81例老年阻塞性睡眠呼吸暂停低通气综合征临床特点分析*
2016-06-15李忠万杨贵军方红雁李晓晓廖修富李劲松
李忠万,杨贵军,方红雁,李晓晓,廖修富,李劲松
(重庆市人民医院耳鼻咽喉头颈外科/重庆市眼耳鼻咽喉科医院 400014)
81例老年阻塞性睡眠呼吸暂停低通气综合征临床特点分析*
李忠万,杨贵军,方红雁,李晓晓,廖修富,李劲松△
(重庆市人民医院耳鼻咽喉头颈外科/重庆市眼耳鼻咽喉科医院400014)
[摘要]目的探讨老年阻塞性睡眠呼吸暂停低通气综合征(OSAHS)与中年OSAHS临床特点和多导睡眠监测特征的差异,为诊断及个体化干预老年 OSAHS提供参考依据。方法分析81例老年OSAHS 和123例中年OSAHS的一般情况、临床表现和多导睡眠图特点,并按BMI匹配比较两组临床表现及多导睡眠指标差异。结果老年及中年OSAHS患者均以男性居多,老年组BMI及颈腹围均小于中年组(P<0.05),而胸围大于中年组(P>0.05)。老年组的临床症状如嗜睡、打鼾、晨起头痛、口干及夜间憋醒发生率均低于中年组,差异具有统计学意义(P<0.05),而并发症如高血压、糖尿病等患病率明显高于中年组,差异具有统计学意义(P<0.05)。老年组OSAHS患病程度主要分布于轻中度,中年组主要分布于中重度,但差异无统计学意义(P>0.05)。REM期AHI老年组大于中年组(P<0.05),AHI低于中年组(P<0.05);NREMⅠ+Ⅱ期大于中年组,差异有统计学意义(P<0.05);而NREM Ⅲ+Ⅳ期、REM期、平均SaO2(%)、MAI小于中年组,LSAT(%)大于中年组,但差异均无统计学意义(P>0.05)。结论老年OSAHS患者典型临床表现的发生率低于中年组,然而高血压、糖尿病等并发症患病率明显高于中年组,二者OSAHS严重程度相近,PSG监测结果与中年组存在差异,且REM期AHI与中年组差异明显。
[关键词]睡眠呼吸暂停,阻塞性;低通气综合征;多导睡眠图;特征
阻塞性睡眠呼吸暂停低通气综合征(Obstructive sleep apnea hypernea symptom,OSAHS)是具有潜在危险性的常见病、慢性病,以睡眠期反复的呼吸暂停、低通气和微觉醒为特征。主要临床表现为打鼾且鼾声不规律、日间嗜睡、晨起口干、头痛及夜尿增多等。老年OSAHS可以是中年发病OSAHS的延续,也可以是老年新发的OSAHS。现有研究表明,不同发病年龄组的OSAHS 患者具有不尽相同的临床表现及多导睡眠图检查(PSG)监测结果,但尚未达成共识,这可能与不同年龄段的身体机能的变化有关。如Chung等[1]报道老年OSAHS患者因上呼吸道塌陷以致呼吸暂停频率增高,且持续时间变长。随着社会老龄化的进展,老年OSAHS的诊治成为了维护老年人健康的重要方面。有针对性的发现并提出适合老年患者的诊治标准将为及时准确的诊断及治疗带来方便。本研究将老年性患者与中年患者的临床表现PSG结果对比分析如下。
1资料与方法
1.1一般资料研究对象为2011年6月至2015年2月在本院行PSG,就诊年龄大于或等于45岁的患者。纳入习惯性打鼾且确诊OSAHS的患者,剔除既往行无创正压通气(continuous positive airway pressure,CPAP)治疗的OSAHS患者,无法明确发病年龄者(如独自居住),脑梗死、脑出血、心功能衰竭、呼吸衰竭者。
