炎症性肠病结肠隆起型异型增生影响因素的回顾性研究
2016-03-02李俊霞刘冠伊王化虹刘新光
田 雨,李俊霞,田 原,刘冠伊,王化虹,刘新光
作者单位:100034 北京市,北京大学第一医院消化内科
·论著·
炎症性肠病结肠隆起型异型增生影响因素的回顾性研究
田 雨,李俊霞,田 原,刘冠伊,王化虹,刘新光
作者单位:100034 北京市,北京大学第一医院消化内科
【摘要】背景随着我国炎症性肠病发病率的上升,炎症性肠病相关结直肠癌及癌前病变的发病情况值得关注。目的探讨炎症性肠病结肠隆起型异型增生发生的相关影响因素。方法选取2007年1月—2014年1月在北京大学第一医院进行内镜随访的393例炎症性肠病患者为研究对象,收集患者临床资料和病理学检查结果。以发生结肠隆起型异型增生为结局事件,以患者的病程为时间变量,采用Cox比例风险回归分析炎症性肠病患者结肠隆起型异型增生发生的影响因素。结果393例炎症性肠病患者中13例发生结肠隆起型异型增生,其中溃疡性结肠炎12例、克罗恩病1例;腺瘤样病变或肿物(ALM)10例、异型增生相关病变或肿物(DALM)3例。Cox比例风险回归模型结果显示,炎症性肠病家族史、疾病活动程度和疾病复发情况与结肠隆起型异型增生有回归关系(P<0.05);性别、起病年龄、结肠癌家族史、吸烟、病变范围和接受至少2年以上的5-氨基水杨酸(5-ASA)/柳氮磺胺吡啶(SASP)维持治疗与结肠隆起型异型增生无回归关系(P>0.05)。Log-rank检验结果显示,无炎症性肠病家族史者、中度活动者及疾病偶发患者的累计生存率高于有炎症性肠病家族史者、重度活动者及疾病频发/持续活动患者(χ2值分别为4.631、7.382、13.438,P值分别为0.031、0.007、<0.001)。10例ALM患者中9例行内镜下黏膜切除、1例多发ALM患者行全结肠切除;3例DALM患者1例行全结肠切除,2例因病情较重或全身情况差未行手术治疗。结论炎症性肠病患者结肠隆起型异型增生的发生率随着病程的延长而增加;影响其发生的高危因素有炎症性肠病家族史、疾病活动程度和疾病复发情况。
炎症性肠病包括溃疡性结肠炎和克罗恩病,两者有着较正常人群更高的罹患结肠恶性肿瘤的风险[1],这些患者结肠镜随访的目的之一是发现癌前病变或早期可治愈的结肠癌[2]。目前通常认为,炎症性肠病患者结肠癌的发生经历了从反复炎症到异型增生再到癌变的过程[3]。炎症性肠病患者结肠的异型增生是炎症性肠病相关结直肠癌(colorectal cancer,CRC)的重要预测因素。炎症性肠病患者结肠的异型增生根据内镜下表现可分为平坦型异型增生和隆起型异型增生,前者的发现是通过结肠镜随机活检病理检查发现的,而后者可以通过内镜肉眼发现可疑病变,活检病理加以证实。其中隆起型异型增生又可分为腺瘤样病变或肿物(adenoma-like lesion or mass,ALM)和异型增生相关病变或肿物(dysplasia associated lesion or mass,DALM)[4]。本研究回顾性分析北京大学第一医院进行了完整随访的炎症性肠病患者的临床资料和内镜资料,探讨炎症性肠病患者结肠隆起型异型增生发生的影响因素。
