Quality of life of hospitalized patients after lung cancer operation and analysis of influencing factors
2023-11-20HUYifanHUANGXiumingXIAOShaZHOUJingWANGShuominWUQishengZHOUBingxianFANShihengFANYayanCHENXianshanZHANGJing
HU Yi‑fan, HUANG Xiu‑ming, XIAO Sha, ZHOU Jing, WANG Shuo‑min, WU Qi‑sheng, ZHOU Bing‑xian, FAN Shi‑heng, FAN Ya‑yan, CHEN Xian‑shan✉, ZHANG Jing✉
1.International School of Public Health and Whole Health, Hainan Medical University, Haikou 571199,China
2.Department of Thoracic Surgery, Hainan Hospital Affiliated to Hainan Medical College, Hainan Provincial People's Hospital, Haikou 571199,China
Keywords:
ABSTRACT Objective: To explore the current status and influencing factors of quality of life in patients with lung cancer after surgery in a tertiary hospital in Hainan province.Methods: To investigate the influencing factors of quality of life of lung cancer patients after surgery in a tertiary hospital in Hainan province by cross‑sectional survey method.Results: The scores of insomnia, appetite loss, constipation and pain in 186 lung cancer patients after surgery in a tertiary hospital in Hainan Province were significantly higher than the reference value.Multiple linear regression analysis showed that older patients (> 60 years) had lower scores in physical function domain (β=‑0.193), and female patients had more appetite loss symptoms(β=0.245).Compared with other minority ethnic groups, Han ethnic group had lower scores in role function domain (β=0.179), more severe fatigue symptoms (β=‑0.162), and higher general health level (β=0.166).Patients with employee medical insurance had lower scores of emotional function (β=0.194), cognitive function (β=0.281), the lowest score in social function (β=0.188), and severe pain in other parts (β=‑0.227).Smokers had less cough symptoms (β=0.175) and more arm and shoulder pain symptoms (β=‑0.21) than non‑smokers.Patients with secondhand smoke exposure had lower cognitive function scores(β=‑0.158) and more obvious symptoms of oral ulcer (β=0.185).Patients who drank alcohol frequently (drinking frequency > 1 time/day) had more severe cough symptoms (β=0.27).Patients with small number of children (0‑1) had milder cough symptoms (β=0.178).Patients who did not understand the disease had obvious symptoms of arm and shoulder pain (β=0.151).Patients with early pathological stage (stage I‑II) had more severe shortness of breath (β=‑0.159) and pain (β=‑0.181).The symptoms of appetite loss were more obvious in patients living in cities (β=0.192).The symptoms of peripheral neuropathy were more obvious(β=0.174).Patients who often consumed pickulated food had severe pain symptoms (β=‑0.219), and pain in other parts was obvious (β=‑0.149).Male patients had obvious alopecia symptoms (β=‑0.306).Conclusion: Age, ethnicity, residence, type of medical insurance,number of children, pathological stage of lung cancer, smoking, second‑hand smoke exposure,alcohol consumption, and frequent consumption of pickled food were related to the quality of life of lung cancer patients in hospital after surgery.Medical staff and family members should pay attention to the emotional communication of patients during the treatment of lung cancer patients in hospital after surgery.Patients should avoid exposure to smoking, alcohol and second‑hand smoke, and reduce consumption of pickled food.
1.Introduction
The epidemiological research and preventive interventions of lung cancer have changed significantly in the past decade.Despite progress in our cognition of the risk, development, immune control and treatment options of lung cancer, lung cancer is still a serious threat to people’s health and is a major public health problem second only to cardiovascular diseases[1,2].In order to control the development of lung cancer patients and improve the survival rate of lung cancer patients, our country mainly uses surgical treatment combined with radiotherapy, chemotherapy, gene targeted drugs and immunotherapy as adjuvant treatment[3,4].With the development and application of thoracoscopic technology, which has greatly reduced the treatment wound, surgical treatment will still cause inevitable physical and psychological damage to patients with lung cancer.During the diagnosis and treatment period, patients in hospital after lung cancer surgery not only suffer from a variety of symptoms caused by surgery and postoperative recovery, including cough, expectoration, hemoptysis, pain and other symptoms,but also accompanied by postoperative infection, impaired lung function, atelectasis, pulmonary air leakage, arrhythmia and other complications, and patients have limitations in their own disease cognition.The interaction of the above conditions increases the physical and mental burden of hospitalized patients after lung cancer surgery, thus affecting the treatment and long‑term prognosis[5-8].
