外用3%氨甲环酸精华液治疗黄褐斑的前瞻性研究
2023-06-23王雅玲毛梦平施为赵志祥简丹
王雅玲 毛梦平 施为 赵志祥 简丹
[摘要]目的:觀察外用3%氨甲环酸精华液治疗黄褐斑的疗效及不良反应。方法:将2021年6月-2021年12月在湘雅医院皮肤科就诊的50例黄褐斑患者按随机数字表法分为两组,实验组外用3%仙瑟氨甲环酸精华液+保湿霜,每日2次;对照组仅外用同种保湿霜,每日2次。每4周回访1次,试验周期为8周,治疗8周停止治疗,随访至12周。回访时依据黄褐斑面积及严重程度评分(Melasma area severity index,MASI)评估疗效,并根据VISIA图评估实验组患者面部红斑改善程度。治疗12周回访时评估复发率、医生及患者满意率并记录不良反应。结果:治疗后4周、8周、12周,实验组的平均MASI均低于对照组,差异具有统计学意义(P<0.05),且实验组患者面部红斑改善情况均优于对照组。随着治疗时间的延长,实验组MASI逐步下降(P<0.05),患者面部红斑改善率逐渐升高。治疗12周回访时医生满意率为88%,患者满意率为92%。结论:外用氨甲环酸治疗黄褐斑疗效肯定,但是对于不同类型的黄褐斑,在起效时间、复发上可能存在不同。配方合理的复合制剂可能是氨甲环酸外用制剂的进一步研究方向。
[关键词]氨甲环酸;黄褐斑;外用;药物治疗
[中图分类号]R758.4+2 [文献标志码]A [文章编号]1008-6455(2023)05-0006-04
Topical Application of 3% Tranexamic Acid Extract for the Treatment of Melasma Prospective Study
WANG Yaling,MAO Mengping,SHI Wei,ZHAO ZhiXiang,JIAN Dan
(Department of Dermatology,Xiangya Hospital,Central South University,Changsha 410000,Hunan,China)
Abstract: Objective To observe the efficacy and adverse effects of topical application of 3% tranexamic acid serum in melasma. Methods Fifty patients with melasma attending the Department of Dermatology at Xiangya Hospital from June 2021 to December 2021 were randomly divided into 2 groups according to the random number table method. Experimental group was treated with 3% Sencer tranexamic acid serum and moisturizing cream twice daily. Control group was treated with the same moisturizing cream only, twice daily. Returning every 4 weeks for a trial period of 8 weeks, with treatment discontinued at 8 weeks and followed up until the 12 weeks. At the follow-up visit, the efficacy of the treatment was assessed according to the Melasma Area Severity Index (MASI), and the improvement of facial erythema in the experimental group was assessed according to the VISIA chart. The recurrence rate, physician and patient satisfaction rates, and adverse effects were recorded at the return visit at week 12. Results At 4 weeks, 8 weeks and 12 weeks of treatment, , the mean MASI of the experimental group was lower than that of the control group, and the difference was statistically significant (P<0.05), and the improvement of facial erythema in the experimental group was better than the control group. With the extension of the treatment time, the MASI of the experimental group gradually decreased(P<0.05), and the improvement rate of facial erythema of patients gradually increased. The physician satisfaction rate was 88% and the patient satisfaction rate was 92% at the return visit at week 12. Conclusion The efficacy of topical tranexamic acid in the treatment of melasma is positive, but there may be differences in the time of onset of effect and recurrence for different types of melasma. A reasonably formulated compound formulation may be a further research direction for topical tranexamic acid formulation.
