Comparison of the psychological status and quality of life of elderly urban Shanghai residents who receive different types of support services
2011-07-08HongZHEBGSiLuCHEBYieiJIHuaTAOWeiDongJI
Hong ZHEBG,Si Lu CHEB,Yi W ei JI,Hua TAO,Wei Dong JI
Comparison of the psychological status and quality of life of elderly urban Shanghai residents who receive different types of support services
Hong ZHEBG1*,Si Lu CHEB2,Yi W ei JI3,Hua TAO1,Wei Dong JI1
Background:In large urban centers in China three common methods have evolved to provide services to the rapidly increasing numbers of elderly residents:traditional family support in the home;supplemental home visits by community service workers;and residential nursing homes for the elderly.The differential effects of these services on the quality of life,social support and psychological functioning of the urban elderly have not been systematically assessed.
Hypothesis:The elderly receiving home visit services have a higher quality of life,better social support and less psychological symptoms than those w ho only receive family support or w ho have moved to live in nursing homes.
Methods:Using cluster sampling methods,persons 65 years of age or older receiving three types of services—community-based home services,traditional family support,and residential home placement—were identified(100 persons for each type)and administered the 36-item Medical Outcome Study Short Form health survey(SF-36),the Social Support Rating Scale(SSRS)and the Symptom Checklist90(SCL-90).
Results:There w ere no significant differences in gender,marital status,monthly income or educational level between the three groups but the mean age of the residential home residents w as somewhat higher.The mean scores for all eight subscales on the SF-36 were higher in the community-based services group and traditional family support group than in the residential home group,but there w ere no significant differences betw een the communitysupport group and the traditional family support group.The mean(SD)SSRS social support measure w as higher in the community-based home services(A)subjects than in the family support(B)and residential home(C)groups[36.8(4.4),25.3(6.7)and 20.0(30.4),respectively;F2,297=12.78,P<0.001;A>B>C]and the overall level of psychological symptom s assessed by SCL-90 was lower in the community-based home services subjects and family support subjects than in the residential home subjects[129.9(38.7),131.6(28.4)and 139.0(31.2),respectively;F2,297=8.98,P=0.004;A,B<C].The mean score of some of the SCL-90 subscales—somatization,interpersonal sensitivity,paranoid ideation,and psychoticism—were significantly higher in the family care group than in the community services group.These differences all remained significant after adjustment for demographic variables.
Conclusion:Compared to elderly residents receiving traditional family support or those w ho have moved to residential homes,those provided community-based social services in their ow n homes report more robust social support networks.The quality of life and psychological health of elderly who stay in their own homes or in the homes of their relatives are better than those of elderly residents w ho move to a residential home.Prospective cohort studies are needed to confirm these cross-sectional results.
Community services;Retirement homes;Elderly;Social support;Quality of life;Psychological symptoms
1 Introduction
A study in late 2005 found that there were 144 m illion persons over 60 years of age in China,accounting for 11%of the population,and the authors estimated that this proportion would increase to 20%by 2025 and to 25%by 2050[1].Thus, China is a rapidly aging country both in terms of the overall proportion of elderly in the population and in term s of the rate of increase in the proportion of elderly.At the same time the one-child-per-family population control policy has led to a rapid decrease in the size of urban families,so the traditional method of supporting the elderly-moving them to live with children or other relatives—is becoming less and less viable.
The aging of the Shanghaipopulation has been about20 years ahead of that of the rest of the country.To address the challenges of this demographic transition the Shanghai government starting experimenting with a community-centered model for supporting the elderly that was based on the experiences of Japan,England and other countries.The‘11 th Five-year Economic and Social Development Plan of the Shanghai Municipality’(released in 2005)clearly specified that by 2010 10%of the Shanghai’s elderly population would receive community based social services,including at least 250,000 who would receive community-base home help and 100,000 who would receive support in residential homes[2].The Changning District in central Shanghai took the lead in providing elderly services,developing a service netw ork that included basic living support,health care,social services, community participation,rights protection,and a three-tiered adm inistrative network for providing services to the elderly[3].