Modern medicine is no longer a biomedical model that simply evaluates the health of patients by observing their condition and survival time.With the development of bio‑psycho‑social model,the evaluation of the quality of life of patients is becoming more and more important.The diagnosis and treatment of lung cancer will cause many negative physical and psychological effects on patients.Studies have found that patients with lung cancer will gradually develop negative emotions such as worrying about expensive treatment costs, poor prognosis of the disease, and increasing the burden of life for their families during the process of diagnosis and treatment, which will lead to a serious decline in the quality of life of patients with lung cancer[9].From September 2021 to June 2022,our research group investigated the quality of life and its influencing factors of patients with lung cancer after surgery in a Class ⅲ Grade A hospital in Hainan Province.Compared with previous studies on the quality of life of lung cancer patients, our research group focused on the patients with lung cancer who underwent surgery in a short period of time, and investigated the patients in combination with social and demographic factors in Hainan Province.To provide relevant suggestions and improvement measures for improving the quality of life of patients with lung cancer after surgery in Hainan province.
2.Objects and Methods
2.1 Respondents
A cross‑sectional study was conducted in this study.The quality of life of patients after lung cancer surgery in hospital was evaluated and the required information was obtained by consulting medical records and questionnaire survey.The subjects of the survey were lung cancer patients within five days after surgery who were hospitalized in the Thoracic Surgery Department of a tertiary hospital in Hainan Province from September 2021 to June 2022.Inclusion criteria: (1) Primary lung cancer confirmed by surgery or pathology; (2) patients voluntarily participated in the survey;(3) history of unconscious disorders and mental diseases; (4) can complete the investigation by themselves or with the help of others;Exclusion criteria: patients with mental system diseases had serious heart, brain, liver, kidney, vascular system diseases or urinary,blood, digestive system diseases.A total of 211 questionnaires were distributed and 186 valid questionnaires were returned, with an effective recovery rate of 88.15%.This study was approved by the Ethics Committee of Hainan Medical University (HYLL‑2021‑156), and patients signed informed consent for the content of this investigation.
2.2 Content of the questionnaire
A self‑designed social demographic questionnaire based on the specific conditions of Hainan province and a clinical disease table were used to collect the basic data and diagnosis and treatment characteristics of patients after lung cancer surgery in the hospital.
2.2.1 EORTC QLQ‑C30 scale
A total of 30 items were included in five functional domains:body, role, cognition, emotion and society.The symptoms included fatigue, pain, nausea and vomiting.1 global quality of life domain;There were 6 single symptom items of shortness of breath, insomnia,anorexia, constipation, diarrhea and financial difficulties; The Cronbach’s α coefficient of the scale was 0.92.
2.2.2 EORTC QLQ‑LC13 scale
A total of 13 items included 10 symptom domains such as shortness of breath, cough, hemoptysis, oral ulcer, dysphagia, peripheral neuropathy, alopecia, chest pain, arm/shoulder pain, and pain in other parts of the body.The Cronbach’s α coefficient of the scale was 0.68.
2.2.3 Conversion of score
The original scores of each item were converted to standard scores from 0 to 100 by linear formula.Higher scores in the functional domain and global quality of life domain indicate better functional status and better quality of life.The higher the score of symptom domain and single symptom, the more severe the symptoms and the worse the quality of life.
2.3 Statistical processing
EpiData was used to establish a database, two people entered the data, and SPSS 25.0 was used for data analysis.The demographic characteristics, clinical characteristics and the scores of each domain of quality of life of the patients were analyzed by descriptive statistics, and the scores of each domain of quality of life were expressed as±s.With the scores of each field of quality of life as dependent variables and the demographic characteristics and clinical characteristics of patients as independent variables, multiple linear regression analysis was used to analyze the influencing factors of quality of life of patients after lung cancer surgery in the hospital.P<0.05 was considered statistically significant.
