Advances in neovascularization after diabetic ischemia
2022-11-24YueCaiGuangYaoZangYanHuangZhenSunLiLiZhangYongJiangQianWeiYuanZhongQunWang
Yue Cai,Guang-Yao Zang,Yan Huang,Zhen Sun,Li-Li Zhang,Yong-Jiang Qian,Wei Yuan,Zhong-Qun Wang
Yue Cai,Guang-Yao Zang,Zhen Sun,Li-Li Zhang,Yong-Jiang Qian,Wei Yuan,Zhong-Qun Wang,Department of Cardiology,Affiliated Hospital of Jiangsu University,Zhenjiang 212000,Jiangsu Province,China
Yan Huang,Department of Ophthalmology,Affiliated Hospital of Jiangsu University,Zhenjiang 212000,Jiangsu Province,China
Abstract With the high incidence of diabetes around the world,ischemic complications cause a serious influence on people’s production and living.Neovascularization plays a significant role in its development.Therefore,neovascularization after diabetic ischemia has aroused attention and has become a hot spot in recent years.Neovascularization is divided into angiogenesis represented by atherosclerosis and arteriogenesis characterized by coronary collateral circulation.When mononuclear macrophages successively migrate to the ischemia anoxic zone after ischemia or hypoxia,they induce the secretion of cytokines,such as vascular endothelial growth factor and hypoxia-inducible factor,activate signaling pathways such as classic Wnt and phosphatidylinositol 3 kinase (PI3K)/protein kinase B (Akt) pathways,trigger oxidative stress response,activate endothelial progenitor cells or enter the glycolysis or lactic acid process and promote the formation of new blood vessels,remodeling them into mature blood vessels and restoring blood supply.However,the hypoglycemic condition has different impacts on neovascularization.Consequently,this review aimed to introduce the mechanisms of neovascularization after diabetic ischemia,increase our understanding of diabetic ischemic complications and their therapies and provide more treatment options for clinical practice and effectively relieve patients’ pain.It is believed that in the near future,neovascularization will bring more benefits and hope to patients with diabetes.
Key Words: Diabetes mellitus;Angiogenesis;Arteriogenesis;Ischemia;Hypoxia
INTRODUCTION
Diabetes mellitus is a complex,heterogeneous,whole-body chronic metabolic disease;it is predicted that by 2045,the number of patients with diabetes,aged 20-79 years,will increase to 783 million[1].Diabetes-related complications include microvascular plaque formation,ischemia and hypoxia caused by atherosclerosis.They are characterized by severe arterial ischemia,increased risk of amputation of peripheral artery disease and so on.Promoting neovascularization to restore the blood flow of the ischemic area is conducive to disease outcomes while avoiding risk.Hence,it is an urgent issue for scientific researchers.
NEOVASCULARIZATION AFTER ISCHEMIA
Neovascularization is caused by angiogenesis and arteriogenesis.Angiogenesis refers to the budding of new blood vessels in the vascular bed in an original way to form new vasculature,mainly in the capillaries[2].Arteriogenesis is the formation of new arteries by expanding lumen diameter and remodeling tube walls to restore blood flow in the ischemic area.The new route gradually disappears when the previously blocked artery is recanalized[3].
Angiogenesis
Physiological angiogenesis mainly occurs in embryo development,endometrial thickening and wound healing;the process depends on the ratio of proangiogenic factors to antiangiogenic factors.Pathological angiogenesis is often triggered in disease states,such as atherosclerosis,tumors,systemic lupus erythematosus,etc[4],to form abnormal blood vessels with thinner walls and higher permeability.Angiogenesis includes the following steps: (1) Endothelial cells sprout under the action of angiogenic factors[5];(2) Pericytes aggregate if their absence leads to increased lumen permeability[6] and vascular instability;and (3) The basement membrane is reconstructed to develop mature and stable blood vessels.
Atherosclerosis can lead to severe complications such as myocardial infarction (MI),resulting in heart failure.Endothelial cells,which sprout under the action of angiogenic factors,significantly improve the patient’s recovery,which is the focus of current research.
