Efficacy of acupuncture therapy for post-stroke fatigue: a systematic review and Meta-analysis
2023-02-15YOUJianyuLIHaiyanXIEDingyiCHENMingrenCHENRixin
YOU Jianyu,LI Haiyan,XIE Dingyi,CHEN Mingren,CHEN Rixin
YOU Jianyu,School of Clinical Medicine,Jiangxi University of Chinese Medicine,Nanchang 330004,China
LI Haiyan,CHEN Mingren,Acupuncture and Tuina School,Jiangxi
University of Chinese Medicine,Nanchang 330004,China
XIE Dingyi,CHEN Rixin,Department of Acupuncture and Moxibustion,the Affiliated Hospital of Jiangxi University of Chinese Medicine,Nanchang 330006,China
Abstract OBJECTIVE: To assess the effectiveness and safety of acupuncture for post-stroke fatigue (PSF).METHODS: Eight online databases were searched to collect relevant trials of acupuncture for PSF published before April 2021.Meta-analysis was performed by using RevMan 5.4 software.The Grading of Recommendations,Assessment,Development and Evaluation system was used to assess the certainty of evidence.RESULTS: Four randomized controlled trials involving 289 PSF patients were identified and included in the systematic review.The results of the Meta-analysis revealed that acupuncture group was significantly better than routine treatment group in improving the effective rate [risk ratio (RR)=1.15,95%CI (1.01,1.33),P=0.04],reducing the FSS score [mean difference (MD)=-4.71,95% CI (-6.22,-3.20),P < 0.000 01] and FMA score[MD =15.60,95% CI (11.96,19.23), P < 0.000 01].Side effects of acupuncture were mild and rarely reported.The certainty of evidence of the outcomes based on the four trials was assessed as low.CONCLUSIONS: The existing evidence suggestsacupuncture as an adjunct to routine treatment may benefit in managing fatigue in stroke patients.However,high-quality RCTs are needed to further confirm these findings.
Keywords: acupuncture;stroke;fatigue;systematic review;Meta-analysis
1.INTRODUCTION
Post-stroke fatigue (PSF) is one of the most serious sequelae of stroke.It is characterized by fatigue and a lack of energy feeling physically and mentally,and this condition cannot be relieved by rest.1According to statistics,the prevalence of PSF in stroke survivors ranges from 25% to 85%.2Persistent fatigue symptoms may limit the rehabilitation process and have a negative impact on the patient's mental health and quality of life.3,4Fatigue can also increase the disability rate and even mortality of patients.5In addition,a recent Meta-analysis showed that the fatigue of stroke survivors increased over time.6Therefore,early detection and treatment of fatigue may have a positive impact on stroke recovery.At present,the pathogenesis of PSF is still unclear,and its fatigue is thought to be related to biological,psychosocial and behavioral factors.7Since PSF may be related to a variety of causative factors,there are many potential pharmacological intervention options,such as antidepressants and conscious stimulants.8,9However,recent studies have shown that there is insufficient evidence to support the effectiveness of pharmacological treatments and the overall effect of drugs is far from satisfactory.9-11Therefore,some researchers have begun to turn their attention to non-pharmacological interventions.12
Acupuncture,as one of the oldest non-pharmacological therapy,involves inserting thin needles into specific acupoints at a specific angle to treat diseases.13In China,acupuncture has been widely used in the management of stroke and related symptoms for a long time,and it has gradually been recognized worldwide.14,15In addition,acupuncture has been recommended by the World Health Organization (WHO) as a complementary and alternative treatment for stroke management.16In many published clinical trials on the treatment of PSF with acupuncture,most studies have shown that acupuncture is a beneficial intervention for PSF,and safety issues rarely occur.17However,no systematic review has been conducted to collect evidence on the efficacy of acupuncture for PSF.Therefore,the current study was conducted to evaluate the effectiveness and safety of using acupuncture to manage PSF.
2.METHODS
The protocol for this study was registered in the PROSPERO (https://www.crd.york.ac.uk/PROSPERO/;registration number CRD42020197221).
2.1.Study identification
The following databases were searched from their inception to April 2021: Embase,PubMed,Web of Science,Cochrane Library,WanFang,China National Knowledge Infrastructure Database,China Science and Technology Journal Database and the Chinese SinoMed Database.The database search was carried out using a combination of MeSH terms and free words,and the search terms include disease name (post-stroke fatigue)and intervention method (acupuncture).References of all included trials were also scanned to identify additional eligible trials.The detailed search strategies in each database are shown in Appendix 1.
