Appearance of a neural bypass between injured cingulum and brainstem cholinergic nuclei of a patient with traumatic brain injury on follow-up diffusion tensor tractography images
2015-01-18HanDoLee,SungHoJang
Appearance of a neural bypass between injured cingulum and brainstem cholinergic nuclei of a patient with traumatic brain injury on follow-up diffusion tensor tractography images
The human brain is known to contain a maximum of eight cholinergic nuclei: the basal forebrain region: the medial septal nucleus (Ch 1), the vertical nucleus of the diagonal band (Ch 2), the horizontal limb of the diagonal band (Ch 3), and the nucleus basalis of Meynert (Ch 4); the brainstem: the pedunculopontine nucleus (Ch 5), the laterodorsal tegmental nucleus (Ch 6), and the parabigeminal nucleus (Ch 8); and the thalamus: the medial habenular nucleus (Ch 7) (Nieuwenhuys et al., 2008; Naidich and Duvernoy, 2009). The cingulum is the neural tract extending from the orbitofrontal cortex to the medial temporal lobe (Mufson and Pandya, 1984). The cingulum plays an important role in memory because it is a passage of the medial cholinergic pathway, which provides cholinergic innervations to the cerebral cortex after originating from Ch 1 and Ch 2 as well as Ch 4 (mainly) (Selden et al., 1998; Nieuwenhuys et al., 2008; Hong and Jang, 2010).
Diffusion tensor tractography (DTT), which is derived from diffusion tensor imaging (DTI), enables three-dimensional visualization and estimation of the cingulum (Concha et al., 2005). As a result, many DTI studies have reported on injury of the cingulum following brain injury (Kraus et al., 2007; Sugiyama et al., 2009; Wu et al., 2010). On the contrary, several studies have reported on the mechanism for recovery of an injured cingulum: recovery of an injured cingulum and neural bypass between an injured cingulum and brainstem cholinergic nuclei (Yeo et al., 2012; Seo and Jang, 2013, 2014; Yoo et al., 2014), however, this recovery mechanism has not been clearly elucidated so far (Yeo et al., 2012; Seo and Jang, 2014; Yoo et al., 2014).
In the current study, we report on a patient with traumatic brain injury in whom a neural bypass was found between an injured cingulum and brainstem cholinergic nuclei on follow-up DTTs.
A 13-year-old male suffered from head trauma resulting from a pedestrian car accident. The patient lost consciousness for 2 months and experienced post-traumatic amnesia for 4 months from the time of the accident. The patient’s Glasgow Coma Scale score was 5 on the day of head trauma. He received conservative management under the diagnosis of intraventricular hemorrhage in the lateral ventricle and diffuse axonal injury. The patient underwent rehabilitative management beginning at 1 month after onset. No specifc lesion was observed on brain MRI (T1-weighted, T2-weighted, and Fluid attenuated inversion recovery [FLAIR] images) performed at 5 months after onset (Figure 1A). The patient showed memory impairment at 5 months after onset: Wechsler Adult Intelligence Scale: 43, and the Memory Assessment Scale (MAS, global memory: 62 [1%ile], short term memory: 76 [6%ile], verbal memory: 69 [2%ile], and visual memory: 60 [1%ile>]) (Wechsler, 1981; Williams, 1991). However, his short-term memory impairment had recovered to normal range at 12 months after onset: Wechsler Adult Intelligence Scale: 43, and the Memory Assessment Scale (MAS, global memory: 64 [1%ile], short term memory: 91 [28%ile], verbal memory: 61 [1%ile>], and visual memory: 87 [19%ile]) (Wechsler, 1981; Williams, 1991). Five age-matched control subjects (fve male; mean age: 15.3 years, range: 11—17) with no history of neurologic disease were recruited for comparison of the configuration of the fornix.
