不同治疗方式对粉碎性柯雷氏骨折两个解剖角的影响
2015-12-20刘晋闽
曾 武,刘晋闽
·作者须知·
不同治疗方式对粉碎性柯雷氏骨折两个解剖角的影响
曾武1,刘晋闽2
目的:观察锁定钢板内固定术、手法复位后外固定架固定或高分子夹板固定维持粉碎性柯雷氏骨折(Colles骨折)掌倾角及尺偏角的情况。方法:搜集64例(72侧)分别行锁定钢板内固定术、手法复位后外固定架或高分子夹板固定的粉碎性Colles骨折患者的相关资料进行,其中锁定钢板组16例(22侧),外固定架固定组18例(18侧),高分子夹板组30例(32侧),定期摄片测其掌倾角、尺偏角,以其差值进行比较分析;根据PRWE评分对腕关节疼痛及功能恢复情况进行评价。结果:锁定钢板组掌倾角差值为1.63±0.81,外固定组掌倾角差值为3.68±0.97,高分子夹板组掌倾角差值为4.78±1.41,统计学检验各组在维持掌倾角上差异有统计学意义。锁定钢板组尺倾角差值为0.56±0.23,外固定组尺倾角差值为2.52±0.85,高分子夹板组尺倾角差值为3.01±0.91,统计学检验各组在维持掌倾角上差异有统计学意义。在功能恢复上,锁定钢板组功能恢复优良率为86.4%,外固定组功能恢复优良率为72.2%,高分子夹板组优良率为75.0%,统计学检验三组之间差异无统计学意义。结论:与手法复位后外固定架或高分子夹板固定相比,锁定钢板内固定在维持复位后两个解剖角方面具有一定的优势,但功能恢复没有明显优势。
Colles骨折;粉碎性;固定;掌倾角;尺偏角
粉碎性Colles骨折需考虑固定可靠性、功能恢复情况、经济条件及肌肉牵拉等多种因素,在取得良好复位后,使用何种固定物固定才能更好地维持其复位效果,相关报道较少。我院从2012年6月—2014年1月,分别采用锁定钢板、外固定架及高分子夹板治疗粉碎性Colles骨折64例(72侧),均获得12~15个月的随访。现报告如下。
1 资料与方法
1.1一般资料本组共64例(72侧),根据患者伤情,详细告知各种治疗方法的优缺点,由患者决定治疗方式,并将符合粉碎性Colles骨折的病例分配入锁定钢板组、外固定架组和高分子夹板组,见表1。3组年龄、性别及分型无统计学意义(P>0.05)
表1 3组患者年龄、性别及分型情况(±s)

表1 3组患者年龄、性别及分型情况(±s)
组别锁定钢板组外固定架组高分子夹板组年龄(±s)C2C3 61.8±6.8 59±8.6 52±7.4 AO分型(n)[1]A3 11 9 16 651 1 545 Gustilo-Anderson分型(n)[2]I 22 80 II 0 10 0
1.2治疗方法锁定钢板组取掌侧Henry入路,复位良好后安装合适T形锁定钢板及螺钉,拔出克氏针,活动腕关节,无明显移位,仔细止血,安装Drainobag引流装置引流,逐层缝合后包扎。外固定架组均在急诊行手术治疗,复位可后安装合适大小外固定架,并探查血管神经有无损伤,有损伤者进行修补,无损伤者逐层缝合后包扎。石膏固定组采用血肿内阻滞麻醉,复位后予高分子夹板于Colles骨折固定于掌屈5°~15°并最大限度尺偏位,并予三角巾取屈肘90°、前臂中立位悬吊于胸前限制患肢活动。2周后改为前臂中立位再固定4周,拆除高分子夹板,定期功能锻炼及摄片。
1.3疗效评定掌倾角测量根据放射科自带的角度测量系统所测得的角度值对相关资料进行搜集。PRWE评分[3]主要依据疼痛和功能两个方面评定,以减少主观因素:疼痛(40分);功能(60分)。
1.4统计学处理应用SPSS 19.0统计软件进行分析,计量资料以均值±标准差(±s)表示,符合正态分布用方差分析,两两比较采用q检验,计数资料采用χ2检验,以P<0.05为显著性差异标准。
2 结果
术后3个月X线片示骨折线基本模糊,结合症状及体征,证实骨折端已骨性愈合,逐渐开始正常活动。术后第1 d测得的掌倾角、尺偏角,减去术后1年至1年半内拆除内固定或复查时测得的差值比较见表2。采用方差分析或χ2检验发现,锁定钢板组掌倾角差值为1.63±0.81,外固定组掌倾角差值为3.68±0.97,高分子夹板组掌倾角差值为4.78± 1.41,统计学检验各组在维持掌倾角上差异有统计学意义。锁定钢板组尺倾角差值为0.56±0.23,外固定组尺倾角差值为2.52±0.85,高分子夹板组尺倾角差值为3.01±0.91,统计学检验各组在维持掌倾角上差异有统计学意义。
