Accidental ingestion of foreign bodies/harmful materials in children from Bahrain: A retrospective cohort study
2023-11-16HasanIsaShaikhaAldoseriAyshaAbduljabbarKhaledAlsulaiti
Hasan M Isa, Shaikha A Aldoseri, Aysha S Abduljabbar, Khaled A Alsulaiti
Abstract
Key Words: Pediatric; Accidental ingestion; Foreign body; Caustic; Complication; Bahrain
INTRODUCTION
Children like to discover their environment by putting substances into their mouth[1].Accidental ingestion of foreign bodies (FBs) or caustic materials is a common problem encountered by families with children.It is considered as one of the most common indications for emergency referral and hospital admission.There are diverse types of FBs or ingested materials that can be swallowed by children.Coins, toy parts, jewelry, button-type batteries, needles, and pins are the most frequently ingested materials[1].
Most ingested FBs pass spontaneously, and patients can be safely observed[2].Although most ingestion incidents are insignificant in terms of consequences, a few can pose a challenging problem that may lead to serious life-threatening complications[2].For example, numerous magnetic objects located at various sites in the bowel can attract one another,leading to pressure necrosis of the bowel wall and eventual perforation[1].Furthermore, although batteries can pass easily through the digestive tract and are eliminated from the stool within a few days of ingestion, swallowing batteries is more dangerous than swallowing coins or other inert objects because of their electrochemical composition and high risk of local damage[3].Moreover, batteries 20 mm or larger in size can affect the esophagus, especially in young children[3].Strong exothermic reactions can lead to serious mucosal injuries that may appear as skin burns[3].Caustic ingestion is also common in pediatric age groups, and most cases happen accidentally[4].The seriousness of this ingestion is due to the tissue injury and necrosis[4].Tissue damage can start from the mucosa and extend to the muscular layers, causing multiple complications, such as burns, strictures, and perforations[4].
Prompt diagnosis of accidental ingestion, appropriate management, and a decision on whether the patient necessitates intervention are crucial for reducing morbidity[2].The type of FB, anatomic location in which the FB is lodged, and clinical picture of the patient determine the timing of endoscopic removal of the swallowed FB[2,3].In children with caustic ingestion, postoperative treatment remains controversial and includes entities such as antireflux therapy,antibiotic therapy, steroids, and interventions such as esophageal stenting[3].Nonetheless, the implementation of preventive methods and safe storage of caustic materials is essential to avoid these accidents and their related consequences[4].
Although many studies on accidental ingestion in children have been published in several countries, no studies have been published on this issue in Bahrain.The aim of this study was to review the incidence, demographics, different types of FBs/harmful materials, diagnostic modalities, complications, and outcomes of accidental ingestion in a pediatric age group and compare patients with endoscopic or surgical complications with those without complications to identify the predicted risk factors.
MATERIALS AND METHODS
Study design, setting, and population
In this retrospective cohort study, all pediatric patients (aged < 18 years) who presented to the Department of Accident and Emergency with a history of accidental ingestion and were admitted to the Department of Pediatrics, Salmaniya Medical Complex, Bahrain from January, 2011 to August, 2021 were included.Patients who presented to the Department of Accident and Emergency and were subsequently discharged were excluded.
Data collection
Patient data were collected by reviewing electronic and paper-based medical records.Important missing data were retrieved through direct contact with the patients’ parents or guardiansviatelephone.Demographic data, including year of admission, nationality, sex, age at presentation, and age at the time of the study, were collected.Data on families’socioeconomic status (SES) were collected, including paternal and maternal educational levels, occupation, number of children, and total family income.Accordingly, families were categorized into low-, middle-, and high-SES groups.Data on symptoms at presentation, including vomiting, abdominal pain, passing tarry stool, choking, dysphagia, drooling of saliva, shortness of breath, and coughing, were collected.Details related to accidental ingestion of FBs, including the type,number, and source of FBs, were collected.Additionally, the presence of witnesses at the time of accidental ingestion,time to presentation to the Department of Accident and Emergency, and spontaneous passage times were outlined.More details regarding the type of battery were collected from the patients who ingested batteries.
Radiological imaging findings, endoscopic findings, and extraction methods were also reviewed.Urgent endoscopy was considered if it was performed within 48 h of ingestion, whereas a longer time was considered a delayed endoscopy.Data on the patients’ hospital management, including endoscopic removal and the use of medications, such as lactulose,enema, glycerin suppositories, and omeprazole, were gathered.Furthermore, data on patient outcomes, including length of stay, morbidity, mortality, and follow-up period, were assessed.
Statistical analysis
Patient data were initially collected and entered into an Excel sheet and then transferred to and analyzed using the Statistical Package for the Social Sciences Statistics ver.21.0 (IBM Corp., Armonk, NY, United States).Categorical variables are presented as numbers and percentages.Continuous variables are presented as the mean and standard deviation or median and interquartile range (IQR), according to distribution normality using the Shapiro-Wilk test.To assess the trend of accidental ingestion episodes over the last 10-year period, the duration was divided into two periods of 5 years each (2012-2016 and 2017-2021), and the incidence of ingestion in both periods was compared.The incidence was calculated as the number of patients with accidental ingestion per year divided by the total pediatric population (less than 18 years), obtained from the Bahrain Health Statistics website (https://www.moh.gov.bh/Ministry/Statistics?lang=en).The patients were divided into three groups based on the type of ingested material (FBs, caustic chemicals, and medications).The three groups were compared based on patient demographics, family SES, clinical presentations,ingestion scenario, endoscopic and surgical complications, management, and outcomes.Based on radiological and endoscopic findings, the anatomical location of the FB was categorized into esophageal, stomach, and bowel locations and compared with regard to the presenting symptoms.Metallic FBs were divided into jewelry and other metal objects and compared based on sex.The Fisher’s exact test or Pearson’s chi-square test was used to compare categorical variables,while student’sttest, Mann-WhitneyUtest, or Kruskal-Wallis’s test was used to compare independent groups.Confidence interval (CI) was set to 95%.P< 0.05 was considered statistically significant.