Key words: tranexamic acid; chloasma; topical; drug treatment
作为亚洲中青年女性最常见的面部色素性疾病,黄褐斑严重影响患者容貌美观与身心健康。目前认为黄褐斑作为亚洲女性皮肤衰老的早期表征之一,其发病被认为与日光照射[1-2]、激素水平变化[3-4]、遗传易感性[5]、化妆品、药物[6]等相关。虽然人们在黄褐斑的治疗领域不断进行新的探索,比如口服甘草酸苷、谷胱甘肽、维生素C和维生素E[7-9];外用氢醌及其衍生物、维A酸类、壬二酸[10-11];以及化学剥脱治疗、光电治疗[12-15],但目前黄褐斑治疗效果仍不理想。在黄褐斑治疗过程中,普遍存在起效慢、难治愈、易复发等问题。在一系列的治疗措施中,口服氨甲环酸被认为是一线的选择,其可竞争性抑制酪氨酸酶,减少黑色素合成,同时抑制血管增生,减轻红斑[16]。但由于其可引起胃肠道反应、月经量减少、疼痛等不良反应[17],限制了其临床应用。有研究尝试外用不同浓度、不同剂型的氨甲环酸(如2%氨甲环酸乳液、5%氨甲环酸凝胶等)治疗黄褐斑并取得了较明显的疗效[6,18-19],由此认为氨甲环酸相关外用制剂亦可在一定程度上改善黄褐斑。本研究进行了外用3%氨甲环酸精华液治疗黄褐斑的前瞻随机对照试验,观察其疗效及不良反应,旨在为选择外用氨甲环酸制剂治疗黄褐斑提供支持。
1 资料和方法
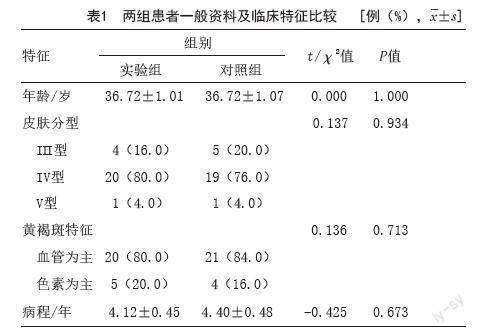
1.1一般资料:纳入2021年6月-2021年12月在湘雅医院皮肤科就诊的黄褐斑患者50例,均签署知情同意书。本研究经笔者医院伦理委员会批准。50例患者均为女性,按随机数字表法将患者分为实验组和对照组。两组患者年齡、皮肤类型、黄褐斑类型、病程比较差异无统计学意义(P>0.05),具有可比性。见表1。
1.2 纳入标准:①年龄20~60岁;②确诊为黄褐斑、可接受跟踪观察,并可提供肖像者。
1.3 排除标准:①3个月内使用过口服药物、化学剥脱、脱色剂、激光等影响面部色素状态治疗者;②妊娠期、哺乳期间的女性;③治疗前实验室检查凝血功能异常者;④患眼部疾病者;⑤面部炎症性皮肤病或感染性皮肤病者;⑥其他,例如对疗效期望值过高者。
1.4 治疗方法:实验组外用3%氨甲环酸精华液(山东烟台仙瑟商贸有限公司,批号:YH40JS46,组成成分:3%氨甲环酸、2%烟酰胺、3%豨莶草提取物)+保湿霜,每日2次;对照组仅外用同种保湿霜,每日2次。每4周回访1次,试验周期为8周,治疗8周停止治疗,随访至12周。
1.5 疗效评估:每次回访时使用VISIA肤色分析系统拍摄患者照片,由笔者医院皮肤科2位医生分别参照黄褐斑面积及严重程度评分(Melasma Area Severity Index,MASI)评估疗效。根据VISIA图评估患者面部红斑改善程度,分为四个等级:明显改善(红斑减少>75%)、改善(红斑减少50%~75%)、不明显改善(红斑减少25%~49%)、基本无改善(红斑减少<25%)。将红斑减少≥50%视为改善。治疗12周后回访时评估复发率、医生及患者满意率并记录不良反应。治疗12周时MASI回升至基线MASI评分90%以上视为复发。
1.6 统计学分析:应用SPSS 25.0统计分析。定量数据统计描述采用(x?±s)表示,定性数据统计描述采用率(%)表示。两组间比较采用t检验或卡方检验。以P<0.05为差异具有统计意义。
2 结果
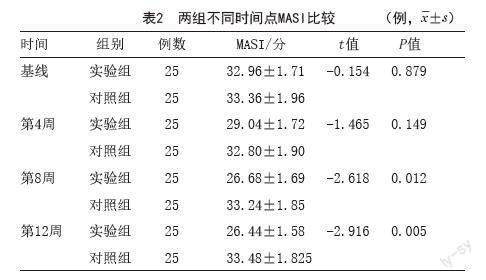
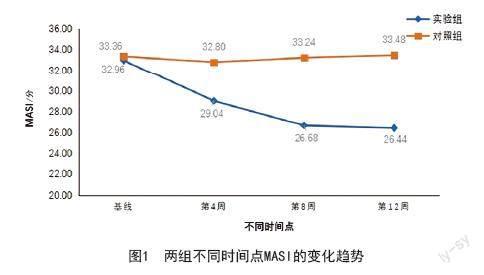
2.1 黄褐斑面积及严重程度评分(MASI):治疗后4周、8周、12周,实验组的平均MASI均低于对照组,且随着治疗时间的延长,实验组MASI逐步下降,见表2、图1。提示外用3%氨甲环酸精华液治疗4周后即可见MASI呈下降趋势,治疗8周后疗效显著,且停药4周后仍能维持较好的临床效果。实验组典型病例见图2。
