Gastrointestinal and nutritional care in pediatric neuromuscular disorders
2023-11-16ValeriaDipasqualeRossellaMorelloClaudioRomano
Valeria Dipasquale, Rossella Morello, Claudio Romano
Abstract
Key Words: Neuromuscular disorders; Diet; Malnutrition; Overweight; Dysphagia; Gastrointestinal dysmotility; Gastrointestinal symptoms; Tube feeding
INTRODUCTION
Pediatric neuromuscular disorders (NMDs) include a variety of diseases where the peripheral nervous system is the main site of abnormalities or damage.These include disorders of the anterior horn cell (i.e., spinal muscular atrophy, poliomyelitis, and amyotrophic lateral sclerosis), peripheral nerve (i.e., Charcot-Marie-Tooth disease), neuromuscular junction (i.e., congenital myasthenic syndrome), and musculature (i.e., myopathies and muscular dystrophies)[1].The main and most frequent symptom in NMDs is hypotonia, which leads to muscle weakness, fatigue, reduced mobility, and decreased physical performance.Furthermore, a deterioration of the quality of life for NMD patients and their families is frequently brought on by orthopedic, cardiac, infectious, and respiratory issues[2].Nutritional and gastrointestinal complications are also frequent in NMDs, but they are sometimes underestimated[2].Compared with the general pediatric population,infants and children with NMDs are at higher risk of malnutrition, ranging from failure to thrive to being overweight or obese (Table 1)[3,4].
Moreover, they present an increased risk of developing chronic gastrointestinal (GI) conditions such as constipation,gastroesophageal reflux disease (GERD), dysphagia, and delayed gastric emptying.Several aspects related to nutrition need to be considered when prolonging survival in patients with NMD, including the negative impact of overnutrition on glucose metabolism, mobility, respiratory, and cardiac function and the effects of undernutrition on muscle development and strength ventilation function.In addition, difficulty chewing and swallowing can lead to a higher risk of aspiration,which predisposes to infectious diseases and respiratory issues[2].Micronutrient deficiencies, such as vitamin D and calcium deficiencies, can affect bone health, particularly in children with Duchenne muscular dystrophy (DMD) who receive steroids (side effects include bone loss and fractures)[4,5].
The importance of optimal nutritional and GI management lies in reducing complications and mortality and improving the quality of life in this group of patients[4,5].A particular attention to these issues is required with an early and appropriate approach.The purpose of this review is to describe the spectrum of nutritional problems in children with NMD and to provide specific dietary and GI recommendations for each NMD.
MATERIALS AND METHODS
For this review, relevant studies published over the last 20 years were identifiedviaa PubMed/Medline (http://www.ncbi.nlm.nih.gov/pubmed/) search using the following keywords or combinations of keywords: neuromuscular disorders, malnutrition, overnutrition, diet, GI symptoms, management, guidelines.All of the most common neuromuscular disorders were afterwards used as search terms to review literature data regarding the GI and nutritional issues.Particular emphasis was placed on evidence-based guidelines and all high-quality studies illustrating current management pathways.Additional papers were identified by reviewing reference lists of relevant publications.Non-English publications were excluded.A systematic approach to study selection was not implemented.Instead, data were extracted based on their relevance to the topic.
RESULTS
Duchenne muscolar dystrophy
DMD is an X-linked recessive disorder caused by out-of-frame mutations in the dystrophin gene (DMD; locus Xp21.2).These mutations result in a deficiency or absence of the protein dystrophin, leading to progressive muscle degeneration and the loss of the ability to walk independently[6].The type of mutation and how it affects dystrophin synthesis are the primary factors in the different phenotypic expression[6].There are also milder allelic forms of the disease, such as intermediate muscular dystrophy and Becker muscular dystrophy, which result in loss of walking ability by ages 13-16 and over 16, respectively[7].DMD affects 1 in 3600-6000 male births and is the most common pediatric muscular dystrophy[7].Initial presentation ranges from motor delay, walking slowly, and difficulty getting up from the floor(Gower’s sign) to loss of the ability to walk and use of a wheelchair for mobility (since adolescence) without treatment[8].