Ethical approval
This study was conducted in accordance with the principles of the Declaration of Helsinki, and it was ethically approved by the Secondary Health Care Research Committee, Salmaniya Medical Complex, Government Hospitals, Kingdom of Bahrain (IRB number: 88300719, July 30, 2019).
RESULTS
During the study period, 161 accidental ingestion episodes were documented in 153 children admitted to the hospital, all of whom were included in this study.Eight (5.0%) patients had another episode of accidental ingestion following the initial episode; one of them had three episodes in total, and two patients ingested the same object (battery or hard food)during the two episodes.Of the eight patients with multiple ingestions, three (37.5%) had neuropsychiatric disorders,including autism, demyelination, and mild intellectual disability.The latter had iron-deficiency anemia associated with pica.The patient with three episodes had disc battery ingestion, followed by two repeated FB ingestions, and was referred to the child protection team because of suspected child neglect, as this patient also had repeated burn events.
The mean number of accidental ingestions was 13.9 ± 10.3 episodes per year.The annual incidence of accidental ingestion episodes is shown in Figure 1.The incidence of accidental ingestion increased during the study period.In 2012-2016, the mean incidence was 3.3 ± 2.8 compared to 4.2 ± 2.4 episodes in 2017-2021.However, this increase was not statistically significant (P= 0.610, 95%CI: -4.6 to 2.9).
The demographic data and clinical presentations are shown in Table 1.Most of the patients ingested FBs (n= 108,70.6%), 31 (20.3%) ingested caustic chemicals, and the remaining 14 (9.2%) ingested medications.Most of the patients were boys (n= 85, 55.6%).Most patients were Bahraini children (n= 118, 77.1%), while non-Bahraini children accounted for 35 (22.9%) patients (10 from India, 5 from Saudi Arabia, 2 from Bangladesh and United States of America each, 1 from Egypt, Sri Lanka, Sudan, Yemen, and Syria each, while 8 patients had unspecified nationalities).The median age at presentation was 2.8 (IQR: 1.8-4.4) years, and the most frequent age group was 2-3 years old, accounting for 43.5%.Patients with caustic ingestion were younger than those who ingested medications or FBs at the time of presentation (P<0.001).Most patients (n= 119, 77.8%) ingested one item, and most were symptomatic (n= 86, 57.3%).The most common symptom was vomiting (n= 44, 29.3%), followed by abdominal pain (n= 25, 16.7%).Patients with caustic ingestion (n=26/31, 89.7%) were more symptomatic than those who ingested medications (n= 8/14, 57.1%) or FBs (n= 52/108, 48.6%) (P< 0.001).The caustic group had more vomiting (P< 0.001) and coughing (P= 0.029) than the other two groups.Most of patients with FB ingestion were asymptomatic (n= 55/108, 51.4%).Upon comparison of symptoms according to the location of FBs (esophagus, stomach, or bowel), most of the 16 patients with esophageal FBs were found to be symptomatic [14 (87.5%)vs2 (12.5%)], while the majority of the 56 patients with gastric FBs [34 (60.7%)vs22 (39.3%)] and the 32 patients with intestinal FBs [19 (59.4%)vs13 (40.6%)] were asymptomatic (P= 0.002).
Five patients had underlying diseases that might have been related to accidental ingestion.Esophageal strictures after tracheoesophageal fistula repair were found in two patients with food bolus impaction; one patient had cerebral palsy with needle ingestion, one had mental retardation with coin ingestion, and one had autism with disc battery ingestion.
Out of 136 (88.9%) patients with available witness history, 58 (43.6%) were witnessed and 78 (57.4%) were unwitnessed.Of those witnessed, 55 (94.8%) patients had a known witness person, while 3 (5.2%) had an unknown witness.Three(5.2%) patients had more than one witness person.First degree relatives were witnesses in 47 (85.5%) patients, second degree relatives in 8 (14.6%), and unrelated people (teacher, housemaid, and family friend) in 3 (5.5%).The mother was the most frequent witness (n= 27, 49.1%), followed by other siblings [n= 11 (20%); seven of them were sisters and four were brothers] and fathers (n= 7, 12.7%).
There were no significant differences among the three groups with respect to sex, nationality, SES, maternal occupation, number of siblings, time to presentation, length of stay, number of ingested materials, or the presence of a witness.
The different types of ingested material are listed in Table 2.Battery ingestion was the most frequent FB type (n= 49,32%); 48 of them were disc batteries, and 1 was a finger type.The sharp objects included earring, screw, and nail/nail hanger (n= 5 each), key/keyring/keychain (n= 4), needle (n= 3), hair clip/pin and sharp pin (n= 2 each), gold chain, leg accessories, necklace, pepsi cap, and zipper piece (n= 1 each).The chemicals and corrosive solutions included alkaline corrosives (n= 19; Clorox in 11 patients, detergents or disinfectants in 3 each, and nonspecific corrosives in 2 patients),acid corrosives (n= 5; keratolytic agents in three and toilet cleaners in two patients), and other chemicals (n= 6).The medications included paracetamol (n= 4), antihypertensives (n= 3, coversyl in two and angiotensin-converting enzyme inhibitor in one patient), antihistamines, hypoglycemic agents, oral contraceptives, nitrite, multivitamins, methylphenidate, and multiple medications (n= 1 each).
Even though there was no significant difference between boys and girls in terms of the type of FBs ingested (P= 0.217),in metal object ingestions, girls were found to ingest more jewelry items than boys, with seven (70%)vsthree (30%),respectively (P= 0.006).Of the 49 (32%) patients who ingested batteries, 43 (87.8%) patients had the source of battery data available.Unsafe toys were the main sources of batteries (n= 22, 51.2%), followed by light torches (n= 10, 23.3%), remotecontrol devices (n= 2, 4.7%), artificial candles, baskets, electronic walking aids, headphones, laser pens, on car seats, on tables, and from watches and weighing scales (n= 1 each, 2.3%).
The accidental ingestion scenarios are presented in Table 3.Data regarding this scenario were available for 131 (85.6%)patients.Accidental ingestion mostly happened while the child was playing (n= 53, 40.5%).FBs were ingested more while playing (P< 0.001), caustic chemical ingestion was mainly due to unsafe storage (P< 0.001), and medication ingestion was mostly due to a missing object (P< 0.001).