表2 3组患者术后第1 d与术后1年至1年半腕关节正侧位差值比较(±s)
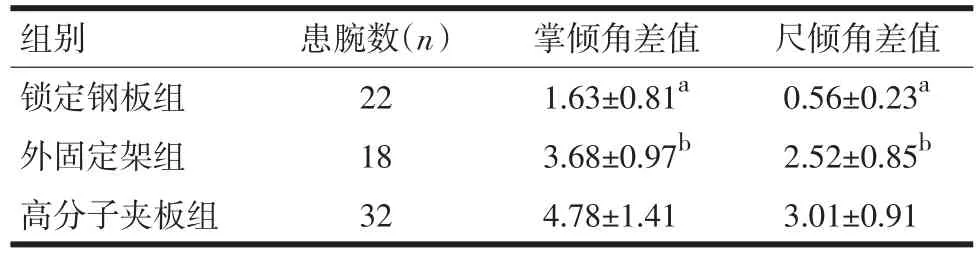
表2 3组患者术后第1 d与术后1年至1年半腕关节正侧位差值比较(±s)
注:与外固定架组比较,aP<0.05;与高分子夹板组比较,bP<0.05
组别锁定钢板组外固定架组高分子夹板组患腕数(n)22 18 32掌倾角差值1.63±0.81a3.68±0.97b4.78±1.41尺倾角差值0.56±0.23a2.52±0.85b3.01±0.91
按照PRWE评分,对术后1年至1年半拆除内固定或复查时功能恢复优良率进行对比。见表3。通过统计学分析后,在功能恢复上,锁定钢板组功能恢复优良率为86.4%,外固定组功能恢复优良率为72.2%,高分子夹板组优良率为75.0%,统计学检验三组之间差异无统计学意义。

表3 3组患者术后第1 d与术后1年至1年半患腕功能恢复情况比较(n,%)
3 讨论
Safdari等[4]通过对76例桡骨远端关节内骨折行掌侧钢板或外固定架固定者比较发现,在功能恢复上两者无统计学意义,但若考虑早日投入工作中,掌侧钢板具有明显的优势。粉碎性Colles骨折不论是那种治疗方法,年龄越大,功能恢复越差。为了获得良好的复位,我们参考了Park等[5]最近发表的一篇临床试验性研究,其通过螺钉可变角度的掌侧钢板及术后功能锻炼,认为尽早功能锻炼有利于促进正常解剖关系的恢复。对各30例的两组不稳定性桡骨远端骨折者分别行锁定钢板和非锁定钢板固定后,Kumar等[6]发现,两组功能评分上并无差异,但在维持正常解剖关系上锁定钢板组明显优于后者。在复位成功后,使用固定物固定也不一定能保证复位不存在丢失可能,而作为桡骨正常结构的生理解剖角,掌倾角、尺倾角在评价骨折复位是否良好中具有重要的参考作用虽相关报道较多,但直接以其术后1年或1年半拆除固定物或复查时影像学资料作为研究者未见报道。值得一提的是,国外有学者[7]认为与影像学评估相比,通过视觉评估桡骨远端骨折并制定治疗计划明显不如结合两者好。我院为了进一步了解这一骨折治疗方式与这两个解剖角是否存在相关性,随机搜集了分别行锁定钢板固定、外固定架固定及高分子夹板固定患者的影像学资料,并利用我院影像科自带的角度测量系统,对具有完整资料的相关病例资料进行搜集并进行统计学分析。3组术后1年至1年半复查或拆除内固定时,术后功能无明显统计学差异。笔者认为,可能掌倾角、尺偏角两个重要解剖角的维持与功能恢复可能不存在明显相关性。而Young等[8]通过研究25例>60岁患者后发现,非手术治疗桡骨远端粉碎性骨折,可获得良好的功能,因此认为功能恢复与影像学畸形并不存在明显相关性。但是Cai等[9]的一项关于老年人桡骨远端骨折回顾性研究利用多重回归分析则发现,桡骨高度及倾斜角与功能具有显著相关性。
与锁定钢板相比,克氏针虽然用于桡骨远端骨折较以往减少,主要因为其容易出现针道感染等并发症,Zong等[10]在最近发表的Meta分析中认为,与克氏针固定相比,锁定钢板在1年随访期间内发生浅表感染的几率要小,只是目前缺少足够的临床资料证实。基于对钢板固定桡骨远端骨折术后平均随访多小于12个月,MacFarlane等[11]通过对187例平均随访达30个月的这类骨折患者进行随访后发现,行钢板内固定能帮助患者更好的恢复正常工作能力。笔者认为,外固定架、克氏针与锁定钢板比较,具有各自的优缺点,值得注意的是,由于粉碎性Colles骨折稳定性较差,即使固定前骨折端活动良好的复位,由于选择固定物不同、肌肉牵拉力、重力及患者自身主被动活动等多种因素共同影响下,骨折断端可能会产生位移,从而导致一定程度上的复位丢失。一方面[12],年龄越大、术后掌倾角恢复越差,其功能恢复越差;另一方面,若术者术中能采用微创技术,减少旋前圆肌的损伤,将更有利于术后功能恢复[13]。Jiang等[14]认为大约2%的桡骨远端骨折患者在30天内会出现并发症,了解这一特点可能对避免并发症的发生会有帮助。有资料[15]显示,术后1年对行外固定架及掌侧钢板固定桡骨远端骨折患者通过Green&O’Brein评分系统比较发现,前者优于后者。本研究中发现,石膏固定组在维持掌倾角及尺倾角方面疗效均逊色于外固定架组及锁定钢板组,但就功能恢复及疼痛方面来说,3种治疗方法并无明显统计学差异。考虑到样本数量较小,难以避免误差。建议在术前制定治疗方案时,既要充分考虑患者自身经济条件及对功能要求情况,又要考虑手术适应症等多种因素,以便选择更为合适的治疗方法。