1资料与方法
1.1临床资料选取2007年1月—2014年1月在北京大学第一医院进行至少一次完整随访(包括结肠镜、病理学检查)的炎症性肠病患者393例为研究对象,炎症性肠病的诊断符合《炎症性肠病诊断与治疗的共识意见(2012年·广州)》[5]的诊断依据。其中男208例,女185例,男女比1∶1.1;起病年龄1~75岁,平均起病年龄(38.4±15.1)岁;病程1~65年,平均病程(8.9±7.8)年;溃疡性结肠炎306例,克罗恩病87例;具有炎症性肠病家族史22例(5.6%);具有结肠癌家族史7例(1.8%);吸烟88例(22.4%);溃疡性结肠炎广泛受累(E3)和克罗恩病结肠受累(L2)174例(44.3%);疾病活动程度为重度活动140例(35.6%);疾病复发情况为疾病频发/持续活动54例(13.7%);接受至少2年以上的5-氨基水杨酸(5-ASA)/柳氮磺胺吡啶(SASP)维持治疗224例(57.0%);无合并原发性硬化性胆管炎(primary sclerosing cholangitis,PSC)患者。
1.2资料收集收集患者的性别、起病年龄、病程、本研究背景和创新点:
国外研究已证实,炎症性肠病是结肠癌的高危因素。近年来,炎症性肠病在我国的发病率有逐年递增的趋势,随着患者数量的增加和病程的增长,此类患者肠道肿瘤发生的情况已经日益显现。目前我国炎症性肠病相关结肠癌的研究数据有限,我国炎症性肠病发生结肠癌及癌前病变的概率是多少?与何因素相关?药物治疗是否能起到预防作用?等问题均需用循证医学的数据来解答。本研究采取回顾性的研究方法,分析了炎症性肠病结肠隆起型异型增生的发生情况,寻找炎症性肠病患者发生结肠癌及癌前病变的相关因素。虽然受到病例数量、研究方法和仅探讨了结肠隆起型异型增生等限制,此项研究仍然为临床医生筛选高危患者、指导治疗和随访提供了重要依据。
炎症性肠病类型、家族史(炎症性肠病、结肠癌)、吸烟情况(吸烟指连续或累计吸烟6个月或以上者,无论是否已经戒烟)、病变范围(根据蒙特利尔分类/型确定E3和L2)、疾病活动程度〔溃疡性结肠炎和克罗恩病分别采用改良Mayo评分和简化克罗恩病疾病活动指数(CDAI)评分,以改良Mayo评分≥6分和简化CDAI评分≥9分为重度活动〕、疾病复发情况(溃疡性结肠炎和克罗恩病患者症状再次出现,且改良Mayo评分>2分和简化CDAI评分>4分为疾病复发;当复发频率≥2次/年时为疾病频发,当患者症状持续不缓解时为持续活动)[5]、接受至少2年以上的5-ASA/SASP维持治疗情况、合并PSC情况等临床资料,同时收集其结肠镜、病理学检查结果。
1.3结肠隆起型异型增生的确定炎症性肠病患者结肠镜检查发现隆起病变处后,活检1块或多块,其中9例患者采用内镜下黏膜切除(endoscopic mucosal resection,EMR),2例经结肠镜活检病理诊断为异型增生者行全结肠切除,手术切除标本进行病理诊断。
结肠隆起型异型增生的病理学改变由病理科医师和消化科医师会诊,参考文献[6]加以判定,分为ALM和DALM,主要根据病变受累肠段,异型增生的程度,黏膜层中性粒细胞、淋巴细胞的浸润程度,腺体形态改变以及有无绒毛成分等综合考虑判定。异型增生根据维也纳标准[7]分为轻度异型增生(light grade dysplasia,LGD)和重度异型增生(high grade dysplasia,HGD)。
