舒芬太尼复合异丙酚在急性心肌梗死镇痛中的应用研究
2015-06-28谈媛媛
谈媛媛
舒芬太尼复合异丙酚在急性心肌梗死镇痛中的应用研究
谈媛媛
目的探讨舒芬太尼复合异丙酚麻醉在急性心肌梗死镇痛中的应用效果。方法按随机数字表法将118例急性心肌梗死镇痛患者分为舒芬太尼组与瑞芬太尼组,每组59例。舒芬太尼、瑞芬太尼初始靶效应室浓度分别为0.25、2ng/ml,均复合初始血浆靶浓度为2μg/ml的异丙酚,每2min增加0.5μg/ml,直至患者意识消失。比较两组患者在麻醉诱导前(T0)、插管前(T1)、插管后即刻(T2)、插管后2min(T3)、术毕(T4)和拔管(T5)时的血流动力学变化以及两组麻醉情况、苏醒时间、术后镇痛效果、并发症发生情况。结果两组收缩压(SBP)和舒张压(DBP)于T0–T2时逐渐下降,T2–T5时逐渐上升,心率(HR)于T0–T1时逐渐下降,T1–T5时逐渐上升,但瑞芬太尼组波动较舒芬太尼组更为明显。两组SBP和DBP于T1–T5时有显著性差异,HR于T1、T2和T5时有显著性差异(P<0.05)。两组麻醉时间、意识消失时间、意识消失时异丙酚剂量和异丙酚总剂量无显著性差异(P>0.05);舒芬太尼组自主呼吸恢复时间、呼之睁眼时间、拔管时间和定向力恢复时间均明显长于瑞芬太尼组(P<0.05),VAS评分显著高于瑞芬太尼组,镇痛药使用率及并发症发生率明显低于瑞芬太尼组(P<0.05)。OAA/S评分两组间比较差异无统计学意义(P>0.05)。结论与瑞芬太尼相比,舒芬太尼复合异丙酚麻醉用于急性心肌梗死镇痛患者,血流动力学更加平稳,术后苏醒质量更优,并发症更少,值得临床推广应用。
心肌梗死;舒芬太尼;瑞芬太尼;异丙酚;麻醉
近年来,随着心脏大血管技术的提高及老龄化人口的增加,心脏大血管手术患者数量日益增多,由于患者多存在多种心脑血管疾病,耐受性低,对手术麻醉提出了更高的要求。王竹梅等[1]报道瑞芬太尼复合异丙酚靶控输注用于急性心肌梗死患者镇痛,麻醉诱导平稳,术后恢复快且安全性高。本研究以瑞芬太尼为对照,探讨等效剂量的舒芬太尼复合异丙酚麻醉对急性心肌梗死镇痛患者血流动力学及苏醒质量的影响,以期为临床应用提供参考。
1 资料与方法
1.1 一般资料 选取2012年1月-2014年6月安徽医科大学第一附属医院收治的择期行急性心肌梗死手术的患者118例,男65例,女53例,年龄70.5±3.2(65~85)岁,体重61.2±4.6(45~75)kg。其中心肌梗死64例,冠心病24例,缺血缺氧型心脏病30例。按随机数字表法分为舒芬太尼组(n=59)与瑞芬太尼组(n=59),两组患者性别、年龄、体重、疾病类型等一般资料比较差异无统计学意义(P>0.05),具有可比性。
1.2 纳入及排除标准 纳入标准:年龄65岁以上,ASA分级Ⅰ-Ⅲ级,无阿片类的药物、异丙酚过敏史,术前未服用影响血糖、血压及代谢药物。排除严重心肺肝肾功能不全及血液系统疾病患者。本研究经医院伦理委员会批准,患者均签署知情同意书。
1.3 方法 手术前30min肌注阿托品0.5mg,苯巴比妥钠0.1g,开放静脉通路,采用DatexOhmeda监护仪常规监测血压(BP)、心率(HR)、血氧饱和度(SpO2)。静脉注射咪唑安定0.05mg/kg,维库溴铵0.1mg/kg,舒芬太尼0.3~0.5μg/kg或瑞芬太尼3~5μg/kg,异丙酚2~2.5mg/kg麻醉诱导。吸氧3~5min后行气管插管,接麻醉机行机械通气,呼吸频率12次/min,吸呼比1:2,潮气量8~10ml/kg,气腹前呼吸末CO2分压30~35mmHg (1mmHg=0.133kPa)。诱导时舒芬太尼、瑞芬太尼初始靶效应室浓度分别为0.25、2ng/ml,异丙酚初始血浆靶浓度为2μg/ml,每2min增加0.5μg/ml,直至患者意识消失。两组术中根据BP、HR调整舒芬太尼、瑞芬太尼血浆靶浓度,维持脑电双频指数(BIS)50~60。若收缩压(SBP)<90mmHg或低于基础血压20%,则静注麻黄碱5~10mg;若HR<60次/min,则静注阿托品0.3~0.5mg。所有患者均不采用任何麻醉性药物的拮抗药促醒。两组局麻处理均由同一麻醉医师完成,且未被告知患者分组情况。