Results of radiological imaging, including chest and abdominal radiography, were available for 123 (80.4%) patients:108 (100%) for FB, 8 (25.8%) for caustic, and 7 (50%) for medication ingestion (P< 0.001) (Table 4).The remaining 30(24.6%) patients with no radiological findings ingested either corrosives (n= 23, 76.7%) or medications (n= 7, 23.3%).The most common location of the ingested object was the stomach both radiologically (n= 54/123, 43.9%) and endoscopically(n= 31/91, 34%).

Table 1 Demographic data and clinical presentation of 153 children with accidental ingestion

aPearson’s χ2 test was used for categorical variables.bKruskal-Wallis’s test was used for continuous variables.1Patients might have more than one symptom.2Dizziness, chest pain, nausea, tarry stool, and throat discomfort, each in two patients; fever, fatigue, nose swelling, tongue and lips swelling, abdominal bloating, noisy breathing, cyanosis, drowsiness (chlorpheniramine ingestion), reduction in activity, and lip ulcer, each in one patient (two patients of them had two symptoms).Boldface indicates a statistically significant difference with P < 0.05.Values are presented as number (%) or median (interquartile range).FB: Foreign body.

Table 2 Types of foreign bodies and harmful materials accidentally ingested by 153 children
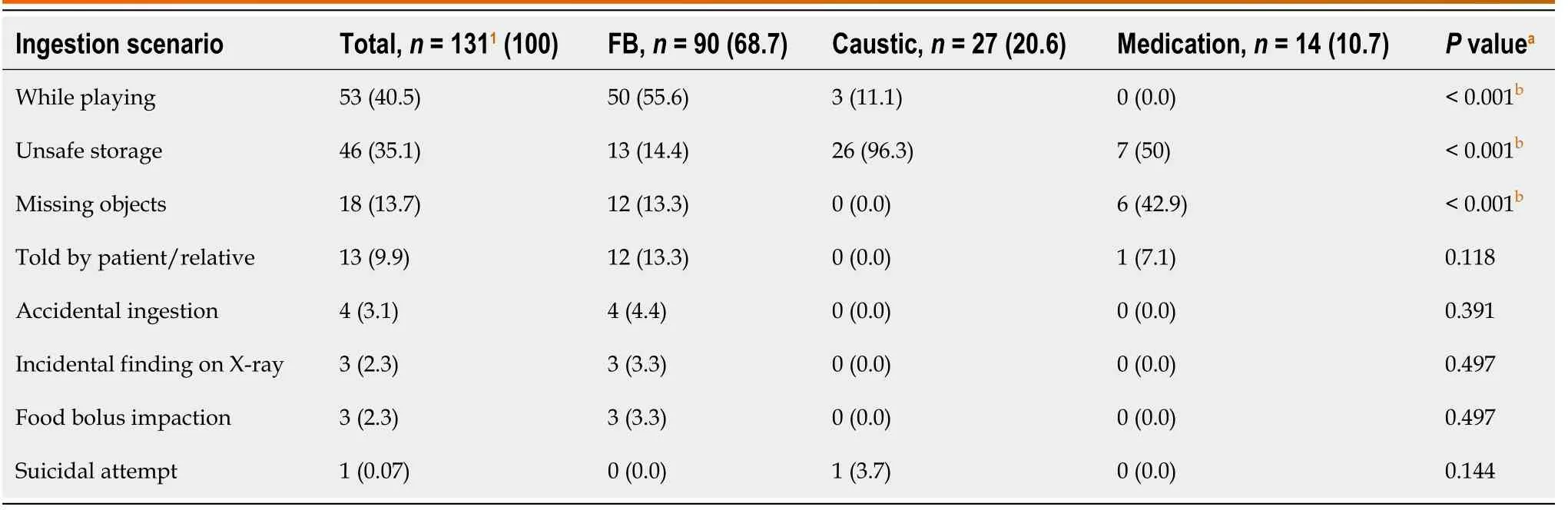
Table 3 Scenario of foreign body/material ingestion in children (n = 131)

Table 4 Anatomical locations of ingested foreign bodies based on radiological and endoscopic findings
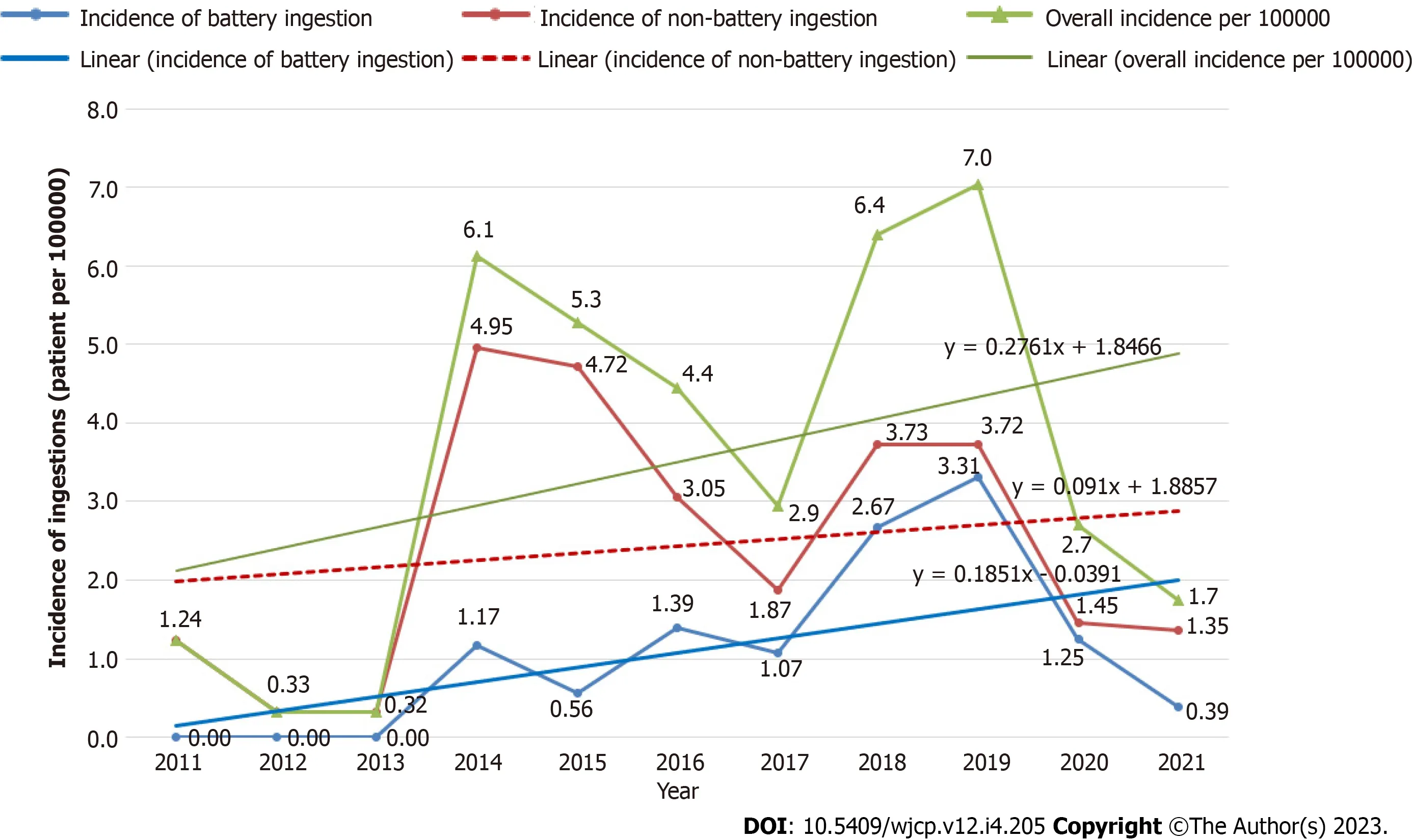
Figure 1 Incidence of accidental ingestion episodes among children admitted to Salmaniya Medical Complex, Bahrain in 2011-2021.
Endoscopic procedures were performed in 91 (59.9%) of the 152 (99.4%) patients: 73/107 (68.2%) for FB ingestion, 18/31 (58.1%) for caustic ingestion, while no patient with medication ingestion underwent endoscopy (P< 0.001) (Table 4).Ninety patients (59.2%) underwent upper gastrointestinal endoscopy and one (0.7%) underwent colonoscopy.The common endoscopic location of the ingested objects was also the stomach (n= 31, 34%).The time from presentation to endoscopy was available for 81 (89%) patients; 78 (96.3%) of them had an emergency endoscopy (< 48 h), while 3 (3.7%)were delayed after 48 h.The first delayed patient was a 4-year-old girl who was brought by her parents with a history of fainting and vomiting streaks of blood after accidental ingestion of Clorox stored in a small water bottle.The second patient was an 8-year-old boy who ingested two attached magnets while playing a game.X-ray imaging revealed that the magnets had passed down to the large intestine.He was administered laxatives for 2 d without any progress; therefore,the magnets were removed endoscopically.The third patient was a 7-year-old boy who ingested a coin while playing,which was found to be in the stomach radiologically and remained there for 3 mo.
