Radiation dose analysis of computed tomography coronary angiography in Children with Kawasaki disease
2023-11-16MaheshChandraBhattManphoolSinghalRakeshKumarPilaniaSubhashChandBansalNiranjanKhandelwalPankajGuptaSurjitSingh
Mahesh Chandra Bhatt, Manphool Singhal, Rakesh Kumar Pilania, Subhash Chand Bansal, Niranjan Khandelwal, Pankaj Gupta, Surjit Singh
Abstract
Key Words: Computed tomography coronary angiography; Coronary artery abnormalities; Dual source computed tomography;Kawasaki disease; Radiation exposure
INTRODUCTION
Kawasaki disease (KD) is a common childhood medium vessel vasculitis with special propensity for coronary arteries.It typically affects children below 5, however, older children and young adults can also be affected.Diagnosis of KD is based on constellation of clinical features, and there are no pathognomonic laboratory tests.Children with KD fluffing the epidemiological case definition are known as complete KD.Incomplete and atypical forms of disease can constitute up to 50% of patients with KD[1-4].Coronary artery abnormalities (CAAs) represent the major contributors to both acute as well as long term morbidity and mortality related to KD[4-8].Timely treatment of KD reduces the CAAs incidence from 25% to < 5%.Timely and precise evaluation of CAAs is important for management of patients with KD[4].2D-echocardiography (ECHO) has hitherto been the first line imaging modality for evaluation of CAAs.However, it has some inherent limitations.These include operator dependency, poor acoustic window and lack of visualization of middle and distal segments of coronary arteries[6].Further, it is difficult to visualize the coronaries in older children who have thick chest walls[9,10].Catheter angiography (CA) is the gold standard imaging modality but has the disadvantages of being invasive and is associated with high radiation exposure[11-13].
Recently, multi-detector CT (MDCT) and dual source CT (DSCT) platforms have allowed imaging of coronary arteries at any heart rate with attempts at radiation optimization[14-18], which otherwise is a serious concern in children[19,20].There are limited studies that to with small sample size on radiation dose in children with KD undergoing CTCA on DSCT (Table 1).Radiation dose in these studies was either more or comparable to our study.This study enumerates various methods to optimize the radiation exposure on CTCA in children with KD, an audit of the radiation dose and show that radiation exposure can be reduced to 1mSv or less in majority of children.
MATERIALS AND METHODS
Study design
Review of records was carried out during the period December 2013-February 2018.The manuscript has been approved by Departmental Publication Review Board (RDG/EC/Pub/27 dated July 03, 2020).Written informed consent was obtained from parents prior to CTCA.
Patient population
Children with KD who underwent CTCA were either at presentation or on regular follow-up with CAAs on ECHO were included in the analysis.As per International Commission on Radiological Protection-103 (ICRP 103) recommendations,children were grouped as per age into infants (< 1 year), 1-5 years, 5-10 years, > 10 years.System generated radiation exposure dose length product (DLP in milligray-centimeters-mGy.cm) was recorded and effective radiation dose (millisieverts-mSv) was calculated by applying age adjusted conversion factors recommended by ICRP 103[21] and analysis ofradiation exposure across groups was done (Table 2).