1.4 效果评价 ①血流动力学变化:监测两组患者麻醉诱导前(T0)、插管前(T1)、插管后即刻(T2)、插管后2min(T3)、术毕(T4)和拔管(T5)时的HR、平均动脉压(MAP)和SpO2;②麻醉情况:记录两组麻醉时间、意识消失时间、意识消失时异丙酚剂量及异丙酚总剂量;③苏醒时间:记录两组自主呼吸恢复时间、呼之睁眼时间、拔管时间、定向力恢复时间;④镇痛效果及并发症:记录两组术后30min疼痛视觉模拟评分(VAS)、警觉/镇静评分(OAA/S)、镇痛药使用率以及围术期恶心、呕吐、躁动等并发症发生情况。
1.5 统计学处理 采用SPSS 13.0软件进行统计分析,计量资料以表示,组间比较采用F检验或χ2检验,P<0.05为差异有统计学意义。
表1 两组麻醉期间血流动力学情况比较(±s,n=59)Tab.1 Comparison of hemodynamic indexes during anesthesia between two groups (±s,n=59)
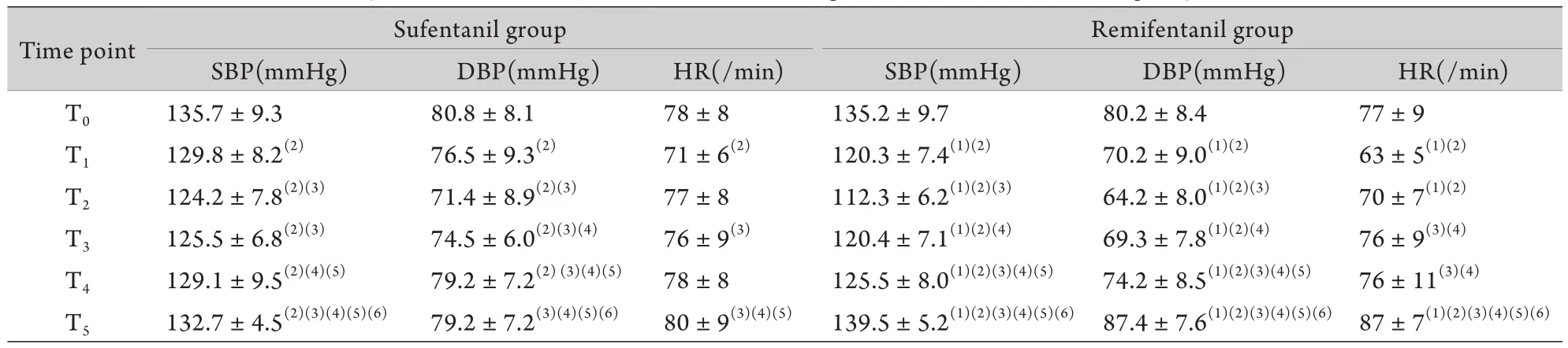
表1 两组麻醉期间血流动力学情况比较(±s,n=59)Tab.1 Comparison of hemodynamic indexes during anesthesia between two groups (±s,n=59)
T0. Pre-anesthesia induction; T1. Pre-intubation; T2. Immediately after intubation; T3. 2min after intubation; T4. End of operation; T5. Extubation; (1)P<0.05 compared with sufentanil group; (2)P<0.05 compared with T0; (3)P<0.05 compared with T1; (4)P<0.05 compared with T2; (5)P<0.05 compared with T3; (6)P<0.05 compared with T4
Remifentanil group SBP(mmHg) DBP(mmHg) HR(/min) SBP(mmHg) DBP(mmHg) HR(/min) T0 135.7±9.3 80.8±8.1 78±8 135.2±9.7 80.2±8.4 77±9 T1 129.8±8.2(2) 76.5±9.3(2) 71±6(2) 120.3±7.4(1)(2) 70.2±9.0(1)(2) 63±5(1)(2)T2 124.2±7.8(2)(3) 71.4±8.9(2)(3) 77±8 112.3±6.2(1)(2)(3) 64.2±8.0(1)(2)(3) 70±7(1)(2)T3 125.5±6.8(2)(3) 74.5±6.0(2)(3)(4) 76±9(3) 120.4±7.1(1)(2)(4) 69.3±7.8(1)(2)(4) 76±9(3)(4)T4 129.1±9.5(2)(4)(5) 79.2±7.2(2) (3)(4)(5) 78±8 125.5±8.0(1)(2)(3)(4)(5) 74.2±8.5(1)(2)(3)(4)(5) 76±11(3)(4)T5 132.7±4.5(2)(3)(4)(5)(6) 79.2±7.2(3)(4)(5)(6) 80±9(3)(4)(5) 139.5±5.2(1)(2)(3)(4)(5)(6) 87.4±7.6(1)(2)(3)(4)(5)(6) 87±7(1)(2)(3)(4)(5)(6)Time point Sufentanil group