Data about the method of extraction were available in 107/152 (70.4%) patients with FB ingestion; spontaneous passage was noted in 54 (35.5%), endoscopic removal in 46 (30.3%), laparotomy in 5 (3.3%) (all after magnets ingestion), and direct laryngoscopy in 2 (1.3%); while in the remaining 45 (29.6%) patients nothing was removed as they ingested chemicals (n=31, 20.4%) or medications (n= 14, 9.2%).Among patients who passed the FB spontaneously, 34 (59.7%) passed it within the first 24 h of admission, 13 (22.8%) passed it between 1 and 2 d, 10 (17.5%) passed it after 3 d, and one patient had missing data.Three patients underwent endoscopic removal of one FB and spontaneous passage of the other.
Pharmacological therapy was required for 105/148 (70.9%) patients; 79/105 (75.2%) in the FB group, 22/29 (75.9%) in the caustic group, and 4/14 (28.8%) in the medication group (P= 0.001).The commonest medication was omeprazole (n=58; 37.9%), which was used more in the caustic group (n= 19/28, 67.9%) than in the FB (n= 37/104, 25.9%) and medication (n= 2/14, 14.3%) groups (P= 0.001).Phosphate/glycerin enemas, lactulose, and glycerin suppositories were used in 30 (19.6%), 28 (18.3%), and 24 (15.6%) patients, respectively.Laxatives and whole-bowel irrigation were administered to one patient who ingested mercury.Among the patients who ingested medication, two received gastric lavage, and two were given activated charcoal.
Seven types of endoscopic and surgical complications were detected in 39 (26.4%) out of 148 patients with available data (Table 5).Some patients experienced more than one complication.Overall, patients who ingested caustics had more complications than those in the other groups (P= 0.036) in the form of mucosal erythema (P= 0.005) and strictures (P=0.019).Gastrointestinal perforation developed in the FB group only (n= 5, 3.4%) and was more with magnet ingestion (4 patients) than with other FB types (one with battery and none with others) (P< 0.001).Examples of complications caused by battery and magnet bead ingestion are shown in Figures 2 and 3, respectively.Patients who ingested the medications showed no endoscopic or surgical complications.Data from follow-up out-patient visits were available for 49 (32%)patients.Median follow-up period was 2 (IQR = 1.7-6.2) wk.
A comparison between the FB and caustic groups with respect to the presence or absence of endoscopic and surgical complications is shown in Table 6.In patients with FB ingestion, patients aged < 1 year (P= 0.042), those with middle or low SES (P= 0.028), and those with more symptoms at presentation (P= 0.027) had more complications.Both the FB and caustic groups with complications had longer hospital stays (P< 0.001) than those without.There were no significant differences in sex, nationality, maternal occupation, number of siblings, presence of witnesses, time to presentation,number and type of ingested FBs, or anatomical location.
