IdenticalAtrio-Hisintervaland A-AintervalsduringlongRP tachycardia What is the mechanism?
2015-05-24童鸿
●心电学英语
IdenticalAtrio-Hisintervaland A-AintervalsduringlongRP tachycardia What is the mechanism?
Case Presentation
A 46-year-old woman with frequent palpitations underwent electrophysiological study.The findings of transthoracic echocardiography were normal,and a 12-lead ECG showed no ventricular pre-excitation. Four catheters were placed in standard locations:high right atrium,His bundle,coronary sinus(CS),and right ventricular apex.All the recorded baseline intervals were within normal limits.Retrograde ventriculoatrial (VA)conduction showed decremental and dual pathways during ventricular pacing and single extrastimulus testing.Antegrade atrioventricular(AV)nodal conduction showed decremental and triple pathways during atrial single extrastimulus testing.Narrow-complex supraventricular tachycardia(SVT)was reliably induced with a V-A-V sequence by a single ventricular extrastimulus (Figure 1).Ventricular premature depolarization(VPD) during tachycardia,when the His bundle was refractory, did not reset the atrial cycle.Retrograde Wenckebach periodicity occurred during right ventricular overdrive pacing at a cycle length(CL)of 500 ms.The tachycardia was terminated with atrio-His(A-H)and VA block during atrial and ventricular entrainment pacing.Figure 2 shows progressive prolongation and abrupt shortening of the A-A interval with block during SVT.In addition, the A-H interval was identical to the A-A interval during SVT.On the basis of these findings,what is the mechanism of the tachycardia?
Commentary
The differential diagnoses of long RP interval tachycardia,with the earliest atrial activation near the ostium of the CS,are atypical AV nodal reentrant tachycardia(AVNRT),orthodromic reciprocating tachycardia with a slowly conducting and decremental accessory pathway and posteroseptal atrial tachycardia(AT).Because of the presence of the His-refractory VPD without the reset phenomenon as well as sustained SVT during A-H block,the possibility of orthodromic reciprocating tachycardia was excluded.Moreover,automatic AT with initiating AV nodal echo was not completely excluded by the V-A-V sequence1on tachycardia initiation. However,AT was less likely because of the termination of tachycardia with A-H/V-A block during atrial/ventricular entrainment pacing and the direct correlation between the A-A interval and the A-H interval during SVT.Therefore,on the basis of these findings,atypical AVNRT was the most likely diagnosis.
In Figure 2,the first 3 A-A intervals were 450 ms, whereas the A-H intervals were gradually prolonged.
This observation could be explained by the presence of a lower common pathway(LCP,which is defined as the conduction pathway between the tachycardia circuit and the His bundle)with decremental conduction. The presence of an LCP was proven by the fact that the retrograde Wenckebach CL(500 ms)during ventricular pacing was longer than the tachycardia CL(450 ms). Subsequently,the next A-A intervals were progressivelyprolonged to 455-480 ms and further to 540 ms and abruptly shortened to 440 ms with an A-H block.Interestingly,the fifth and sixth A-H intervals were identical to the A-A interval.There are several potential mechanisms that can explain these findings.First,a simple hypothesis was that the A-H intervals became progressively longer because of the decremental conduction of an LCP,which was much stronger than that of the antegrade AV nodal pathway,thereby causing a block of the LCP that was reflected as an A-H block.However,this hypothesis does not explain the abrupt shortening of the A-A intervals with an A-H block.The second hypothesis was that the fifth and sixth As switched to a slow pathway,with a slow LCP resulting in the retrograde A preceding the His bundle.Subsequently,the seventh and eighth As are the result of a double fire from the upper turn around point above the LCP and a lower turn around point(LTP)below the LCP.However,during the first 4 A-A intervals,the conduction of the LCP was progressively prolonged,whereas the conduction of the antegrade AV nodal pathway was only 5 ms.Therefore, in the subsequent As,the hypothesis of an LCP block was more likely.Finally,the most likely mechanism may be the dual ventricular response with an LCP block,that is,the antegrade impulse of the tachycardia circuit traveled down a fast pathway,which was followed by a turn to a retrograde slow pathway via the LTP1 with LCP block before the His bundle(Figure 3).Although,at the same time,the antegrade impulse showed a double ventricular response(Figure 3,asterisk),an antegrade slow pathway was conducted to LTP2 but did not turn to a retrograde slow pathway because of the effective refractory period.The next beat also showed a double ventricular response.First,the antegrade fast pathway was conducted to LTP1 and turned to the retrograde slow pathway,while at the same time,an antegrade slow pathway was conducted to LTP2 with decremental conduction and turned to the retrograde slow pathway, which was characterized by recovered excitability and resumed conduction because of the greater prolongationof the A-A interval.However,the impulse from the retrograde slow pathway,which was turned from the antegrade fast pathway,did not travel down the both antegrade fast and slow pathways because of the effective refractory period.As a result of these conduction pathways,the A-A interval was shortened to 440 ms with an A-H block.