2 结 果
2.1 两组血流动力学变化 两组SBP和舒张压(DBP)于T0–T2时逐渐下降,T2–T5时逐渐上升,HR 于T0–T1时逐渐下降,T1–T5时逐渐上升,但瑞芬太尼组波动较舒芬太尼组更为明显,T1–T5时SBP和DBP组间比较有显著性差异,T1、T2和T5时HR组间比较有显著性差异(P<0.05,表1)。
2.2 两组麻醉情况比较 与瑞芬太尼组比较,舒芬太尼组麻醉时间、意识消失时间、意识消失时异丙酚剂量和异丙酚总剂量之间的差异均无统计学意义(P>0.05,表2)。
2.3 两组苏醒时间比较 舒芬太尼组自主呼吸恢复时间、呼之睁眼时间、拔管时间和定向力恢复时间均明显长于瑞芬太尼组,差异有统计学意义(P<0.05,表3)。
2.4 两组术后镇痛镇静效果及并发症比较 舒芬太尼组VAS评分显著高于瑞芬太尼组(P<0.05),镇痛使用率及并发症发生率明显低于瑞芬太尼组(P<0.05),OAA/S评分两组间比较差异无显著性意义(P>0.05,表4)。
表2 两组麻醉情况比较(±s,n=59)Tab.2 Comparison of anesthesia condition between two groups (±s,n=59)

表2 两组麻醉情况比较(±s,n=59)Tab.2 Comparison of anesthesia condition between two groups (±s,n=59)
Group Anesthesia time (min) Unconsciousness time (min) The dose of propofol when consciousness disappears (mg) Total dose of propofol (mg) Sufentanil group 92.3±15.6 3.8±1.0 70.7±14.5 591.7±204.2 Remifentanil group 91.8±17.6 3.6±0.7 69.2±13.4 587.5±195.3
表3 两组苏醒时间比较(±s,n=59)Tab.3 Comparison of awakening time between two groups (±s,n=59)

表3 两组苏醒时间比较(±s,n=59)Tab.3 Comparison of awakening time between two groups (±s,n=59)
(1)P<0.05 compared with sufentanil group
Group Time of spontaneous breathing recovery (min) Time to eye-opening (min) Extubation time (min) Time of directional force recovery (min) Sufentanil group 6.1±1.3 9.1±1.1 15.7±1.5 17.3±1.3 Remifentanil group 4.6±1.5(1) 7.2±1.2(1) 12.2±1.4(1) 13.1±1.6(1)
表4 两组术后镇痛效果及并发症比较(±s,n=59)Tab.4 Comparison of postoperative analgesia effect and complications between two groups (±s,n=59)

表4 两组术后镇痛效果及并发症比较(±s,n=59)Tab.4 Comparison of postoperative analgesia effect and complications between two groups (±s,n=59)