DISCUSSION
This study observed an increasing trend in the incidence of accidental ingestion among children.This may be attributed to the increasing number of battery-powered electronic devices and the increased incidence of disc battery ingestion over the past several years[2,5].
The present study showed a male predominance among children with accidental ingestions, where boys accounted for 55.7%.Some accidental ingestion patterns may also be related to sex[6].In fact, there was a consensus among all the reviewed studies that boys form the majority of children with accidental ingestion (Table 7)[2,4,6-17].However, there were some variations in percentages.For instance, Dereciet al[13] from Turkey showed that boys accounted for 56%,which is similar to our study.However, Diaconescuet al[14] reported a male predominance, but with a lower percentage(52.45%), while Chanet al[9] reported a higher proportion of boys (80%).This finding may be explained by the fact that boys are more active and explore more[16].However, some FBs are more accessible to girls than to boys andvice versa[6].For instance, girls frequently consume jewelry and hair products[6].This finding was confirmed in the present study.In a study by Orsagh-Yentiset al[6], girls were 2.5 times more likely to swallow jewelry than boys.Speidelet al[4] also found that girls were at higher risk of sharp object ingestion.
The current study found that the median age at presentation was 2.8 years, and the most frequent age group was between 2-3 years old, accounting for 43.4%.This finding is consistent with several other studies showing that the toddler age group is the most frequent risk factor for accidental ingestion[2,4,6-10,14,17].This high prevalence of accidental ingestion in younger age groups can be attributed to the exploratory habits of these children[14].Furthermore, children in the oral phase are prone to ingesting objects while crawling and playing[7].Several studies have attributed the high prevalence of FB ingestion to the accessibility of FBs in a child’s environment, especially because this age group has the desire to explore their surroundings[1,6,16,18].However, few studies have reported older age groups up to adulthood[11,13,15,16,18].
In the current study, we evaluated families’ SES as a risk factor for the increased incidence of accidental ingestion, as the child might be left alone at home unwitnessed by the parents/caregivers owing to their work obligations, as stated by Kalraet al[16].Despite that, we did not observe an overall significant difference between families of different SES.However, in patients who ingested FBs, families with middle or low SES had more endoscopic and surgical complications than those with higher SES families (P= 0.028).
In this study, 57.3% (86/150) of the patients were symptomatic at presentation.This is comparable to the studies by Speidelet al[4] and Khoranaet al[17], where the percentages of symptomatic patients were 51.6% and 55.67%,respectively.However, studies by Ubaet al[7] and Diaconescuet al[14] reported higher percentages of symptomatic patients (85% and 70.5%, respectively).In contrast, Chanet al[9] and Leeet al[10] reported very low percentages of symptomatic patients, with 12% and 9.2%, respectively.This variation in the percentage of symptomatic patients who ingested FBs or other materials can be attributed to the differences in the time from ingestion to presentation and the shape, type, location, and amount of the ingested object[14,15].
Overall, the most frequent presenting symptom in our study was vomiting (29.3%).In the literature review, we found variations in the presenting symptoms depending on the type of FBs/materials ingested or the site of the FB impaction[15].In terms of the type of ingestion, caustic materials exhibited the highest percentage of symptoms (89.7%) in this study.A lower percentage of symptomatic patients who ingested cleansers was reported by Speidelet al[4] (53.4%).In the FB group, 48.6% of our patients were symptomatic, and 21.9% had vomiting as the most common symptom.Khoranaet al[17] reported a higher percentage of symptomatic patients with FB ingestion (55.67%), and vomiting was also the commonest presenting symptom (23.2%).Moreover, Diaconescuet al[14] reported symptoms in 70.5% of their patients with FB ingestion, yet they mainly presented with abdominal pain (55.73%), followed by vomiting (34.42%).Upon comparison of symptoms according to the lodgment site, most patients with esophageal FBs were symptomatic in our study (87.5%).This was comparable to the percentage reported by Ubaet al[7] in patients with esophageal FBs (85%).

Table 5 Endoscopic and surgical complications in children with accidental ingestion based on type of ingested materials (n = 153)
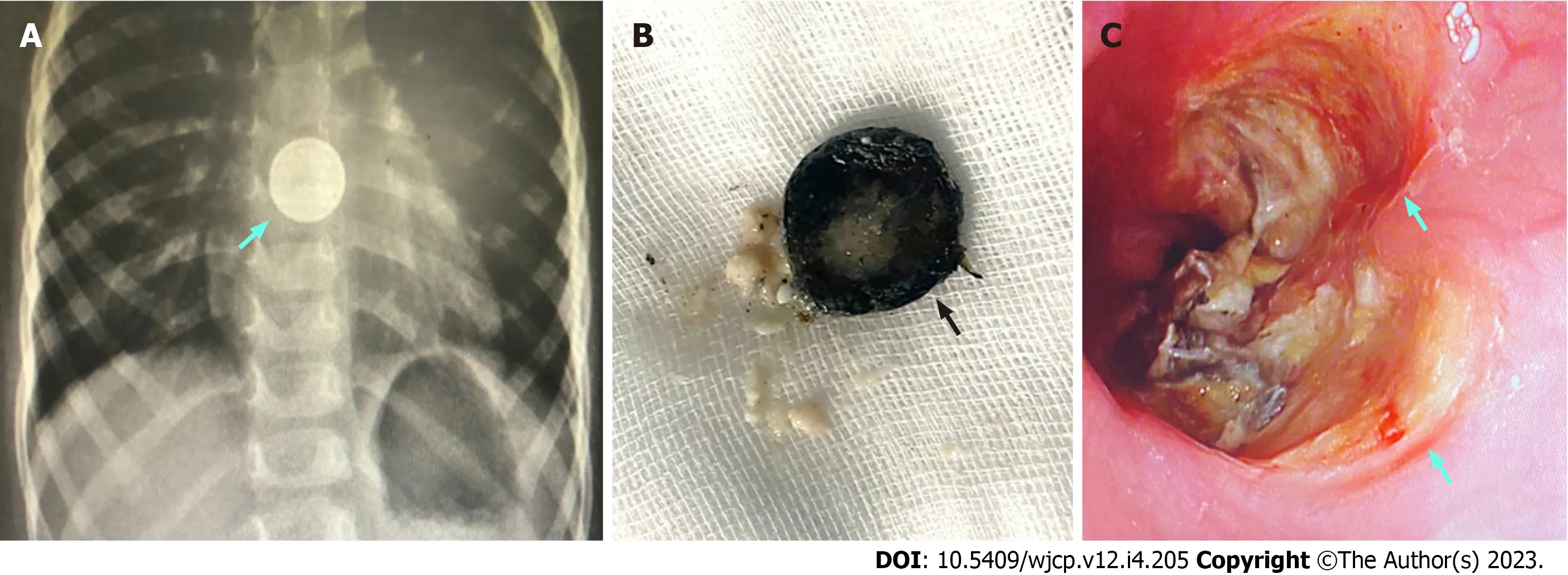
Figure 2 Disc battery ingestion in children.A: Plain chest X-ray revealing the double hallow shadow of a disc battery impacted in the esophagus; B: Rusted and friable disc battery after endoscopic removal; C: Endoscopic picture of the esophagus showing two large kissing mucosal ulcers at the site of the disc battery impaction.