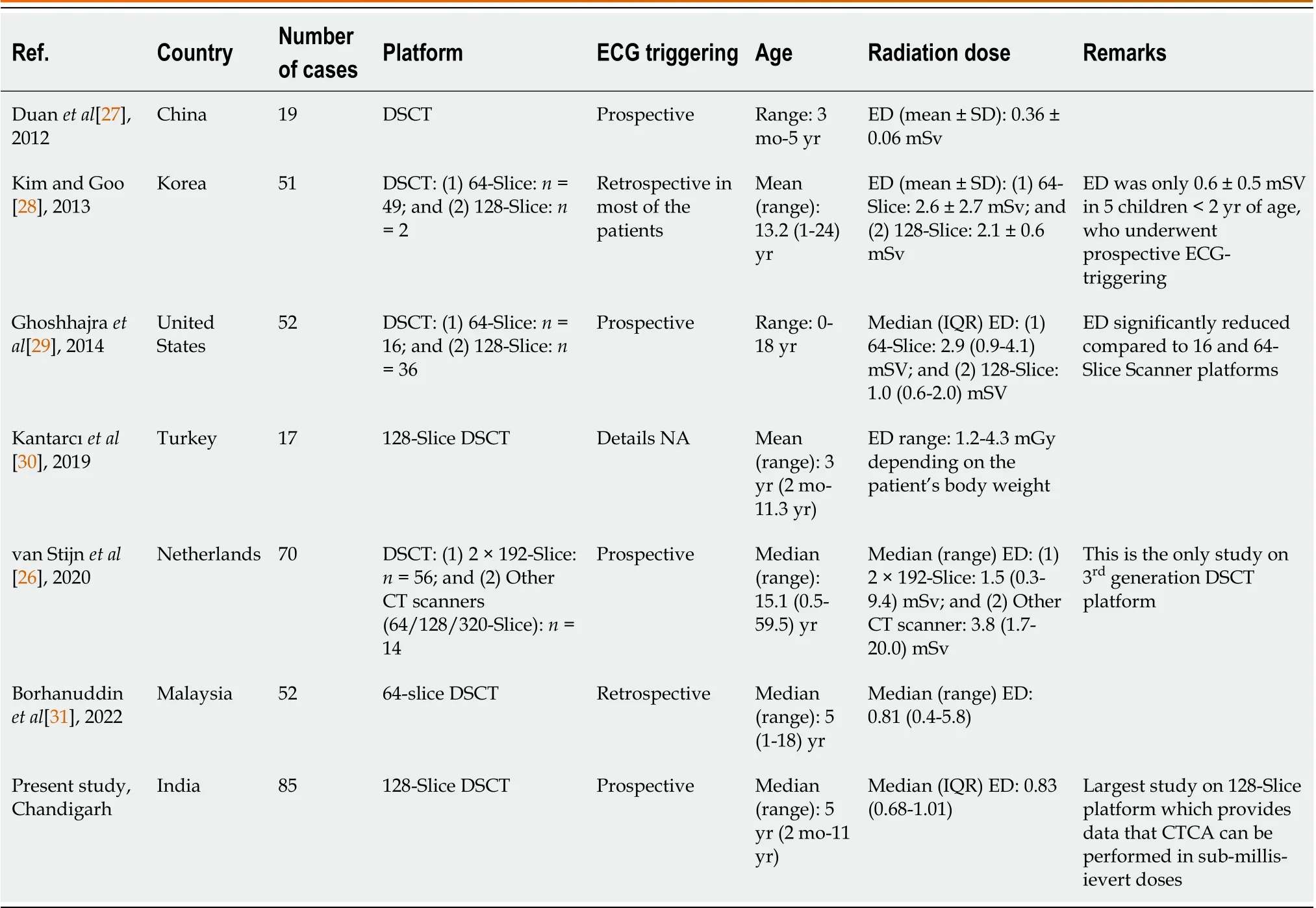
Table 1 Comparison of effective radiation dose on dual source computed tomography coronary angiography platforms in patients with Kawasaki disease
CTCA technique
CTCA was carried out on a second generation DSCT 128-slice scanner (Somatom Definition Flash, Siemens, Erlangen,Germany) using non-ionic contrast (Omnipaque 350, GE Healthcare, Ireland) with the following parameters: Temporal resolution- 75 milliseconds, gantry rotation time-0.28 s, slice thickness-0.6 mm.The scan was conducted in a craniocaudal direction from floor of carina to the diaphragm (till base of heart).CTCA was carried out with adaptive prospective electrocardiography (ECG) triggered sequence (CorAdSeq) tube current modulation to minimize radiation exposures without compromising image quality.With this technique the CT X-ray tube is switched on at the predefined range of RR interval of ECG (in our study 30%-80% R-R interval) and provides images in systolic and diastolic phases.
Scanning parameters were customized to ensure minimal radiation exposure.Volume CT dose index (CTDIvol) was taken as adjusted by the CT scanner according to body-size adapted protocols-CARE Dose4D (Siemens, Erlangen,Germany).With this tube current-time product (mA.s) is automatically calculated for optimal automatic exposure depending on body weight and cross-sectional area.Automatic CARE kV was switched off and adjusted to 80 kilovolt(kVp) in all children.These modifications, along with CARE-Dose 4D tube current modulation, enabled us to further reduce the effective radiation dose.Lowest kVp and mAs values ensured optimal image quality with minimum possible radiation exposure.The current-time product ranged between 32-154 mA.s.