Three different models of support for the elderly are available in Changning.The communitybased home care component of the service system provides professional in-home care,nursing,housekeeping and emotional support during the daytime as w ell as encouraging participation in a w ide range of community activities[4].Community-based service centers with professionally trained staff provide the home services,though the family remains the main source of psychological support,and the cost is jointly borne by the state,the community, the family and the individual[5].Participation in the home care program is voluntary;individuals who need support services or their family members apply for the service,an evaluator visits the home to make an assessment and then the community service center decides whether or not to approve the request.The services are relatively inexpensive,typically costing 300-800 Yuan($50-$120)per month depending on the types of services requested(meals,washing clothes,assistance bathing,physical rehabilitation,etc.);those with financial difficulties can request a government supplement to cover some or most of this cost.The second component of the service system are community-based residential homes for the elderly that provide 24-hour care and supervision;these are funded by the state or,in some cases,by private organizations[6]. The third component of the service system is the traditional family-supportmodel in which the elderly person lives on their own or with blood relatives(but does not participate in the home care program)and is supported financially and emotionally by their family members;over 90%of the elderly in Shanghai still rely on this type of family support.
This survey compares the quality of life,social support and psychological health of elderly residents of Changning District who have received these three different types of services:communitybased home care,residential home care,or traditional family-based care.
2 Subjects and methods
2.1 Subjects
Permanent residents of Changning District 65-89 years of age who do not have any serious physical or psychological illnesses that would interfere with their ability to participate in the survey and who have continuously participated in one of the three types of support services(i.e.home care,residential care,or family care)for the last tw o years are eligible to participate in the survey.
This survey was conducted between February and May of2009.A cluster random samp ling method was used to identify participants(see Figure 1). Two of the 10 sub-districts of Changning District were random ly selected(Huayang and Jiangsu)and then 3 neigborhoods were random ly selected from each of these sub-districts(a total of 6 neigborhoods from the 34 neighborhoods in the two sub-districts).The subjects were selected as follow s:
·Family-supportsample.Based on the resident registry system s for the neighborhoods 973 elderly individuals in the 6 neigborhoods had received family-support(w ithout any additional community-support services)for the prior two years:households were visited consecutively(based on street number)until100 surveys were com pleted;in 4 cases the individuals refused or w ere unable to comp lete the survey.