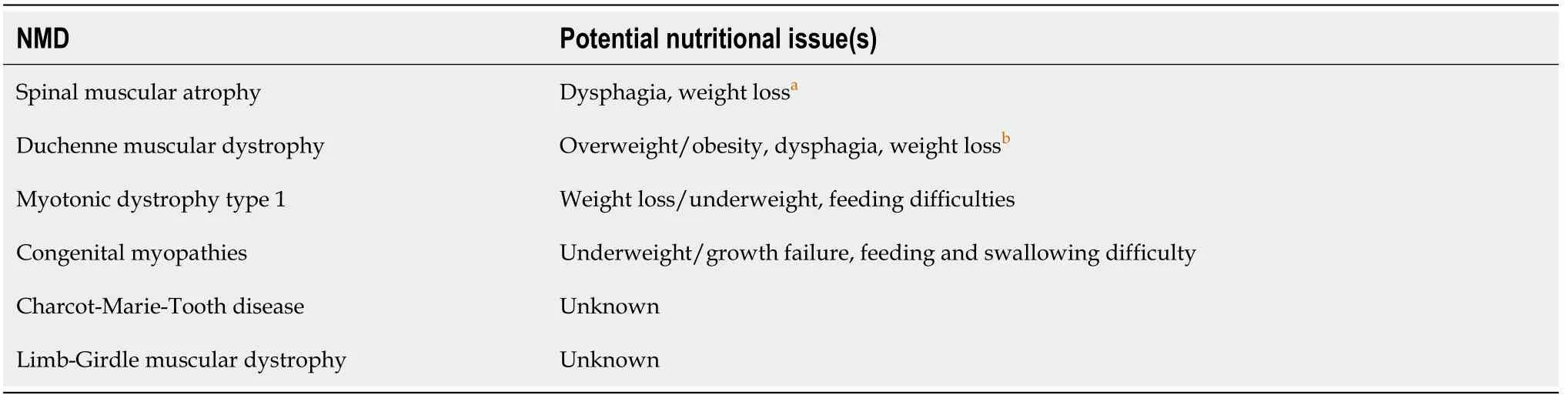
Table 1 Neuromuscular diseases and Neuromuscular disorder-related nutritional issues
Glucocorticoids (GCs) (prednisone 0.75 mg/kg/d as first-line unless otherwise indicated) are the only drugs that currently supports children with DMD in maintaining muscle strength and functionality[1].GCs are relatively well tolerated, although significant weight gain and small height gains are commonly observed.Other (rare) serious side effects include hypertension, glycosuria, osteoporosis, GI lesions, and adrenal crisis[1].
To help multidisciplinary care teams manage this complex pathology, the US Centers for Disease Control and Prevention (CDC) selected a working group in 2018 to develop DMD care recommendations, including consideration of diet and GI health[9].The most important goals in nutritional and gastrointestinal management include: (1) Optimization of macronutrient intake to avoid growth failure or obesity; (2) management of feeding and swallowing issues; (3)treatment of the GI symptoms; and (4) monitoring micronutrient intakes such as vitamin D and calcium[9].Nutritional and GI evidence for DMD children is summarized in Table 2.
Nutritional management
The purpose of nutritional management is to prevent overweight or obesity and under- or malnutrition through regular assessment of growth and weight and the promotion of a healthy, balanced diet.A registered dietitian, an essential member of the multidisciplinary DMD care team, should record the patient’s weight and height on growth charts[9].
Unlike other NMDs, specific growth curves are available for DMD.In a sample of 26 patients with DMD, Griffithset al[10] estimated total muscle mass using 24-h urine creatinine excretion and discovered a 4% loss in muscle mass per year.
The authors developed a weightvsage curve for DMD that would determine the appropriate percentile by initially identifying the percentiles on a standard percentile height table.Recent studies have revealed that urinary creatinine excretion is not a reliable predictor of skeletal muscle mass in DMD, which challenges the logic of these charts based on[11].Using recurrent growth measurements in a cohort of 513 DMD individuals aged 2 to 12 years from the Muscular Dystrophy Surveillance, Tracking, and Research Network, Westet al[12] created growth curves specifically for DMD.Based on the CDC clinical growth charts, these curves demonstrated that male DMD patients were shorter than unaffected boys and tended to be overweight.The same team, later, visited the Muscular Dystrophy Surveillance,Tracking, and Research Network cohort to survey it, and they recently presented growth data in a cohort of 324 outpatients receiving GC therapy for at least 6 mo[13].In contrast to untreated patients, this cohort had shorter stature,more weight, and a higher body mass index[9].