Figure 1Intracardiac electrogram showing that narrow-complex supraventricular tachycardia was induced with a V-A-V sequence by a single ventricular extrastimulus(600/370 ms).CS indicates coronary sinus;HBE,His bundle electrogram;HRA,high right atrium;and RVA,right ventricular apex.
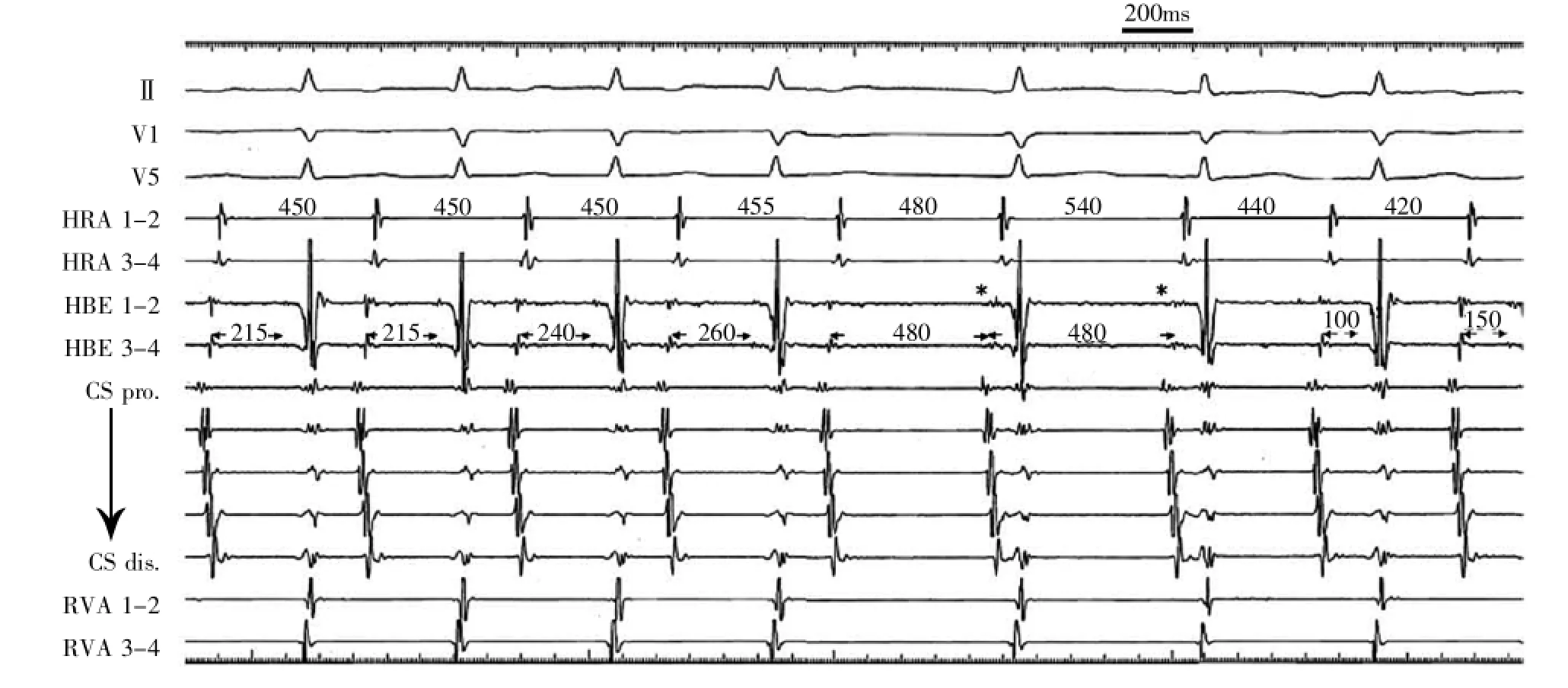
Figure 2Intracardiac electrogram showing progressive prolongation and abrupt shortening of the A-A interval during supraventricular tachycardia.*The atrial and His bundle potentials were fused.