·Community-basedhomeservicessample.Based on the services records in the sub-district offices 258 elderly individuals from the 6 neigborhoods w ho had continuously received communitybased home services for the prior two years were identified:the names were sorted by the stroke count in the character for their family name and then the households were consecutively visited until 100 surveys were com pleted;4 subjects refused or w ere unable to comp lete the survey.
·Residentialhomecaresample.There are three residential homes for the elderly in the two subdistricts;one small home w here most of the 30 residents had dementia was not selected.The re-maining tw o residential homes had a total of245 eligible residents.The names were sorted by stroke count of the character for their family name and then interviewed in order until 100 surveys w ere com pleted;5 identified subjects refused or w ere unable to comp lete the survey.
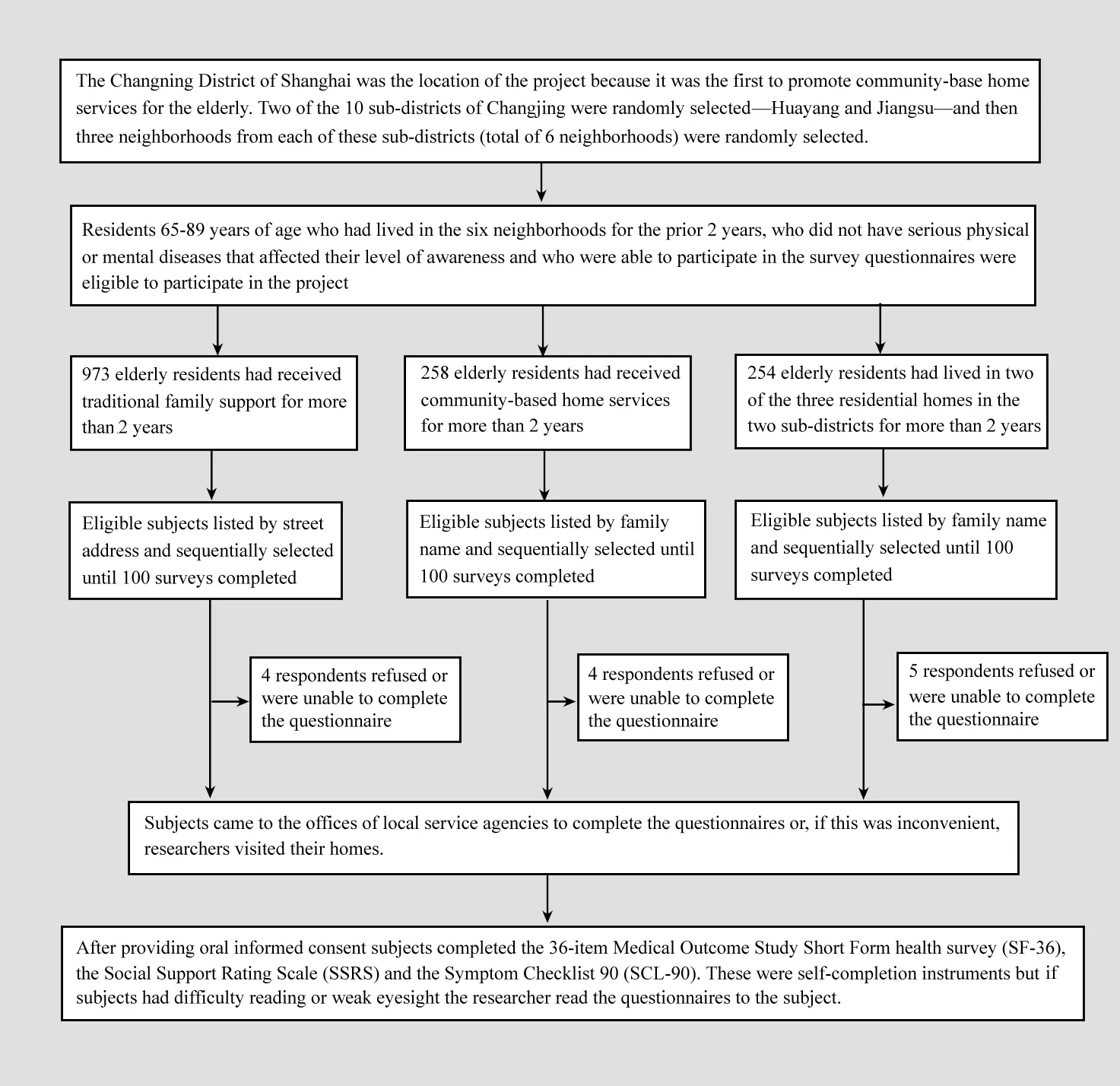
Figure 1.Flow chart of the course of the study
2.2 Questionnaires
Quality of life was measured with the 36-item Short Form Health Survey(SF-36)[7]which was administered as a self-completion instrument.This scale has been used to assess quality of life in a w ide range of countries.The 36 items are divided into eight domains:physical functioning,role limitations due to physical health problems,bodily pain,general health,vitality,social functioning,role limitations due to emotional health problem s,and mental health.The raw score for each subscale is transformed into a standard score with a range of 0 to 100,with higher scores representing better quality of life.Liu and colleagues[8]report that the SF-36 is a reliable and valid measure of the quality of life of elderly community residents in China.
The level of psychological symptoms was assessed using the Symptom Check List-90(SCL-90)[9].This is a self-report scale with 90 item s that uses a 5-point Likert scale response set to assess how distressed the individual is by different symptoms over the prior week(1=notatall,5=extremely).The items are classified into ten primary symptom dimensions:somatization,obsessive-compulsive behavior,interpersonal sensitivity,depression, anxiety,hostility,phobic anxiety,paranoid ideation,psychoticism,and other symptoms.Each of the item s is rated on a five-point scale of distress(1-5)ranging from"not at all"to"extremely."The total score is the sum of all 90 item s;the higher the score the more severe the psychological symptoms.
The Social Support Rating Scale(SSRS)[10]is a self-com pletion instrument that is divided into three subscales:objective support,subjective support,and utilization of social support.Higher total score or subscale scores reflect better social support.Liu and colleagues[11]have noted that the scale has good reliability and validity in China.
W e also constructed a brief questionnaire to record background information on the subjects.This included item s about gender,age,current marital status,current and previous living circumstances,access to health insurance,monthly income and expenses,use of community services, willingness to accept psychological services and so forth.Monthly expenses were estimated by the respondent as the total of the monthly expenditures for meals,utilities,medical expenses,expenses for different types of services,and so forth.