1.2方法对所有对象行一般体格检查,包括身高、体质量、颈围、胸围、腹围。指派专人行问卷调查,包括一般资料、打鼾史、呼吸暂停病史等,并应用嗜睡评估表(ESS)进行嗜睡评分。夜间7 h以上PSG检查,PSG监测项目包括脑电、眼电、心电、下颌肌电、口鼻气流、胸腹运动、血氧饱和度、体位、鼾声,记录数据经软件分析后由专人进行人工校正。多导睡眠监测系统为Australia compumedics limited公司的E-series PSG监测系统。根据患者发病年龄分为以下两组,老年组:发病年龄大于或等于60岁的OSAHS患者81例;中年组:发病年龄45~60岁的OSAHS患者123例。依据我国2011年阻塞性睡眠呼吸暂停低通气综合征诊治指南(修订版)[2]:即每晚7 h睡眠中呼吸暂停及低通气反复发作30次以上或AHI≥5次/h,呼吸暂停以阻塞性为主,诊断为OSAHS,当AHI为5~15属轻度,>15~30属中度,>30属重度。同时监测脑电图、眼动图、颏肌电图、口鼻呼吸(热敏传感器)、鼾声、胸式呼吸、腹式呼吸、体位、经皮血氧饱和度和心电图等。PSG监测的数据于次日由同一人进行电脑分析及人工整理。
1.3定义及诊断标准白天嗜睡评定:利用ESS,患者根据自己的主观感觉评价在8种不同情况下打盹的可能性。参考国际嗜睡评定标准,将 ESS>8分定义为嗜睡。对打鼾程度的评价:轻度打鼾,较健康人呼吸声音粗重;中等度打鼾,鼾声响亮程度大于普通人说话声音;重度打鼾,鼾声响亮以至同一房间的人无法入睡。高血压:在未使用降压药物的情况下,非同日3次测量血压,收缩压大于或等于140 mm Hg和(或)舒张压大于或等于90 mm Hg;既往在医院明确诊断的高血压及已服药治疗的高血压患者。 颈围:受试者清醒垂直站立位,平视前方,紧贴其喉结下缘(环甲膜水平)使用软尺平绕一周所得周径。 胸围:患者自然站立,双肩放松,两臂自然下垂,两足分幵与肩同宽,保持平静呼吸。检测人员面对受检者,将带尺上缘经背部肩胛下角下缘至胸前沿乳头上缘,软尺围绕胸部的松紧度应适宜,带尺上与“0”点相交的数值即为测量值。记录以cm为单位,精确到0.1。腹围:将软尺经脐上0.5~1.0 cm处水平绕一周,肥胖者选腰部最粗处水平绕一周所得周径。

2结果
2.1两组患者一般情况比较老年及中年OSAHS患者中均以男性居多,但老年组与中年组男女比例无差异(P>0.05),老年患者BMI及颈腹围均小于中年(P<0.05),而胸围大于中年(P>0.05),见表1。

表1 两组患者一般情况比较
2.2两组患者临床表现比较老年组的临床症状如嗜睡、打鼾、晨起头痛、口干及夜间憋醒发生率均低于中年组,差异具有统计学意义(P<0.05),而并发症如高血压、糖尿病、冠心病、脑血管疾病等患病率明显高于中年组,差异具有统计学意义(P<0.05),见表2。
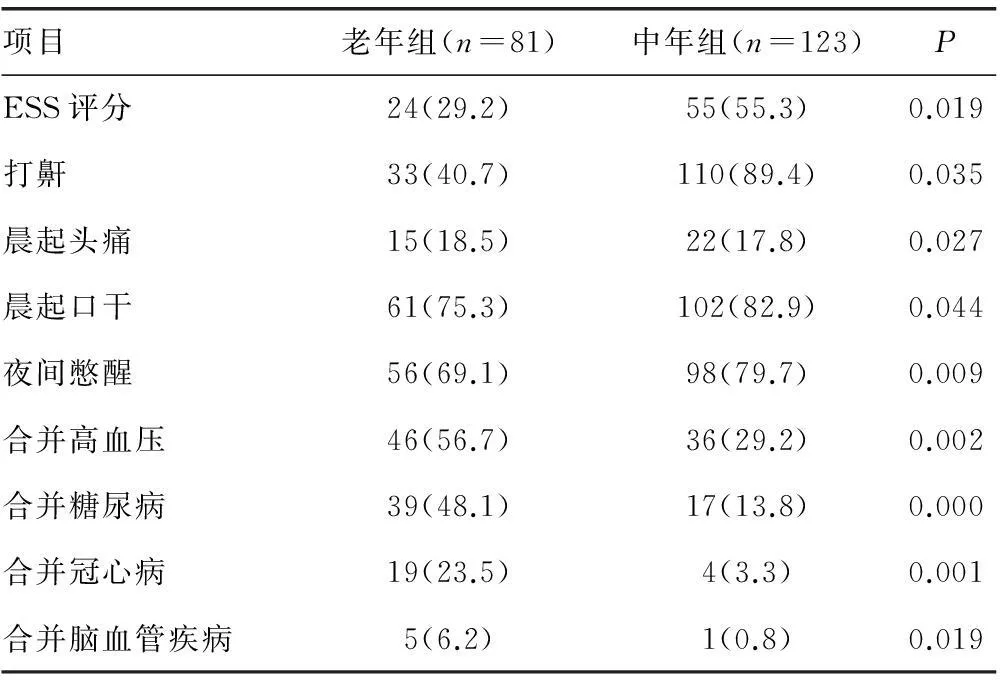
表2 两组临床表现及合并疾病比较[n(%)]
2.3两组患者病情程度比较老年组OSAHS患病程度主要分布于轻中度,中年组主要分布于中重度,但差异无统计学意义(P>0.05),见表3。

表3 两组OSAHS病情程度[n(%)]
表4 两组患者PSG结果比较
2.4两组患者 PSG结果比较REM期AHI老年组大于中年组,AHI低于中年组,NREMⅠ+Ⅱ期大于中年组,差异有统计学意义(P<0.05)。而老年组NREMⅢ+Ⅳ期、REM期、平均SaO2(%)、MAI小于中年组,LSAT(%)大于中年组,但差异均无统计学意义(P>0.05),见表4。
3讨论