1.4结肠隆起型异型增生患者的随访对判断为结肠隆起型异型增生的患者,继续对其进行随访,包括异型增生的处理以及其复发情况。对接受内镜下治疗的患者3个月内复查结肠镜并做病理学检查。

2结果
2.1患者的一般情况393例炎症性肠病患者中13例发生结肠隆起型异型增生,其中男8例,女5例,男女比1∶1.6;起病年龄17~53岁,平均起病年龄(46.5±16.5)岁;病程8~40年,病程中位数为11年;溃疡性结肠炎 12例,克罗恩病1例;具有炎症性肠病家族史2例(15.4%);具有结肠癌家族史1例(7.7%);吸烟6例(46.2%);E3和L2 10例(76.9%);疾病活动程度为重度活动10例(76.9%);疾病复发情况为疾病频发/持续活动10例(76.9%);接受至少2年以上的5-ASA/SASP维持治疗10例(76.9%);无合并PSC患者;ALM 10例,DALM 3例;LGD 10例,HGD 3例。结肠隆起型异型增生的内镜下表现为,在病变肠段生长,大小0.5~3.0 cm,扁平或亚蒂的隆起病变,部分隆起型异型增生呈结节状,多数表面有充血,少数肿物表面有糜烂(见图1~4,本文图1~8等彩图见本刊官网www.chinagp.net电子期刊相应文章附件)。
2.2结肠隆起型异型增生的处理和随访结果10例ALM患者中9例行EMR,病理学检查分别为管状腺瘤Ⅰ~Ⅱ级,LGD;锯齿状腺瘤Ⅰ~Ⅱ级,LGD;增生性息肉合并管状腺瘤,LGD。3个月后随访结肠镜检查和病理学检查患者病变部位均未发现复发。1例多发ALM患者行全结肠切除,术后病理学检查为结肠多发绒毛-管状腺瘤、LGD。3例DALM患者1例行全结肠切除,术后病理学检查为管状腺瘤Ⅲ级、HGD;2例因病情较重或全身情况差未行手术治疗(见表1、图5~8)。
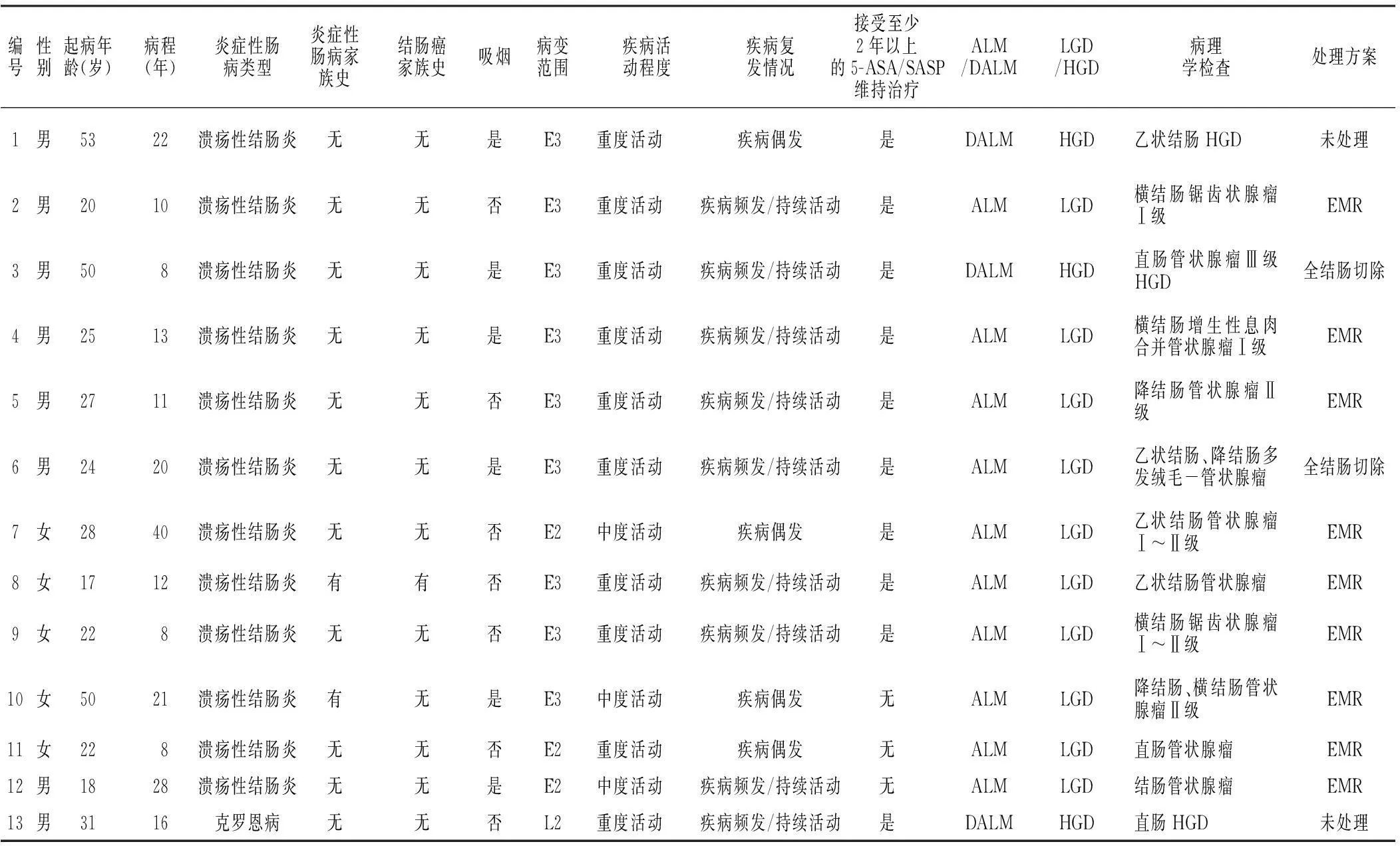
表1 13例炎症性肠病结肠隆起型异型增生患者的临床资料和病理改变
注:E3=溃疡性结肠炎广泛受累,E2=溃疡性结肠炎左半结肠型,L2=克罗恩病结肠受累,5-ASA=5-氨基水杨酸,SASP=柳氮磺胺吡啶,ALM=腺瘤样病变或肿物,DALM=异型增生相关病变或肿物,LGD=轻度异型增生,HGD=重度异型增生;EMR=内镜下黏膜切除
2.3结肠隆起型异型增生发生的影响因素以发生结肠隆起型异型增生为结局事件,以患者的病程为时间变量,代入Cox比例风险回归模型,结果显示,炎症性肠病家族史、疾病活动程度和疾病复发情况与结肠隆起型异型增生有回归关系(P<0.05);性别、起病年龄、结肠癌家族史、吸烟、病变范围和接受至少2年以上的5-ASA/SASP维持治疗与结肠隆起型异型增生无回归关系(P>0.05,见表2)。采用Kaplan-Meier法对炎症性肠病家族史、疾病活动程度和疾病复发情况3个影响因素绘制生存曲线,Log-rank检验结果显示,无炎症性肠病家族史者、中度活动者及疾病偶发患者的累计生存率高于有炎症性肠病家族史者、重度活动者及疾病频发/持续活动患者,差异有统计学意义(χ2值分别为4.631、7.382、13.438,P值分别为0.031、0.007、<0.001,见图9~11)。