(1)P<0.05 compared with sufentanil group
Group VAS score OAA/S score Analgesic utilization (%) Complication rate (%) Sufentanil group 16.1±7.3 4.9±0.3 6.7(2/30) 10.0(3/30) Remifentanil group 10.6±9.3(1) 4.8±0.2 26.7(8/30)(1) 33.3(10/30)(1)
3 讨 论
急性心肌梗死镇痛需要行CO2气腹并持续保持一定压力,加之头低足高位,对呼吸及循环系统均有一定不良影响,故要求麻醉必须快速起效,术后迅速苏醒,以避免气腹性生理损害,减少术后疼痛及其引起的血流动力学变化和并发症[2]。同时,由于患者多合并有多种慢性疾病,各种生理功能衰退,麻醉和手术耐受性较差,易发生严重呼吸和循环改变,导致心血管意外,故麻醉不仅要达到足够深度,保证镇痛和肌松充分,有效抑制伤害性应激反应,而且必须对生理功能干扰小,保持心血管系统的稳定[3-4]。
靶控静脉输注是一种新的静脉输注方式,通过调节目标药物浓度控制麻醉深度,相比传统的恒速静脉输注,能更有效地抑制插管和手术引起的应激反应[5-6]。姚东旭等[7]研究证实,瑞芬太尼靶控浓度2ng/ml时麻醉效果满意,可维持血流动力学稳定,气管插管与切皮反应较轻。另有研究表明,等效剂量瑞芬太尼的效应室浓度为舒芬太尼的8倍[8]。故本研究采用靶控输注方式给药探讨2ng/ml的瑞芬太尼与浓度为0.25ng/ml的舒芬太尼在急性心肌梗死镇痛患者中的应用效果。
本研究结果显示,两组麻醉时间、意识消失时间、意识消失时异丙酚剂量和异丙酚总剂量均无明显差别,显示出良好的麻醉效果,但瑞芬太尼组SBP、DBP和HR波动更为明显(P<0.05),表明瑞芬太尼较舒芬太尼更易引起血流动力学剧烈波动。周仁龙等[9]的研究也得出了相同的结论。本研究对麻醉恢复的观察显示,舒芬太尼组自主呼吸恢复时间、呼之睁眼时间、拔管时间和定向力恢复时间均明显长于瑞芬太尼组(P<0.05),VAS评分显著高于瑞芬太尼组(P<0.05),镇痛药使用率及并发症发生率明显低于瑞芬太尼组(P<0.05)。分析原因为瑞芬太尼半衰期短,仅为4~6min,起效迅速,时量相关半衰期不受输注时间长短影响[10],故苏醒较快,术后镇痛作用消失迅速;而舒芬太尼半衰期长,时量相关半衰期随着输注时间的增加而延长,故作用时间更持久,镇痛作用更强,利于抑制机体应激反应。
综上所述,与瑞芬太尼相比,舒芬太尼复合异丙酚麻醉用于急性心肌梗死镇痛患者,血流动力学更加平稳,术后苏醒质量更优,并发症更少,值得临床推广应用。但值得注意的是,舒芬太尼长时间、大剂量输注给药容易蓄积而发生呼吸抑制。因此,在手术结束前应适度降低靶浓度值,以预防呼吸抑制引起CO2蓄积[11]。但同时也要注意满足术后镇痛需要。故本研究在手术结束前30min将舒芬太尼靶浓度设定为0.2ng/ml,取得较好效果,无一例发生呼吸抑制,术后VAS评分高,镇痛药使用率低。
[1]Wang ZM, Yang ZJ, An YW,et al. Effect of target controlled infusion of remifentanil and propofol in elderly patients with laparoscopic cholecystectomy[J]. Chin J Anesthesiol, 2005, 25(9):710-712. [王竹梅, 杨志军, 安裕文, 等. 腹腔镜胆囊切除术老年病人瑞芬太尼复合异丙酚靶控输注静脉麻醉的效果[J]. 中华麻醉学杂志, 2005, 25(9):710-712.]