Figure 3Ladder diagram demonstrating the mechanism of supraventricular tachycardia with alternate cycles.*The impulse antegrade of the tachycardia circuit showed dual ventricular response;the fast pathway(solid arrow)turned to the retrograde slow pathway via lower turnaround point(LTP, termed LTP1)with lower common pathway(LCP)block,while at the same time,the antegrade slow pathway(dashed arrow)was conducted to LTP2 and turned to the retrograde slow pathway.AVN indicates atrioventricular node;and LCP,lower common pathway.
Long RP tachycardia with variable A-H intervals is usually diagnosed as AT.However,atypical AVNRT with variable A-H intervals has been reported previously.These reports demonstrated that the A-H intervals during atypical AVNRT were progressively prolonged compared with the prolongation of A-A intervals. This observation was evidenced by the presence of an LCP,as an out-of-tachycardia circuit.In addition,adual ventricular response can be sustained,producing a 1:2 tachycardia,which is otherwise known as a nonreentrant SVT.Nonreentrant SVT typically showed that a single atrial impulse conducts both dual AV nodal pathways,and this is followed by excitation of both the His bundle and the ventricles.The main point of interest of the present case is that the A-A interval were identical to the A-H interval during AVNRT.These observations could be explained by a dual ventricular response with an LCP block.To our knowledge,this is the first case in which atypical AVNRT was sustained via a dual ventricular response.Radiofrequency catheter ablation was applied at the earliest retrograde slow pathway lesion at the posteroseptum,with successful elimination and the absence of inducible tachycardia.
词汇
retrograde adj.&adv.&v.向后的,倒转的,逆向的;向后地;衰退,重述,使倒退
decremental adj.减少的
antegrade adj.顺行的,前进的
abrupt adj.突然的,粗鲁的,陡峭的,唐突的
orthodromic adj.顺行的,顺向传导的
reciprocate v.回报,回报,互换,互给,往复运动
switch n.&v.开关,鞭子,长假发,一击;交换,鞭打,甩动,摆动,挥动,转辙
注释
1.V-A-V sequence也有以V-A-V response表达的,指V-A-V顺序或反应,是心内电生理检查中心室拖带起搏时出现的一种心室-心房-心室序贯波形,提示房室之间至少存在两条传导径路,一条保证心室-心房逆传,而另一条保证心房-心室顺传。通常可以据此来排除自律性增高引起的房性心动过速。有学者认为,当房性心动过速合并存在房室结以外多条房室径路,且其中至少有一条能顺传时,也可出现V-A-V反应,即逆传径路产生V-A而顺传径路产生A-V波,只不过都是旁观者而已。
参考译文
第64课长R-P间期心动过速时心房-希氏束间期与心房-心房间期一致——机制如何?
病例资料
患者女性,46岁。因经常发作心悸而行电生理检查。经胸心脏超声检查结果正常,12导联心电图无心室预激。常规放置4根导管:高位右心房,希氏束,冠状窦(CS)和右心室心尖。所有记录的基础间期在正常范围。在心室起搏和单个期外刺激测试中,逆向室房(VA)传导显示递减性和双径路。在心房单个期外刺激测试中,顺向房室(AV)结传导显示递减性及三径路。单一心室期外刺激伴随V-A-V顺序即能诱发出窄综合波室上性心动过速(SVT)(图1)。希氏束处于不应期时,心动过速期间的室性期前除极(VPD)不能重整心房周期。于周长(CL)500ms的右心室超速起搏时发生逆传文氏周期。在心房和心室拖带起搏时心动过速中止伴随心房-希氏束(A-H)和VA阻滞。图2显示SVT期间A-A间期进行性延长及突发缩短伴随阻滞。另外,SVT期间A-H间期与A-A间期一致。基于这些结果,心动过速的机制是什么?