3讨论
炎症性肠病相关CRC的发生只占全部结直肠癌的1%~2%,但是炎症性肠病患者最为严重的并发症[8],最近的研究表明,有近15%的炎症性肠病患者死于炎症性肠病相关CRC[9]。很多研究表明,随着炎症性肠病病程的延长结直肠癌的发病率逐渐递增,从8~10年的2.0%~2.9%,到15~20年的5.6%~8.0%,再到30年的8.3%~18.0%[8,10-11]。炎症性肠病患者出现的异型增生被认为是炎症性肠病相关CRC发生的最可靠的癌前标志[12]。本研究观察了炎症性肠病相关CRC的癌前病变中的重要部分——结肠隆起型异型增生,发现该病变也有着随病程延长逐渐增高的趋势,而且与炎症性肠病相关CRC有着近似的数值。本研究发现,DALM伴HGD仅3例,占全部病例的比例不足1.0%,与国内一些研究接近,提示国人炎症性肠病相关CRC的发生率较低[13-14]。
表2炎症性肠病患者结肠隆起型异型增生发生影响因素的Cox比例风险回归分析
Table 2Cox proportional hazards regression analysis of the influencing factors for the occurrence of IBD colon uplift type dysplasia

变量βSEWaldχ2值P值OR值95%CI性别1.5140.9472.5560.1104.55(0.71,29.08)起病年龄0.0070.0260.0660.7981.01(0.96, 1.06)炎症性肠病家族史3.4081.5844.6310.03130.20(1.36,673.07)结肠癌家族史-2.6322.1091.5570.2120.07(0.01, 4.49)吸烟1.4470.8372.9860.0844.25(0.82,21.93)病变范围-0.8500.8481.0050.3160.43(0.08, 2.25)疾病活动程度3.3061.2217.3280.00727.29(2.49,298.92)疾病复发情况3.4350.93713.438<0.00131.04(4.95,194.82)接受至少2年以上的5-ASA/SASP维持治疗-0.3961.0140.1530.6960.67(0.09, 4.91)
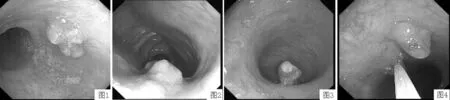
图1直肠不规则隆起病变:DALM图2降结肠隆起病变:ALM
Figure 1Rectum irregular uplift lesions:DALMFigure 2Descending colon uplift lesions:ALM
图3乙状结肠隆起病变:ALM图4乙状结肠多发隆起病变:ALM
Figure 3Sigmoid colon uplift lesions:ALMFigure 4Sigmoid colon multiple uplift lesions:ALM