3.Results
3.1 General condition
The age of the subjects ranged from 27 to 86 years, with an average age of 61.83±11.42 years.60.8% of the subjects were 60 years old, including 96 males (51.6%).Most of the participants were of Han nationality (94.6%), 57.5% of them lived in rural areas, 82.8%of them had education level of high school or below, 79.6% of them had multiple children, only 5.4% of them had family history of malignant tumor, and 63.4% of them had middle and high level of income.81.2% of the patients were aware of their disease, and 57.5% of the subjects had resident medical insurance.The main pathological types were adenocarcinoma (91.9%) and squamous cell carcinoma (5.4 %).The most common clinical stage was stageⅠ (76.9%), stage Ⅱ (8.1%), stage Ⅲ (7.0 %) and stage Ⅳ (8.1%).54.8% of the patients had no history of smoking, 53.8% of the patients had a history of second‑hand smoke exposure, 76.9% of the patients did not often drink alcohol, and 17.7% of the patients often ate pickled food.See Table 1 for details.
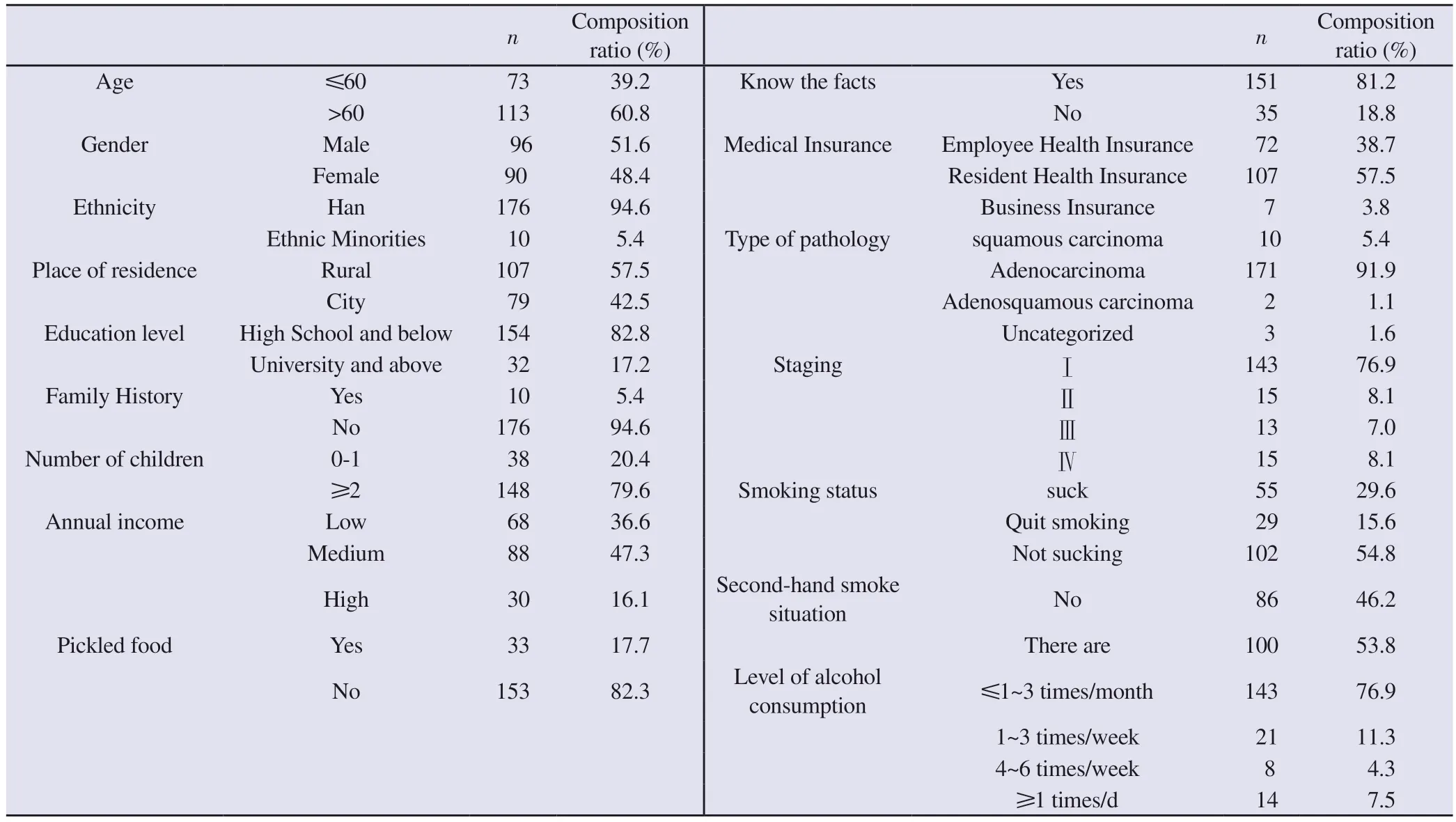
Tab 1 Demographic and clinical characteristics of hospitalized patients after lung cancer surgery (n=186)
3.2 Standardized scores in all areas of the Quality of Life scale
Among the five functional fields of EORTC QLQ‑C30, the role function score of hospitalized patients after lung cancer surgery was lower (54.75±25.54), and the cognitive function score was higher(80.55±20.93), that is, the role function of hospitalized patients after lung cancer surgery was relatively poor and the cognitive function was relatively good.Pain symptoms were obvious in the three symptom areas (61.56±28.51); Constipation symptoms were obvious in 6 single items (71.51±37.90).Among the 10 symptom areas of QLQ‑LC13, chest pain was the most prominent symptom(67.04±30.02).The standardized scores of 186 subjects in all fields of the Quality of Life scale are shown in Table 2.