[1]张英泽.临床骨折分型[M].北京:人民卫生出版社,2013:143-153.
[2]Gustilo RB.Problems in the management of type III(severe)open fractures:a new classification of type III open fractures[J].J Trau⁃ma,1984,24(8):742-746.
[3]MacDermid JC,Turgeon T,Richards RS,et al.Patient rating of wrist pain and disability:a reliable and valid measurement tool[J].J Or⁃thop Trauma,1998,12(8):577-586.
[4]Safdari M,Koohestani MM.Comparing the effect of volar plate fix⁃ators and external fixators on outcome of patients with intra-articu⁃lar distal radius fractures:A clinical trial[J].Electron Physician, 2015,7(2):1085-1091.
[5]Park JW,Kim YH,Park KC,et al.A novel technique for full anatom⁃ic restoration of volar tilt in distal radius fracture[J].Acta Orthop Traumatol Turc,2015,49(2):115-119.
[6]Kumar S,Chopra RK,Sehrawat S,et al.Comparison of treatment of unstable intra articular fractures of distal radius with locking plate versus non-locking plate fixation[J].J Clin Orthop Trauma,2014,5 (2):74-78.
[7]O'Malley MP,Rodner C,Ritting A,et al.Radiographic interpretation of distal radius fractures:visual estimations versus digital measur⁃ing techniques[J].Hand(NY),2014,9(4):488-493.
[8]Young BT,Rayan GM.Outcome following nonoperative treatment of displaced distal radius fractures in low-demand patients older than 60 years[J].J Hand Surg Am,2000,25(1):19-28.
[9]Cai L,Zhu S,Du S.The relationship between radiographic parame⁃ters and clinical outcome of distal radius fractures in elderly pa⁃tients[J].Orthop Traumatol Surg Res,2015,[Epub ahead of print].