图5直肠管状腺瘤Ⅲ级,HGD(×4)图6直肠管状腺瘤Ⅲ级,HGD(×20)
Figure 5Rectum tubular adenoma grade Ⅲ,HGD Figure 6Rectum tubular adenoma grade Ⅲ,HGD
图7横结肠锯齿状腺瘤,LGD(×4)图8降结肠绒毛-管状腺瘤,LGD(×4)
Figure 7Transverse colon serrated adenoma,LGDFigure 8Descending colon villous-tubular adenoma,LGD
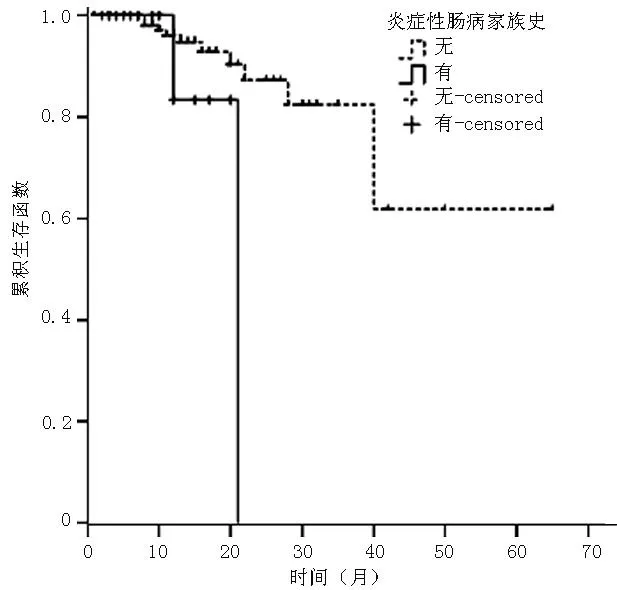
图9有无炎症性肠病家族史患者结肠隆起型异型增生发生生存曲线
Figure 9Survival curves of the occurrence of colon uplift type dysplasia of patients with or without IBD family history
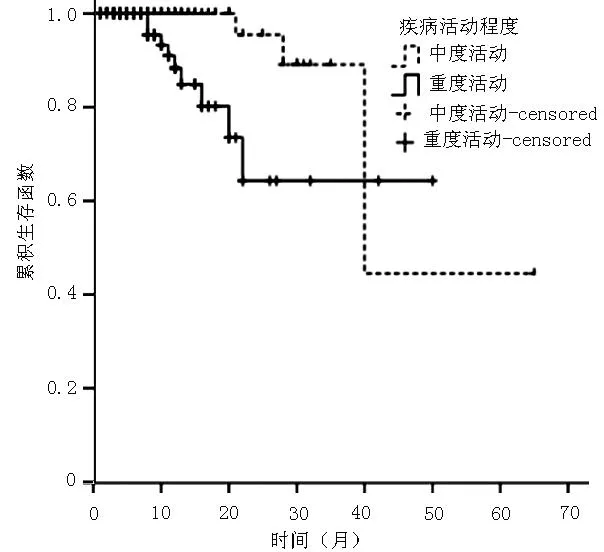
图10不同疾病活动程度患者结肠隆起型异型增生发生生存曲线
Figure 10Survival curves of the occurrence of colon uplift type dysplasia of patients with different disease activity degrees
炎症性肠病相关CRC的高危因素主要包括发病年龄、病程、病变范围、结肠癌家族史、病程迁延和伴发PSC等[15-17]。本研究以病程作为时间变量,通过Cox比例风险回归分析得出,炎症性肠病家族史、疾病活动程度和疾病复发情况3项是炎症性肠病结肠隆起型异型增生发生的高危因素,与既往国内研究结论相似[18],提示炎症性肠病患者遵循着“慢性炎症-异型增生-恶性肿瘤”[3]这一病理改变途径。提示对炎症性肠病的治疗不但要临床缓解,更要以达到黏膜愈合,以减少复发,可以有效地预防炎症性肠病患者异型增生乃至炎症性肠病相关CRC的发生。本研究发现,炎症性肠病家族史也是结肠隆起型异型增生发生的高危因素,提示炎症性肠病结肠隆起型异型增生的发生有一定的家族遗传倾向,对具有炎症性肠病家族史的患者更要注意结肠镜的随访工作。疾病活动程度也是结肠隆起型异型增生的高危因素。
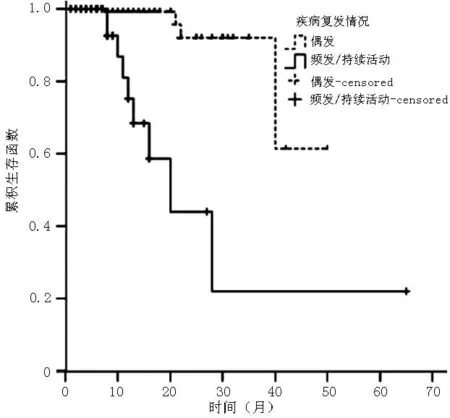
图11不同疾病复发情况患者结肠隆起型异型增生发生生存曲线
Figure 11Survival curves of the occurrence of colon uplift type dysplasia of patients with different conditions of relapse