近年来OSAHS发病率呈上升趋势,因其可引起机体多种疾病,进而损害全身多系统、多器官功能。Lee等[3]研究发现OSAHS在某种程度上增加了韩国人的死亡率,从而引起了人们的重视。本研究发现老年人单纯因OSAHS症状前来就诊的就诊率低。本研究病例在很大程度上来源于心血管、呼吸等相关科室的会诊或转诊病人。老年患者临床症状如嗜睡、打鼾、晨起头痛、口干及夜间憋醒发生率均低于中年组,而并发症如高血压、糖尿病、冠心病、脑血管疾病等患病率明显高于中年组。出现这样的结果是否因为老年患者对OSAHS的认识不够,未及时就诊,常常在多种全身疾病引起相关并发症时才被重视。有研究还表明,随着年龄的增加其发病率升高[4]。Gabbay等[5]报道老年OSAHS发病率高于中青年,但Bixler等[6]及Bielicki等[7]报道随着年龄的增加严重程度逐渐减轻。Kobayashi等[8]认为老年患者较中青年患者严重程度降低可能与老年患者对呼吸反射敏感性降低有关。本研究老年OSAHS患者的BMI、颈、胸、腹围均小于中年,但除胸围以外,另外3项差异均具有统计学意义(P<0.05)。一般情况在OSAHS的发病及治疗方面起着重要作用,Tuomilehto等[9]研究发现,对于肥胖患者持续而适度的减轻体质量可明显减轻OSAHS症状,甚至可以治愈轻度OSAHS。Dacal等[10]等研究发现在正常体质量的人群中以年轻女性患者居多。可见患者的一般情况在诊治中的重要作用。主要临床特点ESS、高血压、打鼾、晨起头痛、晨起口干及夜间憋醒出现率均低于中青年组,差异具有统计学意义。OSAHS严重程度老年组与中年组均以中度为主,但老年组重度患病率明显低于中青年组,与Bixler等[6]及李兵等[11]报道相符合,但尚不能确定是否由年龄变化进而引起身体因素的变化有关。
OSAHS的诊断目前主要依靠PSG监测结果及临床症状,然而Rosen等[12]提出对儿童OSAHS患者采用睡眠问卷通过对临床症状的评分来了解OSAHS程度得到了一定程度的认可。Borges等[13]研究发现从下颌平面和舌骨之间的距离,以及后鼻棘和软腭的前端之间的距离加上颈围与腰围,仅与40~60岁的OSAHS患者有相关性。PSG作为诊断OSAHS的重要手段,其已在临床中广泛应用,然而针对老年人的诊治指标尚未达成共识。本研究结果显示,REM期AHI指数为40.19±12.39,明显高于中年组的34.07±15.04,差异具有统计学意义,然而整个睡眠的期的AHI老年组为29.1±19.27,中年组为38.33±20.11,老年组明显低于中青年组,差异具有统计学意义,统计表明老年患者出现睡眠呼吸暂停主要集中在REM期,Yamaguchi等[14]也发现引起女性OSAHS患者出现呼吸暂停主要在REM期,是否将REM期的AHI作为诊断老年患者OSAHS的特异性指标尚有待进一步研究,Guo等[15]已以对慢性动眼睡眠期的PSG结果与嗜睡等症状进行了相关性研究,发现此期与嗜睡关系密切。NREMⅠ+Ⅱ期为主,明显高于Ⅲ+Ⅳ,这说明不同睡眠时期的睡眠结构差异较大,分期对老年OSAHS患者进行诊治似乎更具有意义。平均SaO2、LSAT及MAI老年组与中年组无明显差,与罗淼等[16]报道的SaO2老年组高于中青年组不一致,这可能与纳入标准的地域差异有关。
我们认为OSAHS严重影响老年患者的生活质量,且增加其死亡率,应当重视老年OSAHS的早期诊断与治疗,其诊断应结合老年患者特异的PSG结果及其临床表现,以期为其诊治提供更好的依据。
参考文献
[1]Chung S,Yoon IY,Lee CH,et al.Effects of age on the clinical features of men with obstructive sleep apnea syndrome[J].Respiration,2009,78(1):23-29.
[2]中华医学会呼吸病学分会睡眠呼吸障碍学组.阻塞性睡眠呼吸暂停低通气综合征诊治指南(2011年修订版)[J].柳州医学,2012,35(3):162-165.