Statistical analysis
Parameters showing normal distribution were depicted as mean and standard deviation, while variables with skewed distribution were expressed as median and interquartile ranges (IQR).APvalue of < 0.05 was regarded as significant.Statistical analysis was accomplished using SPSS statistical software version 20.0 (SPSS Inc., Chicago, IL, United States).
RESULTS
Demographic characteristics
CTCA of 85 patients [71 (84%) boys; 14 (16%) girls] with KD were acquired.Median age of our cohort was 5 years [IQR: 5(7, 2)]; range: 2 mo-11 years.As per ICRP 103 recommendations, children were grouped as per age into infants (< 1 year)(n-10; 12%), 1-5 years (n-29; 34%), 5-10 years (n-38; 45%), > 10 years (n-8; 9%).
Radiation dose
The median DLP and effective dose of all 85 patients in our study were 21.0 mGy.cm, IQR = 15 (13, 28) and 0.83 mSv, IQR= 0.33(0.68, 1.01), respectively.Details of DLP and effective CT radiation dose for children in study group are given in Table 3.
The mean DLP in infants, 1-5 years, 5-10 years, and > 10 years was 9.19, 18.82, 31.76, and 55.67 mGy.cm, respectively.The mean effective dose in infants, 1-5 years, 5-10 years, and > 10 years was 0.63, 0.83, 1.04, and 1.38 mSv.The DLP showed significant increase with increasing age.The difference in the DLP was statistically significant across all age groups (Pvalue for infantsvs1-5 years, 1-5 yearsvs5-10 years, and 5-10 years > 10 years; < 0.001, < 0.001, and 0.01,respectively.The mean effective dose in infants (0.63 mSv) was significantly lower than the other age groups (1-5 years 0.85 mSv, 5-10 years 1.04 mSv, and > 10 years 1.38 mSv) (P< 0.05).There was no significant difference in the effective dose among children in the other groups.
All the CTCA studies were of diagnostic quality.No child required a repeat examination.
DISCUSSION
We performed CTCA on 128-DSCT scanner with radiation optimized protocols (CorAdSeq tube current modulation,body-size adapted protocols and reduced tube kilovoltage settings at 80 kVp) to minimize radiation exposures.In total 85 children with median age of 5 years [IQR: 5 (7, 2)]; (range: 2 mo-11years) were scanned.The mean effective radiation dose was 0.83 mSv with radiation exposure significantly lower in infants (0.63 mSv) as compared to other age groups.CTCA can visualize CAAs along the entire course of coronary arteries[6].
KD is a medium vessels vasculitis with special predilection for involvement of coronary arteries[1-4].ECHO has hitherto been considered the imaging modality of choice for diagnosis and follow-up of CAAs in patients with KD, but with many limitations related to comprehensive evaluation of coronary arteries.CA is the gold standard, but is associated with inordinate radiation exposure, is invasive and cannot be repeated often for follow-up.Moreover, mural abnormalities cannot be depicted on CA[9,22].
With the advent of new high MDCT and DSCT scanners, imaging of coronary arteries is possible.However, until recently the risk of high radiation exposure had precluded the use of CTCA in children with KD.This was probably the limiting factor that prevented its application in pediatrics when cardiac CT on single source 64-slice was made possible.CTCA with single source 64-Slice CT is associated with radiation exposure as high as 3.0-5.7 mSv[23].Moreover, this technique resulted in sub-optimal image quality due to inability to acquire images at high heart rates in children.Though there are no criteria to define limits of radiation dose in children, authors are of the opinion that this is clearly unacceptable in children and every possible method should be used to reduce radiation exposure in children as per ALARA (as low as reasonably achievable) principle[24].Higher slice and dual source CT scanners with improvised technologies have emerged as promising platforms for CTCA with possibility for radiation optimization providing a promising imaging modality for assessment of CAAs of KD vis-a-vis CA.