2.2 面部红斑改善情况:在治疗4周、8周、12周时,实验组患者面部红斑改善情况均优于对照组,且随着治疗时间延长,实验组患者面部红斑改善率逐渐升高,见表3、图3。提示外用3%氨甲环酸精华可有效抑制黄褐斑患者面部红斑,在治疗4周时即可见红斑明显减少,治疗8周可显著抑制红斑,且在停药4周后仍能维持一定的红斑抑制作用。
2.3 医生及患者满意率:在治疗12周回访时,调查医生及患者对黄褐斑改善情况是否满意。医生满意率为88%,患者满意率为92%。
2.4 复发及不良反应:治疗12周回访时,发现实验组25例患者中有2例患者发现色斑较治疗8周时有不同程度加深,但色斑MASI评分均未达到基线MASI的90%,无复发病例。整个试验过程中,所有患者均未出现不良反应。
3 讨论
目前黄褐斑确切发病机制尚不清晰,其治疗仍具有挑战性。相关研究显示,黑色素合成增加[1-2]、皮损处血管增生[20]、炎症反应[21-22]及皮肤屏障受损[23]均参与了黄褐斑的发生[16],其中可能涉及角质形成细胞、肥大细胞、基因调控异常、新血管形成和基底膜破坏之间的相互作用等复杂机制[24],增加了黄褐斑靶向治疗的难度。关于黄褐斑皮损处的相关组织学研究显示,黄褐斑皮损处血管的数量、管径、血流量都有不同程度的增加[25];皮损处血管内皮细胞生长因子(Vascular endothelial growth factor,VEGF)的表达增加[20]。这些研究在一定程度上提示,血管功能紊乱可能是导致黄褐斑的始动因素之一。在光电治疗黄褐斑的相关研究中显示,强脉冲光等调节血管功能紊乱,去除多余的扩张血管后,黄褐斑也有不同程度的改变[26-28],但单一、反复的光电治疗易导致色素沉着、色素减退/脱失,并且有激惹黄褐斑合成功能的可能,因此不被推荐作为临床首选治疗手段[16]。
口服氨甲环酸治疗黄褐斑在临床上被认为是切实有效的治疗方式,有报道其显效率约89.7%,但有7.1%的患者被报道出现了不同程度副反应,如腹痛腹胀、头痛、耳鸣目眩、月经减少、呕吐等,并被认为有发生血栓的可能[17],这导致临床医生在使用口服氨甲环酸制剂时有诸多顾忌。有研究尝试采用外用不同浓度、不同剂型氨甲环酸治疗黄褐斑,但仍存在透皮吸收率低的问题,且约36.75%的患者出现了刺痛、红斑、脱屑等不良反应[29]。本研究尝试外用3%氨甲环酸复合精华液治疗黄褐斑,治疗4周后即显示出明顯改善趋势,治疗8周后疗效显著,这一发现与之前的报道相符[18-19]。这一作用可能与氨甲环酸减少黑素合成[30-31]、抑制血管增生、缩小血管管径及血流量相关[25,32-33]。同时,本研究发现实验组的面部炎症性红斑改善明显,这一方面与氨甲环酸对血管的抑制功能有关;另一方面,也可能与本次实验精华液中存在复合成分3%豨莶草提取物有关。豨莶草具有明确的抗炎、抗过敏等多种药理活性[34],研究证明豨莶草提取液可通过抑制肿瘤坏死因子、白细胞介素、血管细胞黏附分子等各种炎症介质来减轻炎症反应,从而进一步加强了氨甲环酸制剂的抗炎作用,对血管性黄褐斑的治疗可能更具有优势。同时豨莶草被证明起到镇痛、消炎作用[35],能明显降低外用制剂的刺激性。因此,本次临床观察过程中未发生红斑、脱屑、干燥等不良反应,也可能与复合制剂中成分的互补加强作用有关。
综上所述,氨甲环酸治疗黄褐斑疗效肯定,但是对于不同类型的黄褐斑,在起效时间、复发上可能存在不同,但由于本研究样本量较小,本文未做进一步细分。同时配方合理的复合制剂可能是氨甲环酸外用制剂的开发方向。
[参考文献]
[1]Hexsel D,Arellano I,Rendon M.Ethnic considerations in the treatment of Hispanic and Latin-American patients with hyperpigmentation[J].Br J Dermatol,2006,156(Suppl 1):S7-S12.