2.2.Inclusion/exclusion criteria
We used the following items as eligibility criteria: (a)RCTs assessing acupuncture for PSF were included;(b)participants need to meet the diagnosis of stroke and fatigue at the same time,and there were no restrictions on the pathological types of stroke,including hemorrhagic stroke,ischemic stroke or mixed stroke;(c)in addition to the routine treatment of stroke (including western medicine basic treatment and rehabilitation treatment),the intervention of experimental group only included acupuncture,and the acupuncture here only includes manual acupuncture and electro-acupuncture,regardless of different acupoints or treatment duration;(d)in addition to the routine treatment of stroke,studies that employed sham acupuncture,no treatment or medicine as control group intervention were considered eligible;(e)the included trials measured at least one of the following indicators: clinical efficacy (Proportion of patients with improved fatigue symptoms),Fatigue Severity Scale(FSS),Fugl-Meyer Assessment (FMA),and adverse events.Exclusion criteria: (f) Non-RCTs;(g) duplicates;(h) literature reviews;(i) animal experiments.
2.3. Study selection and data extraction
We input all retrieved articles into EndNote 9 software and use the software to eliminate duplicate records.Two investigators independently screened eligible studies by browsing the title,abstract and full text,and extracted relevant data from the included trials,including the study author,publication date,sample size,mean age,intervention,acupuncture session,acupoints,outcomes and adverse events.If there is a difference in study selection or data extraction process,a third investigator would be asked to judge.
2.4.Study quality assessment
Two investigators independently assessed the quality of the included studies by using the Cochrane Risk of Bias tool version 2 (ROB 2.0),which included the following domains: (a) randomization process;(b) deviations from intended interventions;(c) missing outcome data;(d)measurement of the outcome;(e) selection of the reported result.18Discrepancies were resolved through negotiation.
2.5.Data synthesis and analysis
Meta-analysis was performed using Review Manager 5.4.Risk ratio (RR) was used to measure dichotomous variables,and mean difference (MD) or standardized mean difference (SMD) was used to measure continuous variables.When results were measured on the same scale,the outcomes were reported asMD;otherwise,the results were reported asSMD.Heterogeneity was evaluated byI2value and χ2test.WhenI2≤ 50% andP≥ 0.10,the fixed effect model was used;Otherwise,the random effects model was used to make a more conservative assessment of the intervention effect,and sensitivity analysis was performed to explore the robustness of the results.If the number of included trials was insufficient (fewer than 10 studies),we did not assess publication bias.
2.6.Certainty of evidence
The GRADE system was adopted to assess the certainty of evidence for the results,and each outcome indicator was divided into four categories: high,medium,low,and very low.19
3.RESULTS
3.1.Literature search
A total of 199 studies were found after primary search.It remained 143 studies after we excluded 56 duplicates.Then,after reading the title,abstract and full text,139 studies were eliminated.Finally,4 RCTs20-23were included in this systematic review.The process of eligible RCT selection is presented in Figure 1.
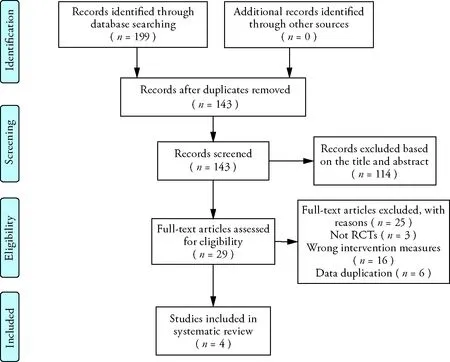
Figure 1 Study selection process
3.2.Study characteristics
We included a total of 4 trials from different research teams.Among them,the outcome indicators of one study21were derived from two RCTs.21,24Because these two RCTs were based on the same study,we integrated the outcome evaluation indicators of the two RCTs into the same one.A total of 289 PSF patients were involved in these four studies (145 in the acupuncture group,and 144 in the control group).All studies were conducted in China and published in Chinese.The sample sizes of the 4 RCTs ranged from 60 to 99.Characteristics of included 4 RCTs were summarized in Table 1.