After a correct interpretation of the anthropometric measurements, the dietician should offer a nutritional plan that includes recommendations for increasing, decreasing, or maintaining caloric intake and water requirement as well as suggestions for modifying food textures to promote secure and pleasurable chewing and swallowing[9].
In the case of DMD and other NMDs, patient obesity is often attributed to a reduction in calorie requirements coupled with a decrease in physical activity and resting energy expenditure.In addition, chronic treatment with steroids can increase appetite and promote excess caloric intake.Instead, patients in the late stages of the disease may be malnourished and underweight[2,9].Muscle weakness and its sequelae (dysphagia, constipation, delayed gastric emptying, prolonged mealtimes, and dependent food intake) are the main causes of malnutrition, and the presence of respiratory failure can cause increased energy demands.The result of malnutrition and increased energy needs is a negative energy balance and progressive weight loss[9].
As the disease progresses, most patients begin to experience increasing difficulty with chewing and swallowing[14].The onset of dysphagia symptoms can be gradual, and the impact of oral-pharyngeal dysphagia might be underrecognized and under-reported by patients[15].Dysphagia may manifest as unintentional weight loss or a slowing of the normal age-related weight growth.Tube feedingviagastrostomy should be considered early in patients with DMD.In the absence of symptoms consistent with suspected GERD, a polymeric formula may be considered initially.Alternatively,bolus feeding with home-made foods can be suggested and effective in children with chronic constipation[9].
According to the 2018 DMD Care Considerations, serum calcium and 25-hydroxyvitamin D levels should be regularly monitored once a year as part of routine bone health management.Vitamin D and mineral supplementation should be considered in all children if levels cannot be maintained[15].
GI symptoms management
The most common GI symptoms in DMD patients are GERD and constipation.GER may be related to altered gastric smooth muscle cell emptying function.Treatment includes the early use of proton pump inhibitors.Regarding constipation, the use of polyethylene glycol after gastrostomy placement is recommended to prevent the use of high oral volumes, both of which are associated with the risk of bronchoaspiration[2].Increasing fiber intake or using natural food enteral formulas could also be considered to treat constipation[16,17].
SPINAL MUSCULAR ATROPHY
Spinal muscular atrophy (SMA) is an autosomal recessive neurodegenerative disease caused by a homozygous mutation or deletion in the survival motor neuron 1 (SMN1) gene.Defects in the SMN1 gene cause the selective destruction of alpha motor neurons in the anterior horn cells of the spinal cord and brainstem.Clinical manifestations include muscle atrophy and weakness, resulting in swallowing and feeding difficulties and respiratory complications.SMA affects approximately one in 6000-10000 newborns worldwide[18].The classification of SMA consists of four subtypes based on age of onset and maximal functional ability: very weak infants unable to sit unsupported, onset < 6 mo of age (type 1),nonambulant patients able to sit independently, onset between 6 and 18 mo of age (type 2), ambulant patients with onset between 18 mo and 18 years (type 3), and adult onset SMA (type 4).
The SMA multidisciplinary care focuses on reducing complications and improving quality of life.Symptoms of GI dysfunction, including constipation, delayed gastric emptying, and GERD, are important determinants of mortality and morbidity, for example dysphagia and reflux can lead to pulmonary disease[19].
In 2007, a consensus statement was published by the International Conference on the Standard of Care for SMA.A two-part update of the topics covered in the prior recommendations was published in 2018 as a result of the more current data publications and more generally made advancements in the themes mentioned in the original version[20].
One of the nine topics included in this update focused on nutrition.The main nutritional goals, which are slightly different for each type of SMA, include weight control, swallowing and dysphagia management, and management of GI dysfunction.Regular growth checks are important for all SMA types.Growth and body composition are measured using a variety of methods, such as basic anthropometry, dual-energy X-ray absorptiometry, and bioelectrical impedance analysis[19,20].