[2]Mahmoud B H,Ruvolo E,Hexsel C L,et al.Impact of long-wavelength UVA and visible light on melanocompetent skin[J].J Invest Dermatol,2010,130(8):2092-2097.
[3]Handel A C,Lima P B,Tonolli V M,et al.Risk factors for facial melasma in women: a case-control study[J].Br J Dermatol,2014,171(3):588-594.
[4]Costin G E,Birlea S A.What is the mechanism for melasma that so commonly accompanies human pregnancy?[J].IUBMB Life,2006,58(1):55-57.
[5]Tamega A A,Miot L D,Bonfietti C,et al.Clinical patterns and epidemiological characteristics of facial melasma in Brazilian women[J].J Eur Acad Dermatol,2013,27(2):151-156.
[6]Ebrahimi B,Naeini F F.Topical tranexamic acid as a promising treatment for melasma[J].J Res Med Sci,2014,19(8):753-757.
[7]黄骏,胡文婷,章玲玲,等.复方甘草酸苷注射液治疗黄褐斑疗效评估[J].中华皮肤科杂志,2018,51(4):299-301.
[8]Sonthalia S,Daulatabad D,Sarkar R.Glutathione as a skin whitening agent: Facts,myths, evidence and controversies[J].Indian J Dermatol Ve,2016,
82(3):262-272.
[9]Handog E B,Galang D A,Leon M A,et al.A randomized, double-blind, placebo-controlled trial of oral procyanidin with vitamins A, C, E for melasma among Filipino women[J].Int J Dermatol,2009,48(8):896-901.
[10]Hu Z M,Zhou Q,LEI T C,et al.Effects of hydroquinone and its glucoside derivatives on melanogenesis and antioxidation: Biosafety as skin whitening agents[J].J Dermatol Sci,2009,55(3):179-184.
[11]Rivas S,Pandya A G.Treatment of melasma with topical agents, peels and lasers: an evidence-based review[J].Am J Clin Dermatol,2013,14(5):
359-376.
[12]何黎,李利,張建中.果酸化学剥脱术临床应用专家共识[J].中华皮肤科杂志,2014,47(10):748-749.
[13]栾琪,刘玲,高天文.激光和强脉冲光治疗黄褐斑的进展[J].中华皮肤科杂志,2015,48(2):142-143.
[14]Mckesey J,Tovar G A,Pandya A G.Melasma treatment: an evidence-based review [J].Am J Clin Dermatol,2020,21(2):173-225.
[15]Trivedi M K,Yang F C,Cho B K.A review of laser and light therapy in melasma [J].Int J Women Dermatol,2017,3(1):11-20.
[16]中国中西医结合学会皮肤性病专业委员会色素病学组,中华医学会皮肤性病学分会白癜风研究中心,中国医师协会皮肤科医师分会色素病工作组.中国黄褐斑诊疗专家共识(2021版)[J].中华皮肤科杂志,2021,54(2):110-115.