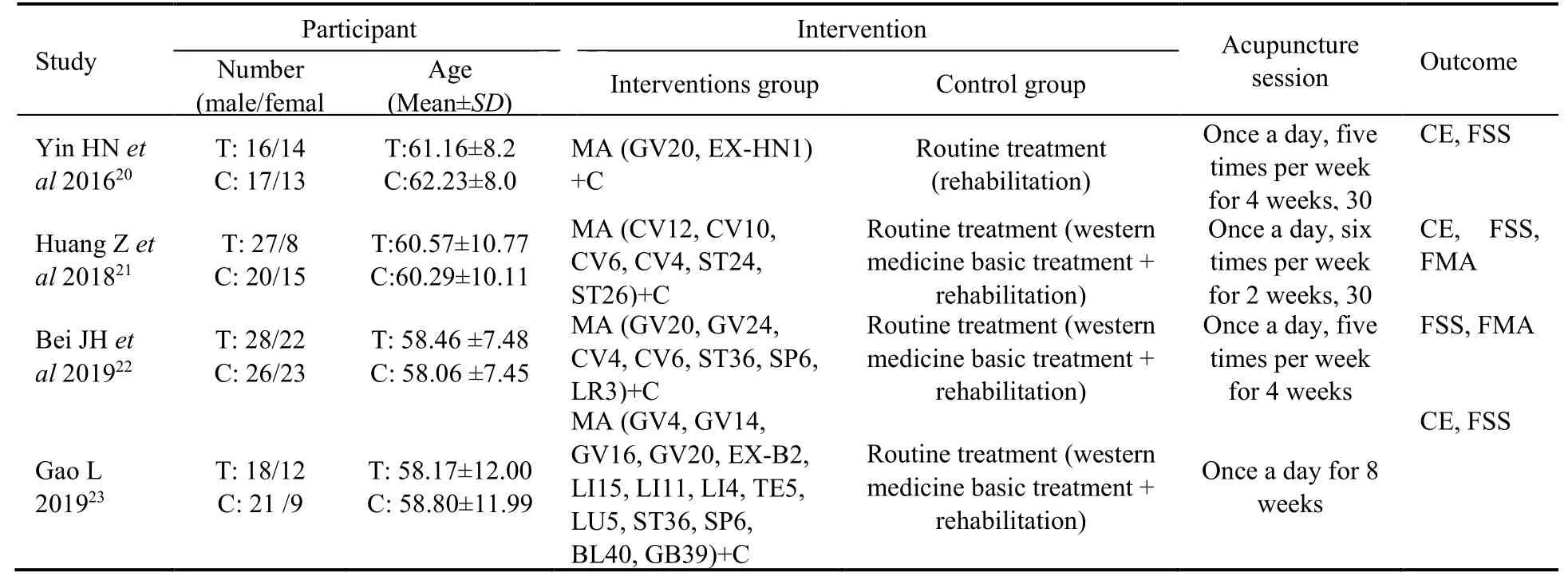
Table1 Characteristics of included studies
3.3.Risk of bias
The ROB assessment is shown in Figure 2.Although all studies used random number tables for random grouping,none of the studies mentioned the specific details of allocation concealment.In addition,due to the nature of acupuncture manipulations,blinding to participants is not suitable for acupuncture therapy.This makes all included studies have a certain risk of bias.
3.4.Efficacy and safety of acupuncture
3.4.1.Clinical efficacy
Three trials evaluated the effective rate of acupuncture for PSF.No heterogeneity was noted (P=0.72,I2=0%),and the fixed-effects model demonstrated that acupuncture group was significantly higher than the routine treatment group [RR=1.15,95%CI(1.01,1.33),P=0.04] in improving effective rate (Figure 3A).
3.4.2.FSS
Four trials assessed the severity of fatigue in stroke patients by using the FSS scores.The four RCTs showed no heterogeneity (P=0.53,I2=0%),and the fixedeffects model revealed that acupuncture group could further improve fatigue symptoms compared with the routine treatment group [MD=-4.71,95%CI(-6.22,-3.20),P< 0.000 01] (Figure 3B).
3.4.3.FMA
Two trials evaluated the recovery of motor function by using the FMA score.Analysis of data from FMA showed low heterogeneity (P=0.27,I2=18%),and the fixed-effects model showed that acupuncture group could further improve motor function compared with the routine treatment group [MD=15.60,95%CI(11.96,19.23),P< 0.000 01] (Figure 3C).