讨论
伴CS口附近最早心房激动的长R-P间期心动过速的鉴别诊断有不典型AV结折返性心动过速(AVNRT),伴随缓慢且递减传导旁道的顺传型折返性心动过速和后间隔房性心动过速(AT)。鉴于希氏束-不应期时VPD不伴重整现象以及A-H阻滞时SVT持续,可排除顺传型折返性心动过速。此外,心动过速开始时的V-A-V顺序不能完全排除发作开始于AV结回波的自主AT。然而,由于心房/心室拖带起搏时心动过速的中止伴随着A-H/V-A的阻滞,而且SVT时A-A间期与A-H间期直接相关,AT可能性小。因此,基于这些结果,不典型AVNRT是最可能的诊断。
图2中,最初3个A-A间期450ms,而A-H间期逐渐延长。这可由存在一递减传导的下部共同径路(LCP,指位于心动过速环路与希氏束之间的传导径路)来解释。心室起搏下逆传文氏CL(500ms)大于心动过速CL(450ms)证实存在LCP。随后,紧邻的A-A间期进行性延长至455~480ms,进一步达540ms,及突发缩短至440ms伴随A-H阻滞。令人感兴趣的是第5和第6个A-H间期与A-A间期一致。有几种机制可解释这些现象。简单的假设是由于LCP的递减性传导导致A-H间期进行性延长,LCP的递减性传导明显超过顺传AV结径路的递减性传导,从而引起LCP阻滞,表现为A-H阻滞。然而,这不能解释突发A-A间期缩短伴A-H阻滞。第二个假设是第5和第6个As转向慢径路,缓慢的LCP导致逆向A波提前于希氏束。随后,第7和第8个As是来自LCP上方高位折返点和LCP下方(LTP)低位折返点的二重激动所致。然而,在最初4个A-A间期,LCP的传导是进行性延长的,而顺向AV结径路传导只有5ms。因此,在随后的As,LCP阻滞的假设更有可能。最后,最有可能的机制是双心室反应伴LCP阻滞,即心动过速环路的前向冲动沿着快径路顺传,接着经LTP1折向逆向慢径路,伴随希氏束前LCP的阻滞(图3)。虽然在同一时间,顺传冲动显示双心室反应(图3,星标),顺向慢径路传导至LTP2,但因有效不应期而不能折向逆向慢径路。下一搏动也显示双心室反应。首先,顺向快径路传导至LTP1并折向逆向慢径路,与此同时,顺向慢径路递减传导至LTP2并折向逆向慢径路,此时逆向慢径路因A-A间期的较明显延长而恢复兴奋性并保持传导。然而,从顺向快径路折向逆向慢径路的冲动,因有效不应期而未能顺传至前向快径路和慢径路。由于这些传导径路,A-A间期缩短至440ms伴A-H阻滞。
长R-P间期心动过速伴不同A-H间期通常诊断为AT。然而,已有不典型AVNRT伴不同A-H间期的报道。这些报道证实不典型AVNRT时,与A-A间期延长相比A-H间期呈进行性延长。这一观察由心动过速环路以外的LCP加以证实。此外,双心室反应可以维持,从而产生1∶2的心动过速,这却被认为是非折返性SVT。非折返性SVT典型的表现为一个房性冲动同时经房室结双径路传导,其后希氏束和心室均被激动。本病例令人兴趣的要点是AVNRT期间A-A间期与A-H间期一致。这一观察可用心室双重反应伴LCP阻滞加以解释。据我们所知,这是通过双重心室反应来维持不典型AVNRT的首例病例。于后间隔慢径路逆传最早点行射频消融,成功消除心动过速且不能被诱发。
图1心内电图显示单一室性期前刺激(600/370 ms)伴V-A-V顺序诱发出窄综合波室上性心动过速。CS.冠状窦;HBE.希氏束电图;HRA.高位右房;RVA.右心室心尖。
图2心内电图显示室上性心动过速时A-A间期进行性延长和突发缩短。*心房和希氏束电位融合。
图3梯形图证实伴周长交替变化的室上性心动过速的机制。*心动过速环路前传冲动显示心室双重反应;快径(实线箭头)经低位折返点(LTP,称作LTP1)转向逆向慢径,伴低位共同径路(LCP)阻滞,而在同一时间,前传慢径路(虚线箭头)传至LTP2并转向逆向慢径路。AVN.房室结;LCP.低位共同径路。
[1]Hayashi T,Fukamizu S,Hojo R,etal.Identical Atrio-His Interval and A-A Intervals During Long RP Tachycardia:What Is the Mechanism?Circ Arrhythm Electrophysiol.2014;7∶352-354.
(童鸿)