2.3 Conductofthesurvey
All subjects in the home-care program were interviewed in the local day-care center;87 of the subjects in the traditional family care group came to the household committee offices to complete the survey and interviewers went to the homes of13 of these subjects;and all 100 subjects in the residential home group were interview ed in the residential homes.After providing written informed consent respondents completed the form s.Four subjects(1 from the home care group,1 from the traditional family support group,and 2 from the residential care group)had difficulty reading so the questionnaires were read to the subjects by the investigator.
This study was approved by the institutional review board of the district mental health center.
2.4 Statisticalanalysis
Questionnaire data was entered using Epidata3.0andanalyseswereconductedusingSPSS16.0.Chi-square tests and ABOVA were used to assess statistical difference among these three groups and multiple comparison tests were used to make pairwise comparisons if the overall test indicated that there were statistical differences between the groups.
3 Results
3.1 Characteristicsoftherespondents
As show n in Table 1,there were no significant differences by gender,marital status,monthly income or educational status between the three groups.However,subjects living in the residential homes were somewhat older that those who had remained in their homes and were receiving community-based support or traditional family care.Elderly individuals in residential care facilities—w ho were no longer living independently or with relatives—were also paying more for support,least satisfied with the support they were receiving and least willing to accept professional psychological services than those in the other two groups.Individuals receiving community-base home care reported higher levels of satisfaction with their support network than elderly living with relatives w ho did not receive community-based home care.

Table 1.Comparison of the characteristics of elderly Shanghai residents receiving three different types of support
3.2 ComparisonofScaleScores
Comparisons of the quality of life,social support and psychological symptoms of subjects in the three groups are shown in Table 2.For all three measures elderly receiving community-based home care had the best outcomes and elderly in residential care had the worst outcomes.The significant differences reported in Table 2 all remained statistically significant after ad justment for the age differences across the groups.

Table 2.Comparison of SF-36,SSRS and SCL-90 mean(SD)total scores and subscale scores of elderly Shanghai residents receiving three different types of support
As assessed by the 8 subscales of the SF-36,all dimensions of quality of life were worse in elderly residents of residential homes than in those receiving community-based services or traditional family support.Bone of the eight dimensions of quality of life showed a statistically significant difference between the community-support group and the traditional family support group.
The overall social support was significantly greater in the home services subjects than in the other two groups and greater in the traditional family support group than in the residential home group;these relationships w ere also found for the three SSRS subscales-objective support,subjective support and utilization of support.
The overall level of psychological symptoms was greater in subjects who had moved to residential homes than in the subjects who remained intheir own homes or in the homes of their relatives;this was also true for 7 of the 10 SCL-90 subscale scores.Some of the symptoms-somatization,interpersonal sensitivity,paranoid ideation and psychoticism—w ere less severe in the community-based home services group than in the traditional family support subjects.
4 Discussion
4.1 Mainfindings
Our study goes beyond previous work on the quality of life of the elderly in China[12,13]by comparing quality of life,social support and psychological symptom s of individuals who participated in three different types of service models.W e found differences betw een the three groups of subjects that do not appear to be a function of the slightly older age of those living in the residential care facilities.Elderly subjects living in their ow n homes(with their spouse or with other family members)w ho get the additional community-based home care package of services report a stronger social support network than those who live in their own homes or with other family members w ho do not receive these services.And both groups living in their own homes or with family members,regardless of whether or not they receive communitybased home services,report a higher quality of life, better social support networks and less psychological symptoms than those living separately from their family members in residential care facilities.The participants in the community-based home care services also report a greater acceptability of receiving psychological help than those in the other two groups,suggesting that participation in the home care services program increases their w illingness to consider accepting non-traditional forms of help from professionals or persons who are not family members.
Given the cross-sectional nature of the study,it is not possible to prove a causal relationship between the different forms of care and the better outcomes in the community-based home care group. However,all subjects in the survey had been receiving a single type of social support service for a minimum of two years and—with the exception of the slightly higher age in the residential care group—their demographic characteristics were similar,so the findings are quite suggestive that the provision of home care services does,in fact,im prove the social support networks and some of the psychological symptoms of elderly urban residents.Individuals living in residential care facilities are more isolated from their family members and from the community at large so the poorer outcomes in this group could be explained by their different social circumstances.The better outcomes in the communitybased home care group compared to those in the traditional family support group(w ithout structured home care services)might be due to the services provided.However,prospective studies will be needed to confirm that the results are not due to a selection bias that resulted in the voluntary enrollment of elderly w ho would have better outcomes in the home care program.