[10]Zong SL,Kan SL,Su LX.Meta-analysis for dorsally displaced dis⁃tal radius fracture fixation:volar locking plate versus percutaneousKirschner wires[J].J Orthop Surg Res,2015,10(1):108.
[11]MacFarlane RJ,Miller D,Wilson L,et al.Functional Outcome and Complications at 2.5 Years Following Volar Locking Plate Fixation of Distal Radius Fractures[J].J Hand Microsurg,2015,7(1):18-24.
[12]Cowie J,Anakwe R,McQueen M.Factors associated with one-year outcome after distal radial fracture treatment[J].J Orthop Surg (Hong Kong),2015,23(1):24-28.
[13]Chmielnicki M,Prokop A.New minimally invasive approach for pal⁃mar plating in distal radius fractures[J].Z Orthop Unfall,2015,153 (1):25-28.
[14]Jiang JJ,Phillips CS,Levitz SP,et al.Risk factors for complications following open reduction internal fixation of distal radius fractures [J].J Hand Surg Am,2014,39(12):2365-2372.
[15]Shukla R,Jain RK,Sharma NK,et al.External fixation versus volar locking plate for displaced intra-articular distal radius fractures:a prospective randomized comparative study of the functional out⁃comes[J].J Orthop Traumatol,2014,15(4):265-270.
(收稿:2015-05-28修回:2015-10-28)
(责任编辑韩 慧)
Different Treatment Methods in Maintaining Comminuted Colles Fracture's Effect of Two Anatomical Angles
ZENG Wu,LIU Jin-minThe First Affiliated Hospital of Traditional Chinese Medicine of Zhejiang Province,Hangzhou(310053),China
ObjectiveTo observe the outcome of three methods in treating comminuted Colles fracture by locking plate for internal fixation,closed manual external reduction with external fixator or orthopedic splint in maintaining the fracture's palmar tilt and ulnar inclination.MethodsSixty four cases(72 sides)of outpa⁃tients and emergency or admitted patients by three methods including locking plate for internal fixation,closed manual external reduction with external fixator or orthopedic splint for treatment of comminuted colles fracture were collected,in which containing 16 cases(22 sides)of using locking plate,18 cases(18 sides)of making use of external fixator,and 30 cases(32 sides)of using plaster immobilization.In regular follow-up,using X ray photography,and PRWE(Patient-Rated Wrist Evaluation)score of Wrist joint to evaluate the conditions of pa⁃tients’pain and functional recovery.ResultsThe Palmar tilt’s difference of the group of locking plate for in⁃ternal fixation was 1.63±0.81,and the palmar tilt’s difference of the group of closed manual external reduction with external fixator was 3.68±0.97.The palmar tilt’s difference of the group of orthopedic splint was 4.78±1.41; statistical tests showed difference between groups in maintaining palmar tilt were significant.The ulnar inclina⁃tion’s difference of the group of locking plate for internal fixation was 0.56±0.23,and the ulnar inclination’s dif⁃ference of the group of closed manual external reduction with external fixator was 2.52±0.85,and the ulnar incli⁃nation’s difference of the group of orthopedic splint was 3.01±0.91,statistical tests showed differences between groups in maintaining ulnar inclination were significant.In terms of functional resoration,the excellent and good rate difference between the group of locking plate for internal fixation was 86.4%,and that between the group of closed manual external reduction with external fixator was 72.2%,the group of orthopedic splint was 75.0%,statistical tests showed the difference be⁃tweengroupswerenotsignificant.Conclusion Compared with closed manual external reduction withexternal fixator or orthopedic splint,locking plate internal fixation in the aspect of maintaining the two angles of anatomical reduction shows some advantages of clinical reference value,but no obvious advantage in terms of re⁃covery of function.
Colles’fracture;comminuted;fixation;palmar tilt;ulnar inclination
R683.41
A
1007-6948(2015)06-0574-04
10.3969/j.issn.1007-6948.2015.06.008
1.浙江中医药大学第一临床医学院(杭州310053)
2.浙江中医药大学附属第一医院骨伤科病区(杭州 310006)
曾武,E-mail:1023705176@qq.com