[2]Ma DX, Liu HL, Yao HY,et al. Effects of intracoronary tirofiban injection on myocardial perfusion and near-future cardiac function in STEM I patients in emergency percataneous coronary artery intervention[J]. Chin Gen Med, 2010, 13(2B):476-478. [马东星, 刘惠亮, 姚宏英, 等. 急诊经皮冠状动脉介入治疗术中冠状动脉内注射盐酸替罗非班对急性ST段抬高型心肌梗死患者心肌灌注及心功能的影响[J]. 中国全科医学, 2010, 13(2B):476-478.]
[3]Wang Z, Tang Q, Tang QZ,et al. TIMI flow influence of intracoronary T irofiban injection in patients with STEMI before primary PCI[J]. Chin J Interv Cardiol, 2009, 17(1):17-19. [王智, 唐强, 唐群中, 等. 急诊经皮冠状动脉介入治疗前冠状动脉内注射盐酸替罗非班对急性ST段抬高型心肌梗死患者术中TIMI血流的影响[J]. 中国介入心脏病学杂志, 2009, 17(1):17-19.]
[4]Gan LX, Liang N. Research on the effects of CO2pneumoperitoneum on respiratory function in patients with progress [J]. J Guangxi Med, 2010, 32(7):860-861. [甘丽霞, 梁宁. CO2气腹对患者呼吸循环功能影响的研究进展[J]. 广西医学, 2010, 32(7):860-861].
[5]Zhou X, Wang QL, Ji M,et al. Joint rayleigh fentanyl propofol target controlled infusion with constant speed infusion mode in craniocerebral surgery effect comparison[J]. J Pract Med, 2009, 25(8):1254-1255. [周翔, 王庆利, 季蒙, 等. 异丙酚联合瑞芬太尼靶控输注与恒速输注模式在颅脑外科手术中效果比较[J]. 实用医学杂志, 2009, 25(8):1254-1255.]
[6]Lv BS, Wang ZQ, Wang W,et al. A clinical evaluation of the effect of sevoflurane or propofol in combination with remifentanil in myasthenia gravis patients undergoing thymectomy[J]. Med J Chin PLA, 2013, 38(7):586-590. [吕宝胜, 王卓强, 王卫, 等.七氟烷或丙泊酚复合瑞芬太尼麻醉在重症肌无力患者胸腺切除术中的应用[J]. 解放军医学杂志, 2013, 38(7):586-590.]
[7]Yao DX, Wei LM, Li M. Target controlled infusion of remifentanil and propofol in aged patients undergoing gynecologic laparoscopic surgery[J]. Chin J Minim Invasive Surg, 2009, 9(2):116-118. [姚东旭, 魏立民, 李民. 瑞芬太尼和丙泊酚靶控输注用于老年患者妇科腹腔镜手术麻醉的研究[J]. 中国微创外科杂志, 2009, 9(2):116-118.]