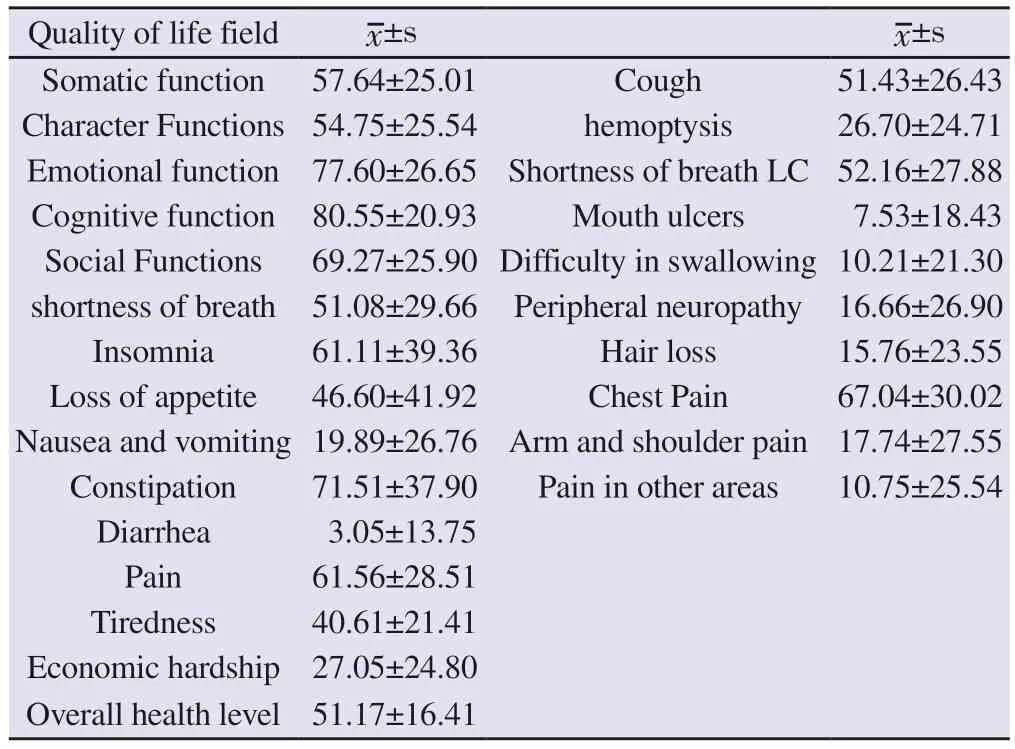
Tab 2 Standardized scores of quality of life in various fields of hospitalized patients after lung cancer surgery
3.3 Multiple linear regression analysis of factors affecting quality of life in patients with lung cancer
With EORTC QLQ‑C30 and lung cancer specific module QLQ‑LC13 scores in various fields as dependent variables, and patients’ demographic characteristics and clinical characteristics as independent variables, multiple linear regression analysis was performed on the influencing factors of the quality of life of patients in hospital after surgery for lung cancer by stepstep regression method, and the influencing factors of scores in each field were analyzed.The assignment method is shown in Table 3.Among them: Gender (X1), age (X2), nationality (X3), rural and urban (X4),number of children (X7), type of medical insurance (X8), knowledge(X10), stage (X11), smoking (X13), second‑hand smoke (X14),drinking (X15), pickled food (X16) and other variables entered into different regression equations respectively (P<0.05), see Table 4 for details.
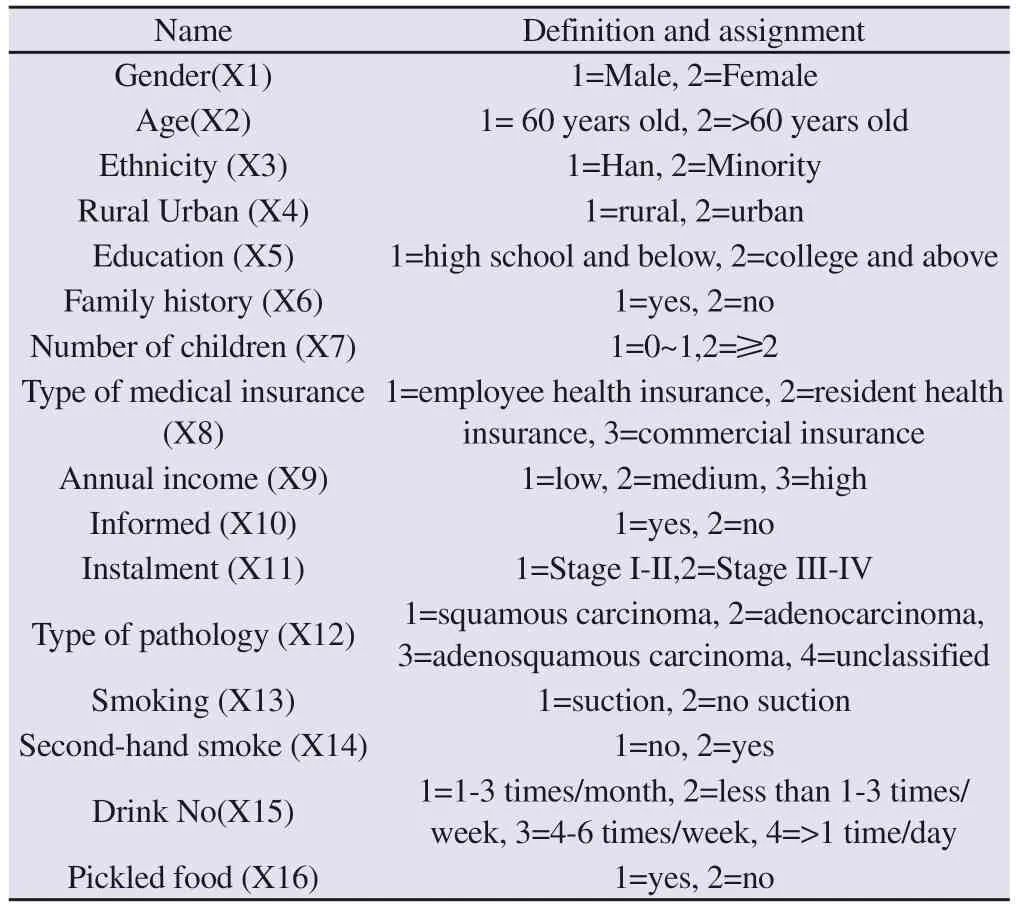
Tab 3 Multiple linear regression analysis variable assignment

Tab 4 Multiple linear regression analysis of factors influencing the quality of life scores of hospitalized patients after lung cancer surgery
4.Discussion