Specific growth charts for SMA are not currently available.Due to modifying body composition in standardized SMA growth charts, it may be helpful to monitor growth trends rather than monitor weight.In contrast, children with SMA type III are prone to overeating and obesity from physical inactivity and have reduced energy needs due to lower basal metabolic rates[3].
For optimal care, a nutritionist assessment is recommended every 3-6 mo for younger children and annually for older children and adults[20].In addition, a qualified dietician should also promote healthy nutrition and keep track of hydration, macronutrient, and micronutrient intake, particularly calcium and vitamin D intake for bone health.Calcium and vitamin D supplements are recommended if the levels are low.It’s crucial to inquire and record the specifics of GI symptoms in all subjects, which could include GERD, constipation, use of bowel regulators, delayed gastric emptying,and vomiting.
Infants and children with SMA types I and II should receive gastrostomies in the first few months of life to avoid the risk of malnutrition.This approach is also recommended to reduce the risk of respiratory infections[20].Nutritional and GI evidence for SMA children is summarized in Table 3.
Non-sitter patients
Some aspects of nutrition assessments and interventions can differ among non-sitters, sitters, and ambulant patients[20].One of the most significant considerations to take into account for a non-sitting child is safe swallowing, as bulbar dysfunction can lead to aspiration and lung infections.Recent data suggest that children with SMA type 1 should have avideofluoroscopic swallow examination soon after diagnosis and when there are clinical indications suggestive of dysphagia (weak sucking, fatigue, a wet voice, pneumonia) to assess bulbar function and prevent growth failure[21,22].In type 1 patient, reduced caloric intake and the possibility of malnutrition are caused by respiratory issues, dysphagia,and weak masticatory muscles.In addition, tachypnea can increase energy expenditure and calorie needs, further increasing the risk of malnutrition[20].
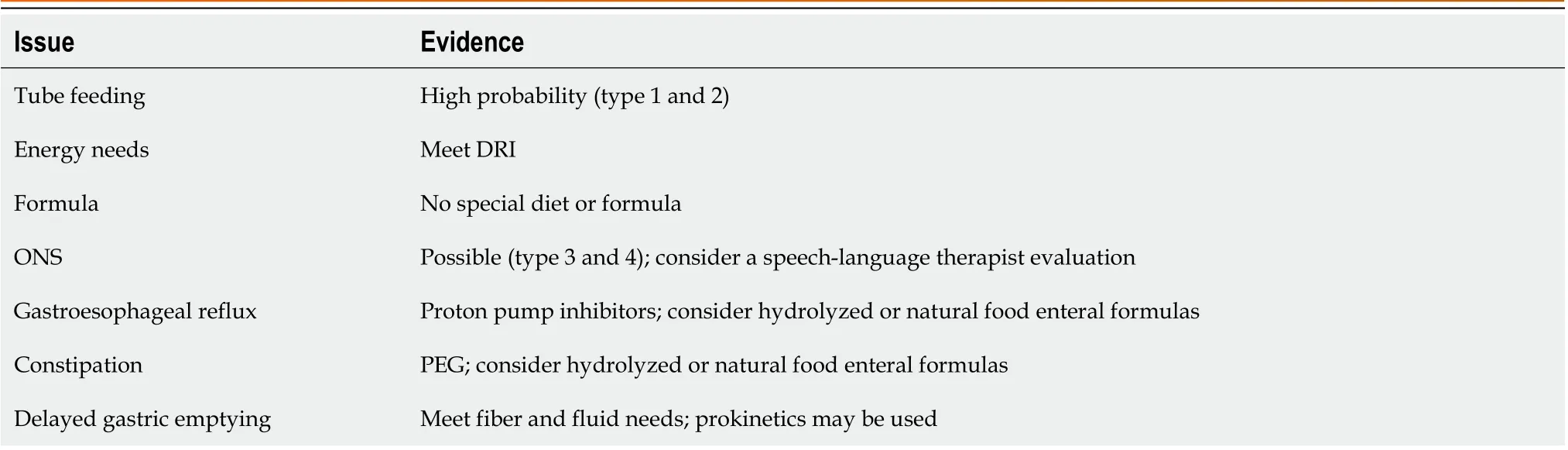
Table 3 Nutritional and gastrointestinal management in children with spinal muscular atrophy
Sitter patients
Sitter patients may have a higher risk of being overweight or obese as a result of reductions in physical activity due to weakness and altered body composition[3,23].Obesity can lead to reduced mobility and increased risks for associated comorbidities, including the metabolic syndrome.