起病年龄是炎症性肠病相关CRC的另一项高危因素,本研究中并未得出此结果。推测因为从异型增生到炎症性肠病相关CRC还需要一段时间,这样在是否发生结肠隆起型异型增生的两组患者之间的起病年龄差异可能被缩小。虽然没有得出起病年龄是高危因素这一结果,但是从发生结肠隆起型异型增生的平均年龄仅为38.4岁上也可以观察出有这样的趋势。以往研究提示,结肠肿瘤家族史也是炎症性肠病相关CRC的高危因素[18],本研究中具有结肠癌家族史的患者仅有7例,无法达到统计学分析的需要,所以没有得出相关结论。病变范围是炎症性肠病相关CRC的另一个高危因素,本研究并未得出此结果,可能与病例数量少有关系。分析13例结肠隆起型异型增生患者,仍可以看出有10例为E3和L2。
早期研究表明,SASP对炎症性肠病相关CRC有一定的化学预防作用[19]。随后国内外的一些学者通过Meta分析得出,5-ASA对炎症性肠病相关CRC具有化学预防作用[20-22]。本研究未发现接受至少2年以上的5-ASA/SASP维持治疗对炎症性肠病结肠隆起型异型增生的发生具有保护作用。可能的原因是,一方面并非所有的研究对5-ASA的化学预防作用有一致的结论[23],另一方面本研究中接受至少2年以上的5-ASA/SASP维持治疗的患者只有224例,占全部患者的比例不足60.0%,可能与样本量有关。
对于结肠隆起型异型增生的处理,美国胃肠病学会于2010年提出了证据等级为A级的强烈推荐方案[24],即伴有DALM的炎症性肠病患者行全结肠切除;对有ALM而结肠其他部位无扁平型异型增生的炎症性肠病患者可行息肉切除术并继续监测。本研究中的结肠隆起型异型增生的处理正是遵照上述处理意见进行的,ALM患者在EMR后3个月内随访结肠镜并病理学检查均未发现复发。而对于DALM和多发难以判断其他部位异型增生情况的患者选择了全结肠切除。
本研究针对的是炎症性肠病相关CRC的癌前病变的发生,这一阶段是炎症性肠病患者随访中可控可治的良机。了解炎症性肠病患者结肠隆起型异型增生的发生情况和高危因素可以更早地做出恰当的处理,从而预防炎症性肠病相关CRC的发生。本研究不足为:首先,受病例数所限,部分高危因素的探究并不深入;其次,本研究是回顾性分析,数据完整没有失访,但病程中位数为11年,没有观察到更长病程的结局,且有一定的选择偏倚;最后,受到实际临床工作的限制,结肠镜随访没有严格按照每10 cm进行4象限随机活检的标准进行,这直接导致本研究只能局限在探讨结肠隆起型异型增生的发生这一局限的方面。这些不足之处更激发今后对炎症性肠病相关CRC以及其癌前病变的临床研究的兴趣。通过设计前瞻性的研究,利用目前先进的共聚焦显微内镜等技术,组成多中心的研究团队,找到针对国人炎症性肠病相关CRC的高危因素和预防措施。
作者贡献:田雨、李俊霞进行试验设计与实施、资料收集整理、撰写论文、成文并对文章负责;田原、刘冠伊进行试验实施、评估、资料收集;王化虹、刘新光进行质量控制及审校。
本文无利益冲突。
参考文献
[1]Jess T,Horváth-Puhó E,Fallingborg J,et al.Cancer risk in inflammatory bowel disease according to patient phenotype and treatment:a Danish population-based cohort study[J].Am J Gastroenterol,2013,108(12):1869-1876.