The quality of life of hospitalized patients after lung cancer surgery is affected by a variety of factors.Our study found that older patients(> 60 years old) had low scores in the field of physical function(β=‑0.193), and female patients showed significant symptoms of loss of appetite (β=0.245).Domestic studies on the influence of age on the quality of life have different conclusions: the influence of age on the quality of life has two sides.With the increase of age and the decline of various body functions, the possibility of suffering from various chronic diseases increases, and the score in the field of physical function decreases, and the quality of life evaluation decreases accordingly.However, multiple investigations have found that elderly patients have less care and their mental state is better than that of young patients.Young patients have a heavier daily burden to bear, and their low mental bearing capacity leads to a more serious fear of cancer recurrence, and they are susceptible to negative emotions brought by the disease[10-12].As for the influence of gender on quality of life, we found that women scored low in cognitive function and high in nausea, vomiting and lack of appetite symptoms, indicating that the quality of life of female patients with lung cancer was lower than that of male patients.This conclusion is consistent with the views of Sun Hao[13] et al.
A number of domestic studies have found that ethnicity is related to quality of life.Wang Zongyan found that the life quality of the Han nationality was lower than that of the Naxi nationality[14], and the ethnic distribution in Hainan Province was mainly dominated by the Han nationality and Li nationality.Xu Weiling[15] found that the life quality of other ethnic groups was worse than that of the Li nationality, and that of the Li nationality was worse than that of the Han nationality.The nationalities