Drooling of saliva and dysphagia are the main symptoms in patients with esophageal FBs[8,13], while abdominal pain and vomiting are the main symptoms in patients with FBs found in the stomach[14,15].Diaconescuet al[14] explained the wide variation in presenting symptoms among different studies based on the shape of the FB, duration between the ingestion event and time to presentation, and age of the patient.
In the current study, 42.7% of the children who ingested FBs, caustics, or medications were asymptomatic.This is comparable to the study by Speidelet al[4], who also included the three types of ingested materials, where the percentage of asymptomatic patients was 48.4%.Moreover, Leeet al[10] reported that most of the 76 patients with FB ingestions were asymptomatic (90.8%), which was also the case in our study, but at a lower rate (51.4%).Chanet al[9] also documented that most of the 25 patients with button battery ingestion were asymptomatic (88%).This high percentage of asymptomatic patients is of concern, as it may lead to delayed diagnosis in many cases, putting these children at risk of a higher rate of complications.Preventing complications and missed diagnoses, particularly in high-risk objects, such as batteries,is important.Early detection of an incident by parents leads to faster presentation, diagnosis, and intervention[3,19].Nevertheless, doctors should consider FB ingestion scenarios in young patients who present with vague symptoms, such as abdominal pain and vomiting[3,19].
In this study, the majority of the ingestion scenarios were during the playing time (40.5%) and were unwitnessed(57.4%).Ingestion episodes while playing were also documented by Dereciet al[13] but at a higher rate (72%).Unwitnessed events were also found in other studies, such as those illustrated by Litovitzet al[19] who reported a comparable percentage to our study (56.2%).In contrast, most of accidental ingestions reported by Linet al[15] were witnessed (89%).However, Kalraet al[16] found a low percentage of witnessed accidental ingestions (19%).The presence of a witness during the child’s play is important for the early detection of ingestion episodes and might hasten medical management.
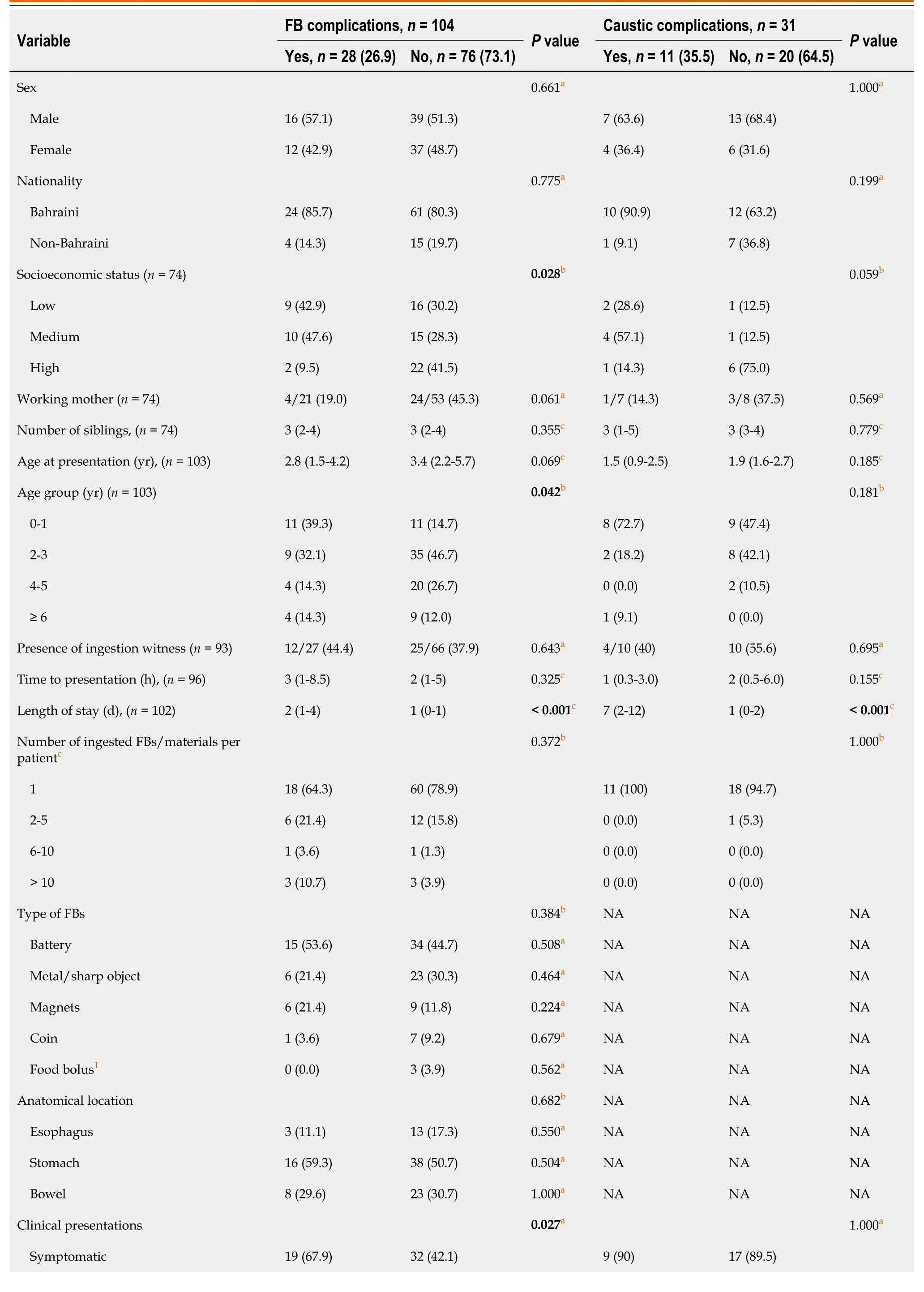
Table 6 Predictors of complications in children with accidental ingestion based on type of ingested materials (foreign body or caustic material)

aFisher’s exact test was used for categorical variables.bPearson’s χ2 test was used for categorical variables.cMann-Whitney U test was used for continuous variables.1Intact grape, olive, and pistachio nut (n = 1 each).Boldface indicates a statistically significant difference with P < 0.05.Data are presented as number (%) or median (interquartile range).FB: Foreign body;NA: Not applicable.