The origin of the community-based home care model of services for the elderly in China was in Dalian(a city in Liaoning Province)where they adapted models used in Japan,Great Britain and other western countries that used governmental resources to purchase services that w ere provided by a variety of agencies coordinated by professional community workers.Recently the rapid aging of the population,the simultaneous weakening of the ability of families to support their elderly,and the inability of the government to provide sufficient placements in residential facilities led to the rapid development of home care service models for the elderly in different parts of China[14].A Shanghai-wide survey[15]found that70%-90%of the elderly preferred to stay in their homes in their final years of life so starting in 2000 the Shanghai government started developing its own model of home services which eventually resulted in the three-component system assessed in the current survey.
Changning District in central Shanghai is relatively affluent and has a high-quality medical care system.Persons aged 60 or over account for21%of the total population of the district and a survey of 13,000 elderly residents found that12%live alone, 42%live with other elderly persons and 6%live in residential homes for the elderly[16].Despite having access to a variety of different types of residential facilities most elderly wanted to stay in their own homes.This made Changning an excellent location to develop a new model of services for the elderly. The district w as the first in Shanghai to establish six target criteria for providing high-quality community services for the elderly:1)provide financial support for all elderly who have no other source of support, 2)provide local health services that establish a medical record for all elderly citizens and provide regular follow-up of chronic conditions,3)provide home meals or community dining services,day care centers,community cultural activity centers,and similar institutions that provide essential social services,4)provide diverse cultural and recreational collective activities that promotes social participation,5)establish a legal consultation service for the elderly that is free of charge for those who can’t afford the service in each local community,and 6)create a three-tiered administrative network for managing services for the elderly with dedicatedfulltime staff.
Based on these criteria the Changning District has gradually built up this three-part model of services over the last decade.Over 12,000 elders have already received support from the network.W e believe that the community-based home care model provides the combined benefit of keeping elderly individuals in the family environment and maximizing their participation in social and community activities.As shown in our results,the cost to the family or the individual is not significantly different from the cost of providing traditional family-centered care,and those who cannot afford the relatively inexpensive charge can apply for a government supplement,so financial access to the services is assured.This model deserves to be assessed in more detail and,if our results are confirmed in prospective studies,it should be adapted for use in other urban communities that are trying to develop a range of services to meet the different types of needs of their elderly citizens.
4.2 Limitations
This is a cross-sectional study so it is not possible to conclude that the type of services have resulted in the reported differences between the three groups of subjects.The sample was reasonably representative of elderly residents who received the three types of services in Changning District,but Changning District has taken the lead in developing innovative models of community-based home services for the elderly in Shanghai so it is uncertain how easy it will be to transplant this model to other urban locations where the enthusiasm and resources available for elderly services may be less.Bor would the model be appropriate for rural communities because of the greater dispersion of the rural population.And the study is focused on the healthy elderly,specifically excluding those with serious illnesses,so it only assesses one aspect of the service system for the elderly;the overall quality of the support system for the elderly must also consider how w ell it helps elderly citizens who develop serious disabling or life-threatening conditions.
4.3 Implications
Our findings confirm previous work in China that show a relationship between strong social support networks and mental health in elderly individuals[12,13].Our data suggests that providing a variety of service options for the urban elderly can im prove their support networks and decrease some of their psychological symptoms,but much more work is needed refine these methods,to test their effectiveness,and to determ ine how best to adapt effective models to other communities,particularly rural communities.Most importantly,the extent to which social engineering activities(such as providing home care services)can actually im prove social support,psychological health and the quality of life in elderly individuals will remain uncertain until long-term,prospective studies in relatively large samples are conducted.The societal resources that will need to be invested in the elderly over the coming decades are substantial so it is imperative that the research community conduct the types of projects that will identify different cost-effective,evidence-based practices that will help policy makers efficiently use these resources.
Acknowledgement:
This survey was supported by the Mental Health Department of the Shanghai Changning District Center for Disease Control,by the leaders and social services departments of the Huayang and Jiangsu sub-districts,and by the doctors in the mental health service offices of these communities.The authors thank the administrators and doctors working in these institutions for their help with the data collection.