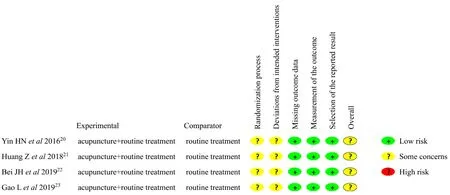
Figure 2 Risk of bias assessment
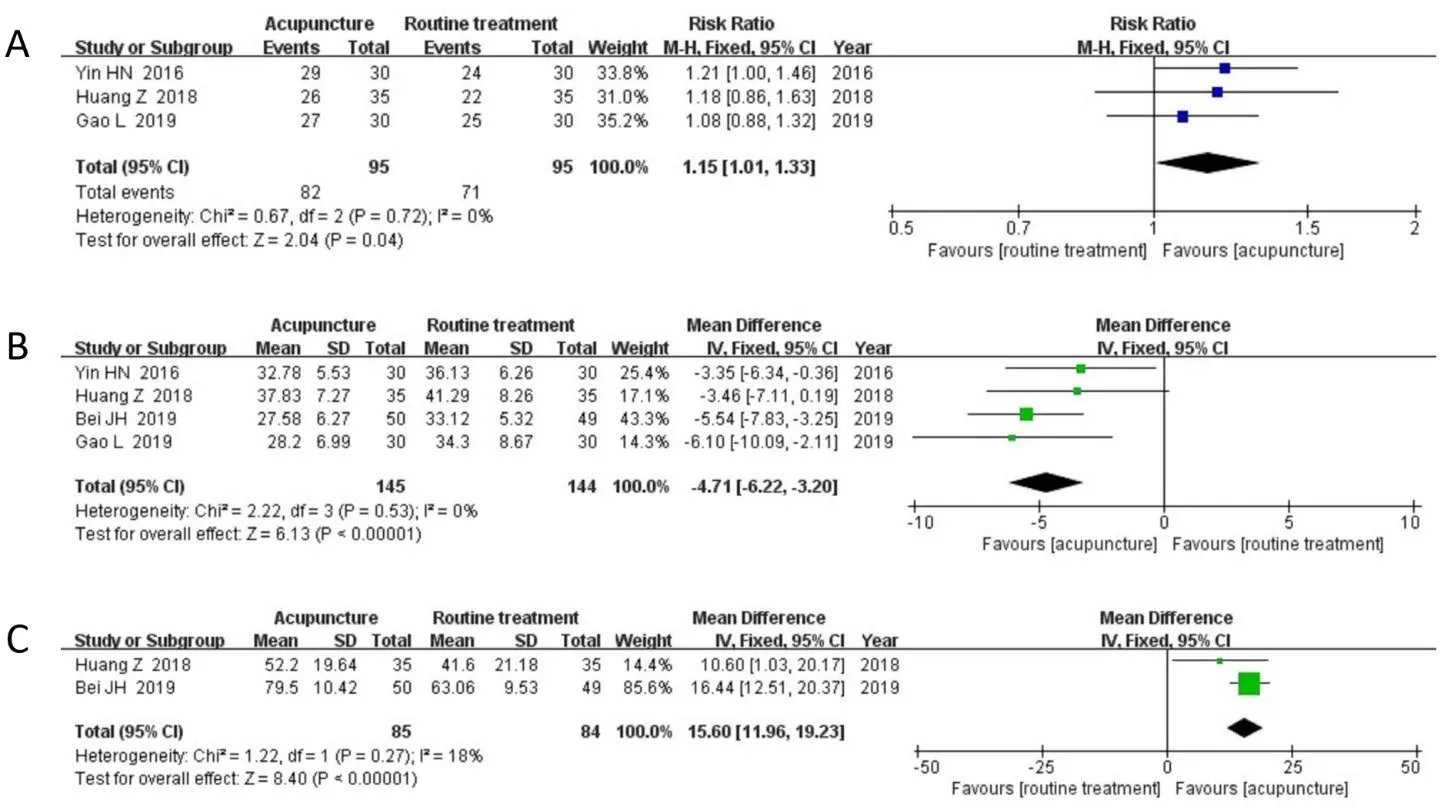
Figure 3 Meta-analysis results of the efficacy of acupuncture versus control group
3.4.4.Safety assessment
Two RCTs21,23reported the safety of acupuncture.One study23reported that 3 cases in the acupuncture group experienced subcutaneous hemorrhage,which disappeared after treatment.And one study21reported no adverse effects related to acupuncture.
3.5.Acupuncture point
A total of 23 acupoints were involved in the included 4 trials.Among them,Baihui (GV20) has the highest frequency of use.A total of 3 studies have selected this acupoint.The top five acupoints used in frequency were Baihui (GV20),Qihai (CV6),Guanyuan (CV4),Zusanli(ST36),Sanyinjiao (SP6).
3.6.Publication bias
Since the number of RCTs included in this study was only four (fewer than 10 studies),we did not perform a publication bias analysis.
3.7.Certainty of evidence
In general,all results were ranked as having low-quality evidence.The main reason for the decline in the certainty of evidence may be related to the poor methodological quality of the included studies and the small sample size.Table 2 presents the results of the GRADE analysis.