of Hainan people investigated in this study are mainly Han, Li and Miao.We found that the function field scores of Han nationality were lower than those of other ethnic minorities (β=0.179), the fatigue symptoms of Han nationality were heavier (β=‑0.162), and the general health level of ethnic minorities was higher (β=0.166), suggesting that the quality of life of hospitalized patients after lung cancer surgery of Han nationality was lower than that of ethnic minorities.
Malignant tumor not only damages patients’ physical and mental health due to the disease itself and the side effects produced in the treatment process, but also brings heavy economic burden to patients’families due to the economic pressure generated in the diagnosis and treatment process[16-17].Our analysis found that patients with employee health insurance had lower emotional function scores(β=0.194), lower cognitive function scores (β=0.281), lowest scores in the field of social function (β=0.188), more symptoms of pain in other areas (β=‑0.227), and lower quality of life.Liu Min[18] analyzed the quality of life of 102 patients with colorectal cancer who underwent surgical treatment, and found that the quality of life of patients with new rural cooperative medical insurance was lower than that of patients with urban employee medical insurance and urban resident medical insurance.Guo Lei[19] found that urban residents had a higher overall health level and a higher evaluation of life quality than rural residents.But the health inequities of urban residents are much different from those of rural residents.We also found that symptoms of appetite loss (β=0.192) and peripheral neuropathy were more pronounced in urban lung cancer patients(β=0.174).