[3]Lee JE,Lee CH,Lee SJ,et al.Mortality of patients with obstructive sleep apnea in Korea[J].J Clin Sleep Med,2013,9(10):997-1002.
[4]Lurie A.Obstructive sleep apnea in adults:epidemiology,clinical presentation,and treatment options[J].Adv Cardiol,2011,46(1):1-42.
[5]Gabbay IE,Lavie P.Age- and gender-related characteristics of obstructive sleep apnea[J].Sleep Breathing,2012,16(2):453-460.
[6]Bixler EO,Vgontzas AN,Ten Have T,et al.Effects of age on sleep apnea in men:I.Prevalence and severity[J].Am J Respir Crit Care Med,1998,157(1):144-148.
[7]Bielicki P,Byskiniewicz K,Kumor M,et al.Obstructive sleep apnoea syndrome in younger and older age groups--differences and similarities[J].Pneumonol Alergol Pol,2006,74(1):56-58.
[8]Kobayashi M,Namba K,Tsuiki S,et al.Clinical characteristics in two subgroups of obstructive sleep apnea syndrome in the elderly:comparison between cases with elderly and middle-age onset[J].Chest,2010,137(6):1310-1315.
[9]Tuomilehto H,Seppä J,Uusitupa M,et al.The impact of weight reduction in the prevention of the progression of obstructive sleep apnea:an explanatory analysis of a 5-year observational follow-up trial[J].Sleep Med,2014,15(3):329-335.
[10]Dacal Quintas R,Tumbeiro Novoa M,Alves Pérez MT,et al.Obstructive sleep apnea in normal weight patients:characteristics and comparison with overweight and obese patients[J].Archivos Bronconeumol,2013,49(12):513-517.
[11]李兵,张峰,余林.老年OSAHS患者多导睡眠监测结果分析及临床意义[J].第三军医大学学报,2007,29(20):1994-1995.
[12]Rosen CL,Wang R,Taylor HG,et al.Utility of symptoms to predict treatment outcomes in obstructive sleep apnea syndrome[J].Pediatrics,2015,135(3):e662-671.