[2]Pellisé M.Overcoming challenges in IBD management:management of colonic dysplastic lesions[J].Dig Dis,2013,31(2):244-247.
[3]Matkowskyj KA,Chen ZE,Rao SR,et al.Dysplastic lesions in inflammatory bowel disease molecular pathogenesis to morphology[J].Arch Pathol Lab Med,2013,137(3):338-350.
[4]Vu M,Chang JY,Chen J,et al.Inflammatory bowel disease associated colorectal neoplasia[J].J Gastrointest Dig Syst,2012,23(Suppl 8):2.
[5]Chinese Society of Gastroenterology Committee of Inflammatory bowel disease.Consensus of the diagnosis and treatment for inflammatory bowel disease (2012 Guangzhou)[J].Chin J Intern Med,2012,51(10):818-831.(in Chinese)
中华医学会消化病学分会炎症性肠病学组.炎症性肠病诊断与治疗的共识意见(2012年·广州)[J].中华内科杂志,2012,51(10):818-831.
[6]Odze RD.Adenomas and adenoma-like DALMs in chronic ulcerative colitis:a clinical pathological,and molecular review[J].Am J Gastroenterol,1999,94(7):1746-1750.
[7]Schlemper RJ,Riddell RH,Kato Y,et al.The Vienna classification of gastrointestinal epithelial neoplasia[J].Gut,2000,47(2):251-252.
[8]Mattar MC,Lough D,Pishvaian MJ,et al.Current management of inflammatory bowel disease and colorectal cancer[J].Gastrointest Cancer Res,2011,4(2):53-61.
[9]Herrinton LJ,Liu L,Levin TR,et al.Incidence and mortality of colorectal adenocarcinoma in persons with inflammatory bowel disease from 1998 to 2010[J].Gastroenterology,2012,143(2):382-389.
[10]Rutter MD,Saunders BP,Wikinson KH,et al.Thirty-year analysis of a colonoscopic surveillance program for neoplasis on ulcerative colits[J].Gastroenterology,2006,130(4):1030-1038.
[11]Canavan C,Abrams KR,Mayberry J.Meta-analysis:colorectal and small bowel cancer risk in patients with Crohn′s disease[J].Aliment Pharmacol Ther,2006,23(8):1097-1104.
[12]Farraye FA,Odze RD,Eaden J,et al.AGA technical review on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease[J].Gastroenterology,2010,138(2):746-774.
[13]Li JN,Zheng WY,Qian JM,et al.Clinical characters of ulcerative colitis associated colorectal cancer and carcinogenesis related protein expression[J].Chin J Dig,2010,30(11):808-810.(in Chinese)
李景南,郑威扬,钱家鸣,等.溃疡性结肠炎相关结直肠癌临床特点及癌变相关蛋白的表达[J].中华消化杂志,2010,30(11):808-810.
[14]Gong W,Lv N,Wang B,et al.Risk of ulcerative colitis associated colorectal cancer in China:a multi-center retrospective study[J].Dig Dis Sci,2012,57(2):503-507.
[15]Andersen NN,Jess T.Has the risk of coloroctal cancer in inflammatory bowel disease decreased?[J].World J Gastroenterol,2013,19(43):7561-7568.
[16]Xie JL,Itzkowitz SH.Cancer in inflammatory bowel disease[J].World J Gastroenterol,2008,14(3):378-389.
[17]Ekbom A,Helmick C,Zack M,et a1.Ulcerative colitis and colorectal cancer.A population-based study[J].N Engl J Med,1990,323(18):1228-1233.
[18]Zhao YJ,Yuan YZ.A clinical study on relationship between inflammatory bowel disease and colocrectal cancer[J].Chin J Dig,2008,28(12):827-830.(in Chinese)
赵玉洁,袁耀宗.炎症性肠病与结直肠癌关系的临床初步探讨[J].中华消化杂志,2008,28(12):827-830.
[19]Pinczowski D,Ekbom A,Baron J,et al.Risk factors for colorectal cancer in patients with ulcerative colitis:a case-control study[J].Gastroenterology,1994,107(1):117-120.
[20]Velayos FS,Terdiman JP,Walsh JM.Effect of 5-aminosalicylate use on colorectal cancer and dysplasia risk: a systematic review and metaanalysis of observational studies[J].Am J Gastroenterol,2005,100(6):1345-1353.
[21]van Staa TP,Card T,Logan RF,et al.5-Aminosalicylate use and colorectal cancer risk in inflammatory bowel disease:a large epidemiological study[J].Gut,2005,54(11):1573-1578.