[17]Lee H C,Thng T G,Goh C L.Oral tranexamic acid (TA) in the treatment of melasma: A retrospective analysis[J].J Am Acad Dermatol,2016,75(2):385-392.
[18]Kim S J,Park J Y,Shibata T,et al.Efficacy and possible mechanisms of topical tranexamic acid in melasma[J].Clin Exp Dermatol,2016,41(5):480-485.
[19]Banihashemi M,Zabolinejad N,Jaafari M R,et al.Comparison of therapeutic effects of liposomal Tranexamic Acid and conventional Hydroquinone on melasma[J].J Cosmet Dermatol,2015,14(3):174-177.
[20]Kim E H,Kim Y C,Lee E S,et al.The vascular characteristics of melasma[J].J Dermatol Sci,2007,46(2):111-116.
[21]Noh T K,Choi S J,Chung B Y,et al.Inflammatory features of melasma lesions in Asian skin[J].J Dermatol,2014,41(9):788-794.
[22]Rodríguez A A,Torres á B,Cortés G D,et al.CD4,IL-17,and COX-2 are associated with subclinical inflammation in malar melasma[J].Am J Dermatopath,2015,37(10):761-766.
[23]Lee D J,Lee J,Ha J,et al.Defective barrier function in melasma skin[J].J EUR Acad Dermatol,2012,26(12):1533-1537.
[24]Rajanala S,Maymone M B C,VASHI N A.Melasma pathogenesis: a review of the latest research, pathological findings,and investigational therapies[J].Dermatol Online J,2019,25(10):13030.
[25]Pomerantz H,Christman M P,Bloom B S,et al.Dynamic optical coherence tomography of cutaneous blood vessels in melasma and vessel response to oral tranexamic acid [J].Lasers Surg Med,2021,53(6):861-864.
[26]Na S Y,Cho S,Lee J H.Better clinical results with long term benefits in melasma patients[J].J Dermatol Treat,2013,24(2):112-118.
[27]Hassan A M,Elfar N N,Rizk O M,et al.Pulsed dye laser versus intense pulsed light in melasma: a split-face comparative study[J].J Dermatol Treat,2018,29(7):725-732.
[28]Li Y H,Chen J Z,Wei H C,et al.Efficacy and safety of intense pulsed light in treatment of melasma in Chinese patients[J].Dermatol Surg,2008,34(5):693-700.
[29]Liu Y,Wu S,Wu H,et al.Comparison of the efficacy of melasma treatments: a network meta-analysis of randomized controlled trials[J].Front Med,2021,29(8):713554.
[30]Maeda K,Tomita Y.Mechanism of the inhibitory effect of tranexamic acid on melanogenesis in cultured human melanocytes in the presence of keratinocyte-conditioned medium[J].J Health Sci,2007,53(4):389-396.
[31]Li D,Shi Y,LI M,et al.Tranexamic acid can treat ultraviolet radiation-induced pigmentation in guinea pigs[J].Eur J Dermatol,2010,20(3):289-292.
[32]Perper M,Eber A E,Fayne R,et al.Tranexamic acid in the treatment of melasma: a review of the literature[J].Am J Clin Dermatol,2017,18(3):73-81.
[33]Na J I,Choi S Y,Yang S H,et al.Effect of tranexamic acid on melasma: a clinical trial with histological evaluation[J].J Eur Acad Dermatol,2013,27(8):1035-1039.
[34]Wang Q,Liang Y Y,LI K W,et al.Herba Siegesbeckiae: A review on its traditional uses, chemical constituents, pharmacological activities and clinical studies[J].J Ethnopharmacol,2021,15(7):275:114117.
[35]Guo H,Zhang Y,Cheng B C,et al.Comparison of the chemical profiles and inflammatory mediator-inhibitory effects of three Siegesbeckia herbs used as Herba Siegesbeckiae (Xixiancao)[J].BMC Complement Med,2018,18(1):141.
[收稿日期]2022-7-21
本文引用格式:王雅玲,毛夢平,施为,等.外用3%氨甲环酸精华液治疗黄褐斑的前瞻性研究[J].中国美容医学,2023,32(5):6-9.