[13]BorgesPdeT,DaSilvaBB,MoitaNeto
JM,et al.Cephalometric and anthropometric data of obstructive apnea in different age groups[J].Braz J Otorhinolaryngol,2015,81(1):79-84.
[14]Yamaguchi K,Inoue Y,Ohki N,et al.Gender-specific impacts of apnea,age,and BMI on parasympathetic nerve dysfunction during sleep in patients with obstructive sleep apnea[J].PLoS One,2014,9(3):e92808.
[15]Guo J,Xiao Y,Huang R,et al.Slow eye movement analysis in patients with obstructive sleep apnea/hypopnea syndrome[J].Zhonghua Jie He He Hu Xi Za Zhi,2014,37(2):89-94.
[16]罗淼,李涛平,冯媛,等.老年与中青年阻塞性睡眠呼吸暂停低通气综合征患者临床表现和多导睡眠特征的差异[J].中国呼吸与危重监护杂志,2012,11(5):489-493.
The clinical characteristics of elderly patients with obstructive sleep apnea hypopnea syndrome*
Li Zhongwan,Yang Guijun,Fang Hongyan,Li Xiaoxiao,Liao Xiufu,Li Jinsong△
(Department of Otolaryngology Head and Neck Surgery,the Third People′s Hospital of Chongqing/EyeEar Nose and Throat Hospital of Chongqing,Chongqing 400014,China)
[Abstract]ObjectiveTo discuss the differences of clinical features and characteristics and features of polysomnography between elderly patients and middle-aged patients with obstructive sleep apnea hypopnea syndrome (OSAHS),so as to provide reference for the diagnosis and individualized intervention of elderly OSAHS.MethodsTotally 81 aged OSAHS cases and 123 youth OSAHS cases were analyzed in terms of general condition,clinical manifestations and polysomnographic characteristics,and the clinical manifestations and polysomnographic difference indicators of the two groups were matched according to body mass index (BMI).ResultsMost OSAHS patients were males in both groups,with BMI and neck waist circumference in the aged group less than those in the middle-aged group,and the difference was statistically significant (P<0.05),while the bust was larger than that in the middle-aged group,but the difference was not statistically significant (P>0.05);clinical symptoms of senile groups such as drowsiness,snoring,morning headaches,dry mouth and nighttime awakenings were lower than the middle-aged group,the difference was statistically significant (P<0.05),and complications such as hypertension,diabetes and other risk disease were significantly higher than those in the middle-aged group,and the difference was statistically significant (P<0.05);in the aged group,the degree of OSAHS was dominated by mild to moderate,while the middle-aged group,was dominated by moderate to severe,but the difference was not statistically significant (P>0.05);REM AHI was more than the middle-aged group,the difference was statistically significant (P<0.05),AHI was less in old age group than in the middle-aged group,the difference was statistically significant (P<0.05);NREMⅠ+Ⅱ stage in the aged group was more than that in the middle-aged group(P<0.05),and NREM Ⅲ+Ⅳ stage,REM period,the average SaO2 (%),MAI clear were less than those in the young group;LSAT (%) was greater than that in the middle-aged group,but the difference was not statistically significant (P>0.05).ConclusionThe incidence of typical clinical manifestations of aged OSAHS patients was lower than that in the middle-aged group,but high blood pressure,diabetes and other complications prevalence were significantly higher than those in the middle-aged group,with similar severity of OSAHS in both groups,there were differences PSG monitoring results with the middle-aged group,and the difference of REM AHI was significant.
[Key words]sleep apnea,obstructive;hypopnea syndrome;polysomnography;characteristics
doi:论著·临床研究10.3969/j.issn.1671-8348.2016.11.014
* 基金项目:重庆市卫生局医学科学技术研究项目(2012-2-224)。
作者简介:李忠万(1976-),副主任医师,硕士,主要从事头颈外科方面研究。△通讯作者,E-mail:402681589@qq.com。
[中图分类号]R766.9
[文献标识码]A
[文章编号]1671-8348(2016)11-1488-03
(收稿日期:2015-11-14修回日期:2016-01-07)