Walkers
Swallowing disorders and feeding problems are rare in walkers[20].The main nutritional concern is the risk of obesity and overweight, as these conditions can impair mobility and raise the possibility of comorbidities like metabolic syndrome, hypertension, and diabetes[3,20].
CHARCOT-MARIE-TOOTH DISEASE
Charcot-Marie-Tooth disease (CMT) is the most common inherited NMD with an estimated prevalence of up to 40 in 100000 people, which corresponds to 200000 cases in the European Union[24].The disease generally appears in the first two decades of life and progresses slowly over many years.It is a genetically heterogeneous disorder resulting from mutations in genes that encode proteins in various locations, which include compact and non-compact myelin, Schwann cells, and axons.These proteins are involved in a wide variety of functions, including myelin compaction and maintenance, formation of the cytoskeleton and axonal transport rich, as well as mitochondrial metabolism[25].Since motor and sensory peripheral nerves are affected, CMT is also known as hereditary motor and sensory neuropathy.Distal weakness, hand and foot deformities, slow loss of sensory perception, and mild to moderate disability are the most common clinical phenotypes.
There is still no effective drug therapy for CMT.A multidisciplinary approach is necessary for therapeutic management; the neurologist should work closely with other professionals such as orthopedics for the surgical treatment of skeletal deformities and soft tissue anomalies[1,25].
There are no specific nutritional recommendations for this patient group, and the nutritional approach must be evaluated individually.Sometimes the use of oral nutritional supplements may be recommended.Skeletal deformities may be associated with an increased risk of GERD.
CONGENITAL MUSCULAR DYSTROPHIES
Congenital muscular dystrophies (CMD) are a group of genetic neuromuscular disorders defined by muscle weakness that appears at birth or in the first few months of life and the presence of dystrophic biopsies and/or increased creatine kinase, two markers that are diagnostic of a muscular dystrophy[26].The identification of different CMD subtypes backed by precise gene identification has been made possible by developments in molecular genetics and histopathology techniques[27].Despite rapid advances in basic research, clinical care for patients with CMD remains poor due to the rarity of this pathology and the difficulty of differentiating clinical phenotypes.
The International Standard of Care Committee for Congenital Muscular Dystrophy published a consensus statement in November 2009 on standards of medical care divided into 7 areas: Diagnosis, neurology, pulmonology, orthopedics,gastroenterology and nutrition, speech, and oral care, cardiology, and palliative care[28].Main topics are nutrition and growth, food intake, GI motility, and oral care[28].There are no specific growth charts or data on the energy and nutritional needs of CMD children, and this makes monitoring nutrition and growth even more difficult[28].Patients with CMD often have a growth trajectory that is below age, and one of the most typical childhood problems is malnutrition and poor weight gain.Instead, obesity should be considered in adults due to the limited mobility of these patients.
In this group of patients, special attention needs to be paid to feeding and swallowing problems, which should be evaluated regularly during routine clinic visits, asking about: (1) Length of meals; (2) frequency of meals; (3) frequency of lung infections; (4) difficulty chewing (choking and coughing); (5) change in the structure of food; (6) stress in the family or enjoyment of meals for the child and parents; and (7) ability to eat independently.Videofluoroscopy can reveal difficulties in the oral phase, a delay in pharyngeal swallowing, and increased risks with aspiration[28].In the case of dysphagia and feeding problems, treatment strategies may include adjustments in standing positioning and sitting,support for self-feeding, which include adjustment of feeding utensils and devices, safe swallowing procedures, and texture modification.When symptomatic treatment is inadequate, the use of tube feeding must be considered.
GERD and GI dysmotility,i.e., delayed gastric emptying and constipation, are common in CMD patients.In order to minimize the risk of gastroesophageal reflux and dysmotility, the frequency and volume of tube feeding should be adjusted and attention should be paid to adequate fluid intake, posture, and movement.Medical treatment includes use of proton pump inhibitors and treatment with antacids and laxatives for GERD and constipation, respectively[28].Increasing fiber intake or using natural food enteral formulas could also be considered to treat constipation[16,17].