[8]Lehmann KA, Gerhard A, Horriehs-Haermayer G,et al. Postoperative patient controlled analgesia with sufentanih analgesic eflleaey and minimum efective concentrations[J]. Acta Anaesthesiol Seand, 1991, 35(3):221-226.
[9]Zhou RL, Wang SJ, Hang YN. Application of plasma target controlled infusion of remifentanil in elderly patients during induction of general anesthesia[J]. J Clin Anesthesiol, 2008, 24(2):100-102. [周仁龙, 王珊娟, 杭燕南. 雷米芬太尼靶控输注在患者全麻诱导中的应用[J]. 临床麻醉学杂志, 2008, 24(2):100-102.]
[10]Zhang Y, Li YB, Hu JY. Comparison of the anesthesia effect of remifentanil and fentanil in thoracic surgery[J]. J Chin Basic Med, 2010, 17(17):2367-2368. [张燕, 李羽斌, 胡佳燕. 瑞芬太尼与芬太尼在胸腔镜手术中的麻醉效果比较[J]. 中国基层医药, 2010, 17(17):2367-2368.]
[11]Goulson DT. Anesthesia for outpatient gynecologic surgery[J]. Curt Opin Anaesthesiol, 2007, 20(3):195-200.
The use of sufentanil combined with propofol for analgesia in patients with acute myocardial infarction
TAN Yuan-yuan
Department of Emergency, First Hospital Affiliated to Anhui Medical University, Hefei 230022, China
ObjectiveTo explore the efficacy of sufentanil and propofol for analgesia in patients with acute myocardial infarction (AMI).MethodsAccording to the random number table, 118 AMI patients were divided into sufentanil group and remifentanil group, with 59 in each group. The initial target effect concentrations of sufentanil and remifentanil were 0.25ng/ml and 2ng/ml respectively, and both of them were combined with propofol, initial target plasma concentration of which was 2μg/ml, with an increase of 0.5μg/ml every 2min till the loss of consciousness. Hemodynamic changes at pre-anesthesia induction (T0), preintubation (T1), immediately after intubation (T2), 2min after intubation (T3), end of operation (T4), and extubation (T5), and anesthetic condition, awakening time, postoperative analgesic effect, and complications were compared between two groups.Results
Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were lowered at T0-T2in both groups, and they gradually rose at T2-T5. HR was lowered at T0-T1, and it rose gradually at T1-T5, but SBP and DBP fluctuation was more obvious in remifentanil group than in sufentanil group, with a significant difference at T1-T5, and a significant difference in HR at T1, T2and T5(P<0.05) between two groups. There was no significant difference between two groups in anesthesia time, awakening time, propofol dose, and total dose of propofol during loss of consciousness (P>0.05). The time for recovery of spontaneous breathing, time for eyeopening, upon calling, time of extubation and orientation recovery time were significantly longer in the sufentanil group than those in the remifentanil group (P<0.05). VAS score was significantly higher in sufentanil group than in remifentanil group (P<0.05), but analgesic use rate of the latter and incidence of complications were significantly lower in sufentanil group than in remifentanil group (P<0.05). No significant difference in OAA/S score was found between two groups (P>0.05).ConclusionAs compared with remifentanil, sufentanil combined with propofol is used for analgesia in AMI patients resulting in more stable hemodynamics, better postoperative awakening quality, and fewer complications, thus it is worthy of wider clinical use.
myocardial infarction; sufentanil; remifentanil; propofol; anesthesia
R542.22
A
0577-7402(2015)07-0587-04
10.11855/j.issn.0577-7402.2015.07.15
2015-03-20;
2015-06-05)
(责任编辑:熊晓然)
谈媛媛,医学硕士,主治医师。主要从事急诊医学方面的研究
230022 合肥 安徽医科大学第一附属医院急诊科(谈媛媛)