1. Liu LP,Jiang SY,xu DY,Huang Y.Development trend of oldage service style in urban area.Chin J Community Medicine, 2008,6(7):44-46.(in Chinese)
2. 11thFive-year Econom ic and Social Development Plan of the Shanghai Municipality.Shanghai Government〔2006〕Docum ent Bumber 5.March 2006.(in Chinese)
3. Liu F.Establishment of old-age service system in Changning District of Shanghai.Chin J Gerontology,2010,30(12):1762-1764.(in Chinese)
4. Luo xR.Practices of social construction:exploration and enlightenment of the community-home old-age service.J Jiangxi Adm inistration Institute,2008,10(4):63.(in Chinese)
5. Chen DY.Exploration of the family support of the elderly.Aerospace Industry Management,1998,(9):12-14.(in Chinese)
6. Yang WZ.Exploration of family old-age service model in urban of China during the period of social transformation.J W uhan University:Philosophy Social Science Edition,1998,5:15-19.(in Chinese)
7. Zhang ZJ.Handbook of behavioral medical scales.Beijing: Chinese Medical Multimedia Press,2005:54-59.(in Chinese)
8. Liu JB,Jiang YH,Liu YT.Reliability and validity of SF-36 among the elderly living in communities.Chin JBehavior Medical Science,2001,10(3):65-67.(in Chinese)
9. Chen CH.Sym ptom checklist90.Chin Mental Health J,1999, 13(Supple):31-35.(in Chinese)
10. x iao SY.Social support scale.Chin Mental Health J,1999,13(Supp le):127-131.(in Chinese)
11. Liu JW,Li FY,Lian YL.Reliability and validity of social support scale.Jxinjiang Medical University,2008,31(1):1-3.(in Chinese)
12. Jiang QP,Sun D,Su SY,Liu J,Li JF.Com parison of life quality betw een the elderly living with fam ilies and the elderly living in organizations.Shanghai Arch Psychiatry,2005,17(2):78-79.(in Chinese)
13. Sun Yx,W ang JJ.Mental health of the elderly having different kinds of old-age service Chin JGerontology,2007,27(4):376-377.(in Chinese)
14. Zhang WD.Theoretical basis for the home-based care model for the elderly.Chin J Gerontology,2000,20(3):120-122.(in Chinese)
15. Han MJ.Exploration of community-home old-age service model. Medical JChin Peopleˊs Health,2009,21(12):1393.(in Chinese)
16. Yang xD.Ageing of population and the developmentof elderly health in Shanghai.J Community Healthcare,2003,(2):81.(in Chinese)
17. Wang LF,Shi YJ.Relationship of social support and mental health status in the urban em pty-nest elderly.Chin Mental Health Jl,2008,22(2):118-122.(in Chinese)
18. Huang JQ,Chen QE,Shu xF.Relationship of social support and life quality in elderly living in communities.Chin JBehavior Medical Science,2005,14(8):725-726.(in Chinese)
19. Martis B,Alam D,Dow d SM,Hill SK,Sharma RP,Rosen C,et al.Beurocognitive effects of repetitive transcranial magnetic stimulation in severe major depression.Clin Beurophysiol. 2003,114(6):1125-1132.
20. Austin MP,M itchell P,Goodw in GM.Cognitive deficits in depression:possible im p lications for functional neuropathology. Br J Psychiatry,2001,178:200-206.
21. Li Z,Sun x L,Huang Y,Zhang B.The relationship of neurohormones and cognitive functioning in treatment-resistant depression.Chin J Evidence-Based Med,2007,7(8):575-579.(in Chinese)
22. Hausmann A,Pascual-Leone A,Kemm ler G,Rupp CI,Lechner-Schoner T,Kramer-Reinstadler K,et al.Bo deterioration of cognitive performance in an aggressive unilateral and bilateral antidepressant rTMS add-on trial.J Clin Psychiatry,2004,65(6):772-782.
23. Loo C,Sachdev P,Elsayed H,McDarmont B,M itchell P,W ilkinson M,et al.Effects of a 2-to 4-week course of repetitive transcranial magnetic stimulation(rTMS)on neuropsychologic functioning,electroencephalogram,and auditory threshold in depressed patients.Biol Psychiatry,2001,49(7):615-623.
[received:2010-06-22;accepted:2010-12-22]
10.3969/j.issn.1002-0829.2011.02.003
1Changning District Mental Health Center,Shanghai200333;2Jing’an District Mental Health Center;
3Jiangsu Community Health Service Center,Shanghai200050
*Correspondence:zhhmm2@163.com