Various dose-saving strategies that can be adopted during CTCA on DSCT are body size-adapted protocols including low tube voltage techniques, ECG-controlled and attenuation-based tube current modulations, and prospectively ECGtriggered scanning[14-18].Lowering the KVp values (to 80) results in a significant dose reduction with acceptable image quality[25].We have used adaptive prospective ECG-triggered sequence with tube current modulation, lower tube voltage (80 kVp) and optimized system calculated tube current using CARE-Dose 4D for radiation reduction.Iterative reconstruction algorithm that was used in our protocol in addition provides excellent quality images even at low exposure.
van Stijnet al[26] recently published a study on coronary artery assessment in patients with KD using 3rdgeneration DSCT platform (2 × 192-Slice CT scanner) on 70 children.The authors achieved a radiation exposure of 1.5 mSv (range 0.3-9.4 mSv)[26].The radiation dose in our cohort was lower.Median effective dose of radiation 0.83 mSv (0.68-1.01) in our study is amongst the lowest achieved so far on DSCT platform using 128-Slice CT scanner.Further, cohort sizes in the previously published studies have been much smaller than ours[26-31] (Table 1).Having achieved such low radiation exposures and given the fidelity of images acquired on these platforms, it may not be long before CTCA on a DSCT platform becomes the imaging modality of choice for detailed evaluation of CAAs in children with KD.

Table 3 Effective computed tomography radiation exposure according to age in adaptive prospective electrocardiography-triggered sequence computed tomography coronary angiography on 128-dual source computed tomography platform
We recognize several limitations to our study.The data in the current study comes from a single center and more such studies are required for further validation of our results.Further, there were fewer children in individual age groups.The cumulative impact of radiation dose in children who may require follow up CTCA is not known.Though, all the scans were of diagnostic quality, it is desirable to assess image quality along with radiation dose.However, our study was not tailored to assess the image quality.
CONCLUSION
In conclusion, DSCT scanners by virtue of high temporal resolution, faster gantry rotation, ECG triggered tube current modulation, large field of view, body adaptive automatic selection of tube current modulation and iterative reconstruction algorithm have largely addressed the issue of high radiation exposure when subjecting children with KD to CTCA.It is now possible to evaluate these patients using submilliseivert radiation exposure.This is a significant advance in management of KD.
ARTICLE HIGHLIGHTS
FOOTNOTES
Author contributions:Bhatt MC and Singhal M contributed to the data interpretation, writing of first draft, review of literature, editing of manuscript and critical revision of manuscript at all stages; Pilania RK contributed to the patient management, data interpretation,writing of first draft, review of literature, editing of manuscript and critical revision of manuscript at all stages; Bansal SC, Khandelwal N, and Gupta P contributed to the review of literature and editing of manuscript; Singh S contributed to the patient management, review of literature, editing of manuscript, critical revision of manuscript at all stages; Bhatt MC and Singhal M contributed equally; Singhal M finally approved the manuscript.
Institutional review board statement:The manuscript has been approved by Departmental Publication Review Board (RDG/EC/Pub/27 dated July 03, 2020), No.NK/1837/Res/2890.
Informed consent statement:All study participants or their legal guardian provided informed written consent about personal and
medical data collection prior to study enrolment.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:The author(s) declare(s) that they had full access to all of the data in this study and the author(s) take(s)complete responsibility for the integrity of the data and the accuracy of the data analysis.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:India
ORCID number:Manphool Singhal 0000-0002-1311-7203; Rakesh Kumar Pilania 0000-0002-9015-1704; Niranjan Khandelwal 0000-0002-8326-5164; Pankaj Gupta 0000-0003-3914-3757; Surjit Singh 0000-0002-8738-4582.
S-Editor:Fan JR
L-Editor:A
P-Editor:Yuan YY
杂志排行

World Journal of Clinical Pediatrics的其它文章
- Transient hyperphosphatasemia in a toddler with COVID-19 infection: A case report and literature review
- Safety and efficacy of intravitreal anti vascular endothelial growth factor for severe posterior retinopathy of prematurity with flat fibrovascular proliferation
- Accidental ingestion of foreign bodies/harmful materials in children from Bahrain: A retrospective cohort study
- Gastrointestinal and nutritional care in pediatric neuromuscular disorders
- Role of gastrointestinal health in managing children with autism spectrum disorder
- Use of endolumenal functional lumen imaging probe in investigating paediatric gastrointestinal motility disorders