DTIs were acquired twice, at 5 months and 12 months after onset, using a 1.5 T Philips Gyroscan Intera system (Philips, Ltd, Best, The Netherlands) equipped with a Synergy-L Sensitivity Encoding (SENSE) head coil using a single-shot, spin-echo planar imaging pulse sequence. For each of the 32 non-collinear diffusion sensitizing gradients, we acquired 60 contiguous slices parallel to the anterior commissure-posterior commissure line. Imaging parameters were as follows: acquisition matrix = 96 × 96, reconstructed to matrix = 192 × 192, feld of view = 240 mm × 240 mm, repetition time = 10,398 ms, echo time = 72 ms, parallel imaging reduction factor (SENSE factor) = 2, echo planar imaging factor = 59 andb= 1,000 s/mm2, number of excitations = 1, thickness = 2.5 mm. Eddy current-induced image distortions were removed using affne multi-scale two-dimensional registration at the Oxford Centre for Functional Magnetic Resonance Imaging of Brain (FMRIB) Software Library (FSL; www.fmrib.ox.ac. uk/fsl). DTI-Studio software (CMRM, Johns Hopkins Medical Institute, Baltimore, MD, USA) was used for evaluation of the CST. The CST was reconstructed using fbers passing through two regions of interest (ROIs) on the color map. The cingulums were reconstructed using fbers passing through two ROIs on the color map (green color: middle and posterior portion of the cingulum). Termination criteria were fractional anisotropy (FA) <0.15 and an angle change > 70°.
DTTs of the cingulum in control subjects originated from the basal forebrain and extended posteriorly along and over the corpus callosum. On both 5-month and 12-month DTTs of the patient, discontinuations were observed in both anterior cingulums. On 5-month DTT of the patient and control subjects, we did not observe any neural bypass between injured cingulum and brainstem cholinergic nuclei. However, on 12-month DTT, a neural bypass was observed between the right injured cingulum and right brainstem cholinergic nuclei (Ch 6 and 8) (Figure 1A).
discussion
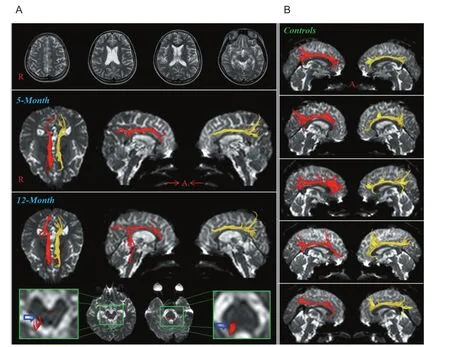
Figure 1 Conventional magnetic resonance (MR) images and diffusion tensor tractography (dTT) images of a 13-year-old male patient with traumatic brain injury.
Since introduction of DTI, a few studies have reported on a neural bypass between the injured cingulum and brainstem cholinergic nuclei (Yeo et al., 2012; Seo and Jang, 2014; Yoo et al., 2014). In 2012, Yeo et al (2012) reported on a patient with discontinuations in both anterior cingulums following TBI in whom a neural bypass was found between the left injured cingulum and left Ch 5. Subsequently, Seo and Jang (2014) reported on a patient in whom a neural bypass was found between an injured cingulum and brainstem cholinergic nuclei (Ch 5 and 6) in the brainstem on DTT following an aneurysmal subarachnoid hemorrhage. In a recent study, using DTT, Yoo et al. (2014) investigated the relation between cognition and the neural bypass between injured cingulum and brainstem cholinergic nuclei in chronic patients with traumatic brain injury. According to their findings, patients who had a neural bypass showed better short-term memory than patients who did not have such a neural bypass.
In conclusion, we report on a patient with traumatic brain injury in whom a neural bypass was found between the injured cingulum and brainstem cholinergic nuclei concurrent with recovery of short-term memory at chronic stage of traumatic brain injury. We believe that this case may suggest one of the mechanisms for recovery of an injured cingulum following traumatic brain injury and it can provide a basis for development of a new therapeutic modality for treatment of an injured cingulum However, our results are limited to this case report. Further studies involving larger numbers of patients are required.
This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology, No. 2012R1A1A4A01001873.
Han Do Lee, Sung Ho Jang*
Department of Physical Medicine and Rehabilitation, College of Medicine, Yeungnam University, 317-1, Daemyung dong, Namku, Daegu, Republic of Korea
*Correspondence to: Sung Ho Jang, M.D., strokerehab@hanmail.net.
随着一个国家或地区的劳动力成本上升,将不利于劳动密集型产业发展,而有利于资本密集型和技术密集型产业发展,其产业结构高度会得以提升。
Accepted:2014-12-27
Concha L, Gross DW, Beaulieu C (2005) Diffusion tensor tractography of the limbic system. AJNR Am J Neuroradiol 26:2267-2274.