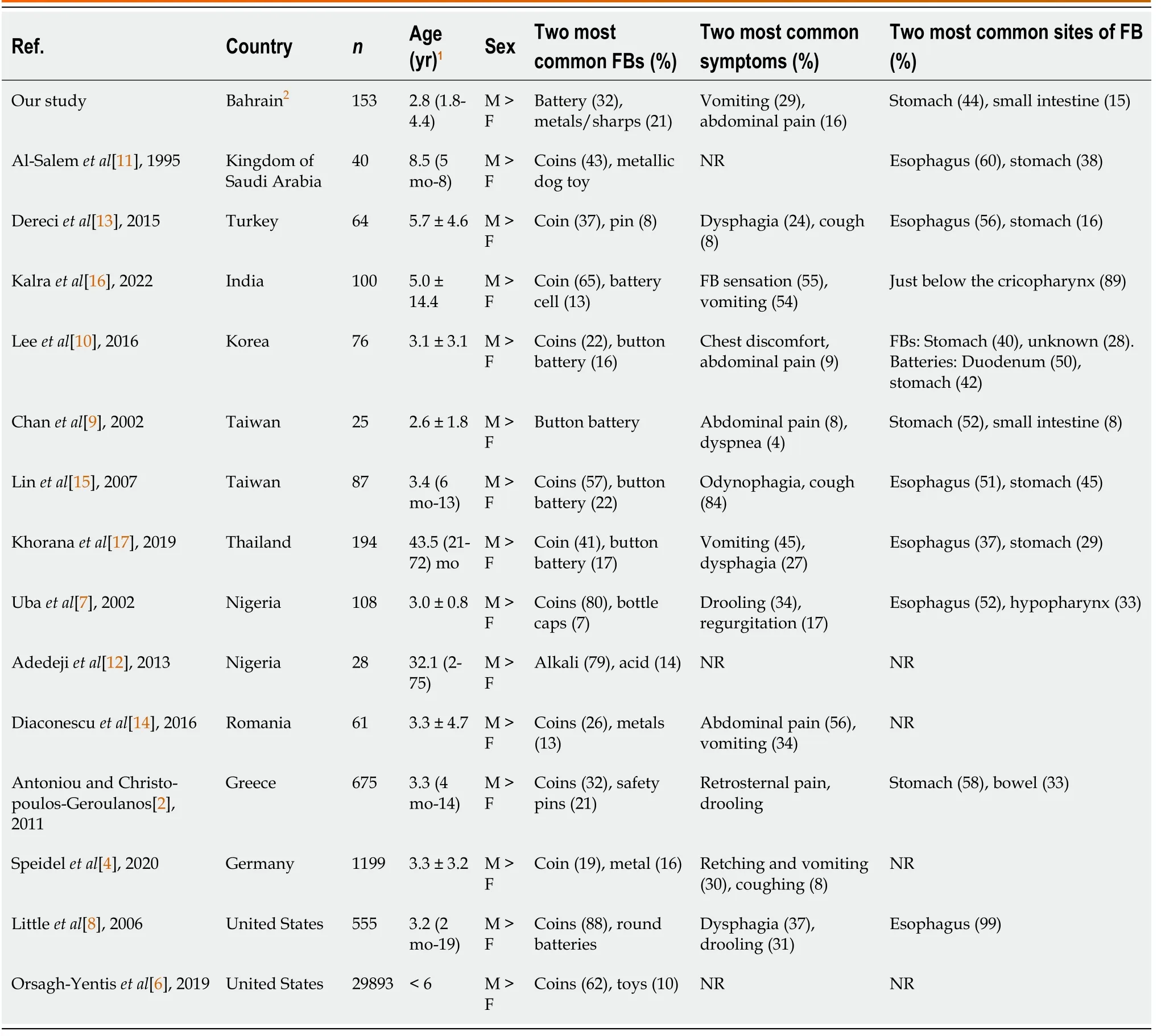
Table 7 Summary of foreign body ingestion in children from neighboring counties and worldwide
In our study, the most frequently ingested FBs were batteries (32%), followed by chemical solutions (20.3%).The main source of ingested batteries was unsafe toys (51.2%).Unsafe toys are a source of danger, particularly if their batteries are not locked.This may be due to the ease of swallowing these objects and/or being within reach of the children.However,our findings are not compatible with those of many other studies on the most commonly ingested FBs.Most studies have reported that coins are the most common[2,6-8,10,11,13,14].This can be explained by the strict inclusion criteria of our study, in which patients were admitted to the hospital for observation and for the inclusion of possible endoscopic procedures.Most patients who ingested coins at our hospital were seen in the Department of Emergency, and if the coin was in the stomach or beyond, the patient was discharged if he or she was asymptomatic.Because a significant number of patients with accidental ingestion present to the hospital without any symptoms, the implementation of specific investigations and diagnostic modalities, such as erect chest radiography, technetium-labelled sucralfate scan, and early esophago-gastroduodenoscopy, is important to establish any anatomical-internal injuries[4].The decision to perform an endoscopic procedure to remove a FB depends on the time since ingestion, FB location, size, and shape, as well as the patient’s age, symptoms, and complications[10].In our study, both radiologically and endoscopically, FBs were mostly found in the stomach, followed by the small bowel, and then the esophagus, with 37.7%, 19.7%, and 14.7%, respectively.However, the study by Linet al[15],which was conducted on 87 patients who underwent an endoscopic procedure,showed that the most common lodgment site of FBs was the esophagus (51.4%), followed by the stomach (44.6%) and finally the duodenum (4%).
