[4] Suresh SS, Zaki H. Giant cell tumor of tendon sheath: case series and review of literature. J Hand Microsurg, 2010, 2(2):67-71.
[5] WHO classification of tumours of soft tissue and bone. IARC Press, 2013, 99-102.
[6] Cione JA, Cozzarelli J. Capillary hemangioma of the foot. J Am Podiatr Med Assoc, 2002, 92(3):155-157.
[7] Wang K, Zhu B, Yang S, et al. Primary diffuse-type tenosynovial giant cell tumor of the spine: a report of 3 cases and systemic review of the literature. Turk Neurosurg, 2014, 24(5):804-813.
[8] Jhuang JY, Lin LW, Hsieh MS. Adult capillary hemangioma of the liver: case report and literature review. Kaohsiung J Med Sci, 2011, 27(8):344-347.
[9] Guo R, Folpe AL. Extensively Myxoid and Hyalinized Sinonasal Capillary Hemangiomas: A Clinicopathologic Study of 16 Cases of a Distinctive and Potentially Confusing Hemangioma Variant. Am J Surg Pathol, 2015, 39(11):1584-1590.
[10] Vavallo A, Lafranceschina F, Lucarelli G, et al. Capillary hemangioma of the scrotum mimicking an epididymal tumor:Case report. Arch Ital Urol Androl, 2014, 86(4):395-396.
(本文编辑:李贵存)
Tenosynovial giant cell tumor of the right foot with capillary hemangioma of the left foot: 1 case report
NIU Lin, HUANG Yao, TANG Wei, HU Xiao. Department of Diagnostic Radiology, Cancer Hospital, Chinese Academy of Medical Sciences, Beijing, 100021, PRC
HUANG Yao, Email: huangyao93@163.com
Tenosynovial giant cell tumor is a benign soft tissue tumor arising from the synovia of the fibrous tissues surrounding the joints, tendon sheaths, mucosal bursas. It is mostly found in the hand and wrist and rarely observed in the foot. Capillary hemangiomas are benign vascular lesions, most often found in the cutaneous,subcutaneous, or mucosal tissues in the childhood. The report of capillary hemangiomas in the foot is especially uncommon and the number of papers is less than 10. In this case, we presented an elderly man who was diagnosed with tenosynovial giant cell tumor of the right foot and capillary hemangioma of the left foot. He had masses for 9 year on the back of the right foot and 1 year in the left external ankle without any reasons. He received surgical excision of masses, which is the imperative treatment strategy and could reduce the recurrence rate. Also, we presented a brief literature review of the tenosynovial giant cell tumor and capillary hemangioma.
Giant cell tumors; Hemangioma, capillary; Tendons; Foot
10.3969/j.issn.2095-252X.2016.08.017 中图分类号:R738.5
100021 北京,中国医学科学院肿瘤医院影像诊断科
黄遥,Email: huangyao93@163.com
(2016-02-05)