[22]Wang CD,Yu CM.The chemopreventive effect of 5-aminosalicylic acid on inflammatory bowel disease associated colonic cancer and dysplasia:a meta-ayalysis[J].Chin J Gastroenterol Hepatol,2013,22(4):348-353.(in Chinese)
王乘党,喻春梅.5-氨基水杨酸对炎症性肠病相关结肠癌和上皮内瘤变化学预防:Meta分析[J].胃肠病学和肝病学杂志,2013,22(4):348-353.
[23]Nguyen GC,Gulamhusein A,Bernstein CN.5-aminosalicylic acid is not protective against colorectal cancer in inflammatory bowel disease:a meta-analysis of nonreferral populations[J].Am J Gastroenterol,2012,107(9):1298-1304.
[24]Farraye FA,Odze RD,Eaden J,et al.AGA medical position statement on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease[J].Gastroenterology,2010,138(2):738-745.
(本文编辑:陈素芳)
【关键词】肠炎;结肠炎,溃疡性;克罗恩病;增生;影响因素分析
田雨,李俊霞,田原,等.炎症性肠病结肠隆起型异型增生影响因素的回顾性研究[J].中国全科医学,2016,19(6):652-657,665.[www.chinagp.net]
Tian Y,Li JX,Tian Y,et al.Retrospective analysis of relevant influencing factors for the occurrence of uplift type dysplasia in the colons of patients with inflammatory bowel disease[J].Chinese General Practice,2016,19(6):652-657,665.
Retrospective Analysis of Relevant Influencing Factors for the Occurrence of Uplift Type Dysplasia in the Colons of Patients With Inflammatory Bowel DiseaseTIANYu,LIJun-xia,TIANYuan,etal.DepartmentofGastroenterology,PekingUniversityFirstHospital,Beijing100034,China
【Abstract】BackgroundAs the prevalence of inflammatory bowel disease(IBD)in China is increasing,the morbidity of IBD associated colorectal cancer and precancerous lesions are worth noticing.ObjectiveTo investigate relevant influencing factors for the occurrence of IBD colon uplift type dysplasia.MethodsA total of 393 IBD patients who were followed up by endoscope in Peking University First Hospital from January 2007 to January 2014 were enrolled in the study.Clinical data and pathological results of the patients were collected.With uplift type dysplasia as outcome event and disease duration as time variable,the influencing factors for the occurrence of IBD colon uplift type dysplasia were analyzed and screened by Cox proportional hazards regression.ResultsA total of 13 cases had colon uplift type dysplasia among the 393 IBD cases.Among the 13 cases,12 cases were ulcerative colitis and 1 case was Crohn′s disease;10 cases had adenoma-like lesion or mass(ALM) and 3 cases had dysplasia associated lesion or mass(DALM).The result of Cox proportional hazards regression model showed that regression correlation existed between colon uplift type dysplasia and IBD family history,disease activity degree and disease relapse (P<0.05);regression correlation did not exist between colon uplift type dysplasia and gender,onset age,family history of colon cancer,smoking,scope of lesions and receiving maintenance treatment of 5-aminosalicylic acid (5-ASA)/Salazosulfapyridine (SASP)for at least two years (P>0.05).Log-rank test result showed that cumulative survival rate of patients who had no IBD family history and had moderate activity and accidental symptoms was higher than that of patients who had IBD family history,severe activities and frequent symptoms/persistent activity (χ2= 4.631,7.382,13.438;P=0.031,0.007,<0.001).Among 10 cases of ALM,9 cases were given tumor resection by endoscope and 1 case with multiple ALM was given total colectomy.Among 3 cases of DALM,1 case was given total colectomy and 2 cases were not given operative treatment because of serious disease or poor general physical condition.ConclusionThe incidence of IBD colon uplift type dysplasia increases with prolonged disease duration.High risk factors include IBD family history,disease activity degree and disease relapse.
【Key words】Enteritis;Colitis,ulcerative;Crohn disease;Hyperplasia;Root cause analysis
(收稿日期:2015-05-12;修回日期:2015-12-13)
【中图分类号】R 574.621
【文献标识码】A
doi:10.3969/j.issn.1007-9572.2016.06.007
通信作者:李俊霞,100034 北京市,北京大学第一医院消化内科;E-mail:lijxtom@foxmail.com