Fortunately, most of our patients did not develop complications (73.6%).However, 26.4% had endoscopic and surgical complications, 10.8% developed mucosal erythema, 9.5% had ulcer, 6.1% had erosions, and 3.4% had gastrointestinal perforation (n= 5).Ubaet al[7] illustrated that the most common comorbidities were hemorrhage (15%), perforation(3.7%), and aspiration pneumonitis (2.8%).
In our study, 38.2% (n= 58) of the patients had a spon-taneous passage of the FBs.However, higher rates of spontaneous passage have been documented.Chanet al[9] and Khoranaet al[17] reported percentages of spontaneous passages that reached 92% and 60.31%, respectively.Accordingly, it was thought that the actual number of ingested FBs in children was higher than the documented number, since many cases had uneventful and symptomless spontaneous passage without the recognition and witnessing of the parents[13].In our study, 30.3% of children underwent endoscopic procedures either to remove the FB or for the assessment/management of any complications.However, Dereciet al[13]reported a higher percentage of endoscopic procedures (n= 55, 85%).Fortunately, the overall need for surgical intervention reported in the literature is relatively low.In our study, five (3.3%) cases needed surgical intervention.Speidelet al[4] showed an even lower percentage (n= 4; 0.3%).
Limitations
This study had several limitations.As this was a retrospective study, missing data, such as patient contact number,presence of a witness, and details of the ingestion scenario, were expected.One of the limitations of this study was that we included only those who had been admitted to the hospital, excluding those who attended the Departments of Accident and Emergency and were discharged home, especially asymptomatic patients and those who ingested metallic coins found in the stomach or beyond.Moreover, the ingestion scenario of some patients was gatheredviatelephone calls to the child’s parents/guardians after the ingestion episode, which was subject to recall bias.Some parents did not provide consent for endoscopy, especially for children who ingested corrosives, which made the assessment of local injury and gastrointestinal complications difficult.The ingestion of glass is a real challenge because it is radiolucent, and nothing was seen on the X-ray to determine the location.Despite these limitations, this study had many strengths.It is the first study from Bahrain to focus on accidental ingestion in children.This covered all types of accidental ingestion, unlike most other studies, which included the ingestion of only one type of hazardous material.The findings of this study are particularly important for health care providers dealing with this group of patients.They are also valuable for policymakers as prevention guidelines and legislation are crucial for protecting children from avoidable risks.
CONCLUSION
Accidental ingestion of FBs/harmful materials in children is a serious problem.Our study showed that boys and toddlers were at a higher such risk.Most children were symp-tomatic at presentation, with vomiting being the predominant symptom.Batteries were the most commonly ingested materials, followed by metals and chemicals.Most accidents occur while children playing games unwitnessed.Patients who ingested chemicals had higher endoscopic morbidity than the FB or drug group.In patients with FB ingestion, younger age (less than 1 year), those from middle- and low-SES families,and those with more symptoms at presentation, were more prone to complications.Gastrointestinal perforation developed in the FB group only, and mainly after magnet ingestion.Further studies are required to assess the impact of parental education, government legislation, and ensuring a safe environment to prevent such serious accidents in children.
ARTICLE HIGHLIGHTS

ACKNOWLEDGEMENTS
The authors gratefully acknowledge all heath care providers taking care of children with accidental ingestion in the Department of Pediatrics and Pediatric Surgery Division at Salmaniya Medical Complex, Manama, Bahrain.
FOOTNOTES
Author contributions:Isa HM was the main contributor in study conceptualization, data curation, formal analysis, investigation,methodology, project administration, resources, software, supervision, validation, visualization, original draft writing, and manuscript review and editing; Aldoseri SA, Abduljabbar AS, and Alsulaiti KA were responsible for literature review, data collection, and manuscript drafting and revision; and all the authors have read and approved the final manuscript.
Institutional review board statement:This study was conducted in accordance with the principles of the Declaration of Helsinki, and it was ethically approved by the Secondary Health Care Research Committee, Salmaniya Medical Complex, Government Hospitals,Kingdom of Bahrain (IRB number: 88300719, July 30, 2019).
Informed consent statement:Consent was not needed as the study was retrospective without exposure to the patients’ data.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Data sharing statement:Data are available upon reasonable request.
STROBE statement:The authors have read the STROBE Statement-checklist of items, and the manuscript was prepared and revised according to the STROBE Statement-checklist of items.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Bahrain
ORCID number:Hasan M Isa 0000-0001-6022-5576; Shaikha A Aldoseri 0000-0001-5533-7119; Aysha S Abduljabbar 0000-0002-6028-9198;Khaled A Alsulaiti 0000-0002-3057-3833.
S-Editor:Wang JJ
L-Editor:Wang TQ
P-Editor:Wang JJ
杂志排行
World Journal of Clinical Pediatrics的其它文章
- Use of endolumenal functional lumen imaging probe in investigating paediatric gastrointestinal motility disorders
- Role of gastrointestinal health in managing children with autism spectrum disorder
- Gastrointestinal and nutritional care in pediatric neuromuscular disorders
- Safety and efficacy of intravitreal anti vascular endothelial growth factor for severe posterior retinopathy of prematurity with flat fibrovascular proliferation
- Radiation dose analysis of computed tomography coronary angiography in Children with Kawasaki disease
- Transient hyperphosphatasemia in a toddler with COVID-19 infection: A case report and literature review