MYOTONIC DYSTROPHY
Myotonic dystrophy (MD) is the most common form of muscular dystrophy in adults, with an estimated prevalence of 1 in 8000[29].Myotonia and muscular dystrophy were traditionally used to name this multisystem condition.Myotonic dystrophy type 1 (MD1, Steinert disease) is caused by a cytosine, thymine, and guanine repeat expansion in the 3rduntranslated region of the myotonic dystrophy protein kinase gene on chromosome 19[30].MD1 patients range from asymptomatic or moderately severe, late adult onset to severe congenital variants, with an autosomal dominant inheritance pattern.In particular, congenital MD is the most severe form and may present prenatally with polyhydramnios and reduced fetal movements.
Respiratory failure, hypotension, feeding difficulty, weakness, and tented or fish-shaped upper lips are all frequent at birth[30].Facial weakness, dysarthria, myotonia, low intellect, and cardiac conduction anomalies characterize the childhood-onset (1-10 years) phenotype[31].Patients may gradually present with early cataracts, myotonia, muscle weakness or atrophy, fatigue, excessive daytime sleepiness, central or obstructive apnea, respiratory failure, cardiac arrhythmia, insulin resistance, dysphagia, GI dysmotility, cognitive impairment, cluster C personality traits, and/or mood swings.
No particular dietary risks are reported for MD patients, although each patient must be assessed on an individual basis.The major GI problems that arise during the course of the disease are dysphagia, postprandial bloating or abdominal pain, diarrhea, constipation, and/or fecal incontinence, and cholelithiasis[31].Drug therapy for the treatment of GERD does not differ from that for other patient groups[32].
CONCLUSION
The management of children with NMDs, who frequently present with nutritional issues like inappropriate weight and body composition, difficulty swallowing and feeding, constipation, and GERD, places a high priority on nutritional care.Effective interdisciplinary management can considerably lower morbidity and mortality even though there is often no treatment available.
This present study is an unstructured, narrative review, so there are inherent limitations, such as the lack of direct comparison between studies.However, we described the methods for selecting and reviewing literature to make it possible to verify or replicate these results.Moreover, the heterogeneity of the published studies on the nutritional and GI care of pediatric patients with NMDs made it challenging to implement a systematic approach to study selection and interpretation.The aims of the present article were to report the spectrum of nutritional problems in children with NMD and to provide clinicians with specific dietary and GI directions for each NMD while highlighting the knowledge gaps in this topic.There are no specific nutritional and GI recommendations for all of the NMDs in the scientific literature currently available, especially in the pediatric age group.More nutritional and GI data are available for DMD and SMA.Future studies should focus on creating disease-specific treatment guidelines, including dietary recommendations based on age group, physical activity status, and swallowing problems.This patient population is at high nutritional risk, so a proactive attitude is recommended.The clinician should plan for the early use of tube feeding and the appropriate selection of the most appropriate formula, with a particular interest in enteral hydrolyzed formulas.In terms of GI symptoms, the greatest challenges lie in the treatment of GERD and chronic constipation.The use of drugs to inhibit acid secretion should be prompt.The possibility of increasing fiber intake or the use of natural food formulas in enteral feeding should also be considered to further assist in the management of constipation.
FOOTNOTES
Author contributions:Dipasquale V, Morello R and Romano C equally contributed to the article.Conflict-of-interest statement:All the authors declare no conflict of interests for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Italy
ORCID number:Valeria Dipasquale 0000-0003-3328-0734.
S-Editor:Liu JH
L-Editor:A
P-Editor:Yuan YY
杂志排行
World Journal of Clinical Pediatrics的其它文章
- Use of endolumenal functional lumen imaging probe in investigating paediatric gastrointestinal motility disorders
- Role of gastrointestinal health in managing children with autism spectrum disorder
- Accidental ingestion of foreign bodies/harmful materials in children from Bahrain: A retrospective cohort study
- Safety and efficacy of intravitreal anti vascular endothelial growth factor for severe posterior retinopathy of prematurity with flat fibrovascular proliferation
- Radiation dose analysis of computed tomography coronary angiography in Children with Kawasaki disease
- Transient hyperphosphatasemia in a toddler with COVID-19 infection: A case report and literature review