We also found that symptoms of appetite loss (β=0.192) and peripheral neuropathy were more pronounced in urban lung cancer patients (β=0.174).This study found that patients exposed to secondhand smoke pollution had lower cognitive function scores(β=‑0.158) and significant symptoms of oral ulcers (β=0.185),suggesting that the quality of life of hospitalized patients exposed to secondhand smoke after lung cancer surgery was low.The symptoms of arm and shoulder pain in smoking patients were more severe (β=‑0.21) and cough symptoms were less severe (β=0.175) than those in non‑smoking patients, which may be related to the fact that patients with mild cough symptoms were more inclined not to change their smoking behavior.Patients who drank alcohol frequently (drinking frequency > 1 time/day) had severe cough symptoms (β=0.27).A number of foreign studies have shown that quitting smoking behavior has a profound impact on the long‑term prognosis of hospitalized patients after lung cancer surgery: the longer the duration of quitting smoking, the lower the risk of postoperative complications[20].Quitting smoking after diagnosis can reduce the risk of cancer recurrence in lung cancer patients and improve the level of various functional areas and quality of life of patients[21].Previous studies have shown that smoking is closely related to the occurrence and development of lung cancer, but a recent study believes that smoking is not a decisive factor in the incidence of lung cancer, because there are large differences between individuals in the ability to metabolize carcinogens (such as nicotine) produced by smoking, and these differences will affect the incidence of lung cancer[22].Studies have found that the survival rate of non‑smoking lung cancer patients exposed to household second‑hand smoke is lower than that of non‑exposed similar patients, and the risk of death of non‑smoking lung cancer patients exposed to household second‑hand smoke is 1.83 times higher than that of similar patients without household second‑hand smoke exposure.Spousal and parental smoking is the main source of secondhand smoke exposure.The presence or absence of tobacco smoke in the home environment is one of the factors affecting the prognosis of lung cancer.When patients’ exposure to second‑hand smoke is reduced, the impact of lung cancer prognosis in non‑smoking patients is directly proportional to the time and intensity of tobacco smoke exposure before[23-24].A foreign study found that patients with high nicotine dependence had significantly lower scores in functional areas and total health status, and smoking would increase the risk of chest pain[25].Bai Feng[26] found in the follow‑up of colon cancer patients that the quality of life of smoking patients was low: smoking patients had low scores in emotional function and social function, and high scores in fatigue, nausea,vomiting, diarrhea symptoms and economic difficulties.
At present, there are few studies on the impact of the number of children on the quality of life of lung cancer patients.A study in Shanghai found that lung cancer patients with only one child had high scores in fatigue, loss of appetite, diarrhea and other fields, with heavy symptoms and low quality of life[27].In this study, we found that patients with fewer children (0~1) had less cough symptoms(β=0.178), which may be related to the low economic pressure of single child patients.We found that patients without knowledge of the disease had significant symptoms of arm and shoulder pain(β=0.151).Qi Luyan[28] believed that concealing the condition would lead to anxiety and depression in lung cancer patients and affect their quality of life, while diagnosis notification could help lung cancer patients regulate their emotions, form positive disease perception, and improve their quality of life.We found that patients with early pathological stages (stage I to II) had severe symptoms of shortness of breath (β=‑0.159) and pain (β=‑0.181), the reasons for which need to be further studied.At the same time, we also found that patients who often ate pickled food had severe pain symptoms(β=‑0.219), and pain symptoms in other parts (β=‑0.149) were obvious.
5.Conclusion
Through this investigation, we believe that medical staff can carry out individualized diagnosis and treatment for patients in the treatment process, provide positive emotional guidance for patients,pay attention to patients’ physical and mental health, set up patient clubs for patients to enhance communication between patients,organize support activities between patients, guide patients’ families to increase communication and support with patients, and actively participate in social activities.And help patients with psychological problems, such as guidance.The importance and benefits of quitting smoking and drinking should be emphasized, and patients should be encouraged to quit smoking and reduce consumption of preserved food in order to improve the quality of life and long‑term prognosis of hospitalized patients after lung cancer surgery.
杂志排行

Journal of Hainan Medical College的其它文章
- Mechanism of FXR alleviating the liver fibrosis by regulating perilipin 5
- Study on the mechanism of effect of Daodi Tongguan Decoction on rats with premature ovarian failure
- Correlation between Nrf2‑GPX4 signaling pathway and patients with coronary heart disease
- Establishment and validation of a nomogram for predicting the risk of liver inflammation in chronic HBV infection
- Clinical study of different modes of repetitive transcranial magnetic stimulation in the treatment of post‑stroke executive dysfunction
- Meta-analysis of the efficacy and safety of extended right liver transplantation versus whole liver transplantation