4.DISCUSSION
Stroke is a major cause of mortality and disability worldwide3.Due to the aging population,stroke has become an increasingly serious health concern.At the same time,those who survive a stroke often suffer from residual functional disabilities,cognitive deficits and emotional problems.Among them,fatigue is one of the most common complaints after stroke,and the management and prevention of PSF has been listed as one of the ten research priorities related to life after stroke.25-27Although the prevalence of fatigue in stroke patients is high,the pathophysiology of fatigue is poorly understood,and there is almost no evidence-based therapy to relieve fatigue.9Acupuncture has been used to treat stroke and its sequelae for centuries in China,and it has the advantages of reliable efficacy,easy operation,and safety.14Although the pathogenesis of PSF is still unclear,and PSF is also considered to be a multifactorial disease with complex etiology,28the clinical and basic research on acupuncture treatment of stroke and its sequelae have confirmed the efficacy of acupuncture.Acupuncture can promote the repair of the injured nervous system,reduce inflammation,increase cerebral blood flow,and regulate oxidative stress to improve stroke-related symptoms.14,29-31In addition,several recent Meta-analysis have also confirmed the antifatigue effect of acupuncture,32-34which may be related to the effect of acupuncture in regulating perturbed energy Metabolism,choline Metabolism,attenuating reactive oxygen species induced stress and downregulating the levels of related inflammatory factors(CPR,IL-6,TNF-α,IFN-γ,sTNF-R1).35-38Therefore,acupuncture is regarded as a promising intervention method for PSF.
In this systematic review,although the acupoint plans used by these 4 RCTs were different,some acupoints were still used very frequently.The five most popular acupoints were Baihui (GV20),Qihai (CV6),Guanyuan(CV4),Zusanli (ST36),Sanyinjiao (SP6).According to the theory of traditional Chinese medicine (TCM),we found that the above-mentioned acupoints have the properties of replenishingQiand activating blood,regulatingQi,and awakening the brain.39At the same time,TCM theory believes that the main cause of PSF is related to the deficiency ofQiand blood and poor circulation ofQiand blood.40,41Therefore,the therapeutic effects of the above 5 acupoints are beneficial to improve the fatigue symptoms of stroke patients.
To date,there is no systematic review focusing on acupuncture for PSF,and this is the first Meta-analysis to evaluate the efficacy of acupuncture for PSF.In this study,we included 4 eligible trials with a total of 289 PSF participants in this review.Compared with routine treatment,acupuncture combined with routine treatment has shown potential benefits in improving FSS,FMA and clinical efficacy.In addition,in terms of safety,one study reported no adverse events,and only one study reported subcutaneous hemorrhage after acupuncture treatment,but the symptoms were mild.Therefore,based on the findings of this review,we suggest that acupuncture might be an effective and safe adjuvant therapy for PSF.However,the GRADE system has rated the existing evidence as “low”.This weakens the reliability and influence of the evidence.Therefore,it is necessary to further explore the efficacy of acupuncture for PSF.
There were some limitations exist in the current study.Firstly,we only searched the Chinese and English databases,which may miss some potential trials published in other languages that meet the inclusion criteria.In addition,the four trials included in this study were all conducted in China.Therefore,the evidence in this review may have regional limitations.Secondly,the methodological quality of the evidence in this study is not high.None of the included trials reported the implementation of allocation concealment.Moreover,due to the particularity of acupuncture,it is not feasible to implement a blind design.Thirdly,despite our extensive search,this study was still limited by the number of included trials and the small sample size,which may lead to inaccurate research evidence.
In conclusion,based on currently limited evidence,the results of our Meta-analysis show that acupuncture as an adjunct to routine treatment may benefit in managing PSF.However,the number of RCTs included in this study is limited and the methodological quality is suboptimal,which greatly weakens the reliability and influence of the evidence.Therefore,high-quality RCTs are still needed to confirm the benefits of acupuncture for PSF.

杂志排行

Journal of Traditional Chinese Medicine的其它文章
- Effects of the Huangkui capsule (黄葵胶囊) on chronic kidney disease: a systematic review and Meta-analysis
- Effectiveness of moxibustion alone on lumbar disc herniation: a Meta-analysis of randomized controlled trials
- Efficacy of luteolin on the human gastric cancer cell line MKN45 and underlying mechanism
- Tilianin extracted from Xiangqinglan (Herba Dracocephali Moldovicae) inhibits apoptosis induced by mitochondrial pathway and endoplasmic reticulum stress in H9c2 cells after oxygenglucose deprivation/reoxygenation
- Comparing the effects of three decoctions for coronavirus disease 2019 on severe acute respiratory syndrome coronavirus 2-related tolllike receptors-mediated inflammations
- Astragaloside IV ameliorates insulin induced insulin resistance in HepG2 cells through reactive oxygen species mediated c-Jun Nterminal kinase pathway