Wechsler D (1981) Manual for the wechsler adult intelligence scale-revised. New York: Psychological Corporation.
Gazzaniga MS, Ivry RB, Mangun GR (2009) Cognitive Neuroscience: the Biology of the Mind, 3rdEdition. New York: W.W. Norton.
Harding L, Beech JR (1996) Assessment in Neuropsychology. London; New York: Routledge.
Hong JH, Jang SH (2010) Neural pathway from nucleus basalis of Meynert passing through the cingulum in the human brain. Brain Res 1346:190-194.
Kraus MF, Susmaras T, Caughlin BP, Walker CJ, Sweeney JA, Little DM (2007) White matter integrity and cognition in chronic traumatic brain injury: a diffusion tensor imaging study. Brain 130:2508-2519.
Miranda MI, Ferreira G, Ramirez-Lugo L, Bermudez-Rattoni F (2003) Role of cholinergic system on the construction of memories: taste memory encoding. Neurobiol Learn Mem 80:211-222.
Mufson EJ, Pandya DN (1984) Some observations on the course and composition of the cingulum bundle in the rhesus monkey. J Comp Neurol 225:31-43.
Naidich TP, Duvernoy HM (2009) Duvernoy’s Atlas of the Human Brain Stem and Cerebellum. New York: Springer.
Nieuwenhuys R, Voogd J, Huijzen CV (2008) The Human Central Nervous System, 4thEdition. New York: Springer.
Selden NR, Gitelman DR, Salamon-Murayama N, Parrish TB, Mesulam MM (1998) Trajectories of cholinergic pathways within the cerebral hemispheres of the human brain. Brain 121:2249-2257.
Seo JP, Jang SH (2013) Recovery of injured cingulum in a patient with brain injury: diffusion tensor tractography study. NeuroRehabilitation 33:257-261.
Seo JP, Jang SH (2014) Unusual neural connection between injured cingulum and brainstem in a patient with subarachnoid hemorrhage. Neural Regen Res 9:498-499.
Sugiyama K, Kondo T, Oouchida Y, Suzukamo Y, Higano S, Endo M, Watanabe H, Shindo K, Izumi S (2009) Clinical utility of diffusion tensor imaging for evaluating patients with diffuse axonal injury and cognitive disorders in the chronic stage. J Neurotrauma 26:1879-1890.
Williams JM (1991) MAS: Memory Assessment Scales: Professional Manual. Odessa, Fla.: Psychological Assessment Resources.
Wu TC, Wilde EA, Bigler ED, Yallampalli R, McCauley SR, Troyanskaya M, Chu ZL, Li XQ, Hanten G, Hunter JV, Levin HS (2010) Evaluating the relationship between memory functioning and cingulum bundles in acute mild traumatic brain injury using diffusion tensor imaging. J Neurotrauma 27:303-307.
Yeo SS, Chang MC, Kim SH, Son SM, Jang SH (2012) Neural connection between injured cingulum and pedunculopontine nucleus in a patient with traumatic brain injury. NeuroRehabilitation 31:143-146.
Yoo JS, Kim OL, Kim SH, Kim MS, Jang SH (2014) Relation between cognition and neural connection from injured cingulum to brainstem cholinergic nuclei in chronic patients with traumatic brain injury. Brain Inj 28:1257-1261.
Copyedited by Bazeed MF, Kanat A, Li CH, Song LP, Zhao M
10.4103/1673-5374.153702 http∶//www.nrronline.org/
Lee HD, Jang SH (2015) Appearance of a neural bypass between injured cingulum and brainstem cholinergic nuclei of a patient with traumatic brain injury on follow-up diffusion tensor tractography images. Neural Regen Res 10(3)∶498-500.
猜你喜欢
杂志排行

中国神经再生研究(英文版)的其它文章
- RAFting the rapids of axon regeneration signaling
- TAM receptors: two pathways to regulate adult neurogenesis
- Synapsing with NG2 cells (polydendrocytes), unappreciated barrier to axon regeneration?
- Targeting the body to protect the brain: inducing neuroprotection with remotely-applied near infrared light
- Novel advancements in threedimensional neural tissue engineering and regenerative medicine
- Functional regeneration of the brain: white matter matters