After MI,blood congestion,thromboembolism and compression of the surrounding tissue,proinflammatory factors are released,leading to impaired endothelial integrity,loss of myocardial cells,endothelial cell damage,increased capillary permeability and secretion of proinflammatory cytokines to activate white blood cells and endothelial cells.This results in the release of a large number of inflammatory factors into the infarcted myocardium,thus promoting myocardial inflammation[7].The formation of neovascularization in the ischemic infarct area to provide nutrients and oxygen is the key to post-MI repair.Neovascularization in the surrounding area of infarction increases vascular density and extends to the core area of infarction[8],and hypoxia plays an essential role in this process.
The most studied factor is hypoxia-inducible factor-1α (HIF-1α),whose reduced protein expression under high glucose conditions leads to increased MI[9].In anoxic environments,the HIF-1α/vascular endothelial growth factor (VEGF) pathway acts by releasing angiogenic factors.After MI,reactive oxygen species (ROS) in cardiac fibroblasts increase by about 50%,resulting in mutations in the HIF phenotype marked by scar contraction and dysfunction[10].HIF activation induces VEGF release,which activates endothelial cells (ECs) through the paracrine mechanism,and can be expressed in ECs to participate in angiogenesis.In addition,angiopoietin-like protein 4 stabilizes VEGF receptor 2/Ca2+-dependent cell adhesion molecule 5 complex to maintain endothelial structural integrity and promote macrophage transformation into a repair phenotype to enhance boundary region angiogenesis.
Arteriogenesis
Arteriogenesis refers to the growth of new arteries or the derived collateral vessels,mainly involved in the active proliferation of ECs and smooth muscle cells,resulting in lumen enlargement and wall remodeling.It comprises primarily two stages[3].In the early stage,the diameter of lateral branches and tube walls increases under the influence of fluid shear stress.Subsequently,monocytes promote lumen remodeling by secreting metalloproteinases and cytokines.In addition,M1-type macrophages promote the progression of myocardial inflammation[11].The release of inflammatory factors under ischemia and hypoxia promotes the progression of inflammation and the occurrence of glycolysis.Under this action,fibroblasts are transformed into ECs,triggering epigenetic modification.ECs and fibroblasts contribute to the formation of arteries[12-14].
Human coronary circulation has an extensive anastomotic network.Even one-third of ordinary people have collateral circulation to cope with MI caused by transient vascular occlusion[15].Further,20%-25% of patients with coronary artery disease can prevent MI,improve survival and reduce mortality by promoting normal blood flow through collateral circulation during coronary artery occlusion.Approximately 1 in 5 patients cannot tolerate percutaneous coronary intervention or coronary artery bypass grafting.Therefore,collateral growth promotion is a promising therapeutic strategy targeting arteriogenesis.In the absence of coronary artery disease,these arteries are only 100-200 µm in diameter,and the lumen is impassable.When coronary artery disease causes a major artery occlusion,the collateral arteries are remodeled and the lumen is expanded to 100-800 µm in diameter to serve as part of the major artery[16],which is in line with normal routes and has one to two layers of smooth muscle cells.At the same time,the expansion of the diameter of the tube is accompanied by a decrease in the number of collateral arteries.The myocardial protection of large blood flow is more significant in the collateral arteries than in the new capillaries surrounding the infarct area[17].
Although collateral maturation is essential for preserving cardiac function,the related markers are still lacking[18].Although the influence of coronary artery collateral formation and prognosis has been controversial at present[19],some studies showed[20] that patients with MI having coronary collateral circulation have more severe stenosis and worse cardiac function.Therefore,from a macro point of view,it is believed that collateral circulation benefits at least one-fifth of patients who cannot undergo percutaneous coronary intervention and coronary artery bypass grafting.Physiological or pathological vascular reconstruction and blood flow redistribution can prevent excessive MI and reduce injury to the body.This therapeutic strategy has broad research prospects and is worth further exploration to benefit patients.
Impact factors
As mentioned earlier,neovascularization is affected by various proangiogenic/antiangiogenic factors.The mechanisms and roles of proangiogenic factors,such as HIF,macrophages,VEGF family,noncoding RNA and hepatocyte growth factor,and antiangiogenic factors,such as thrombospondin-1 and interleukin 12 (IL-12),summarized in this study (Tables 1 and 2)[7,21-44].
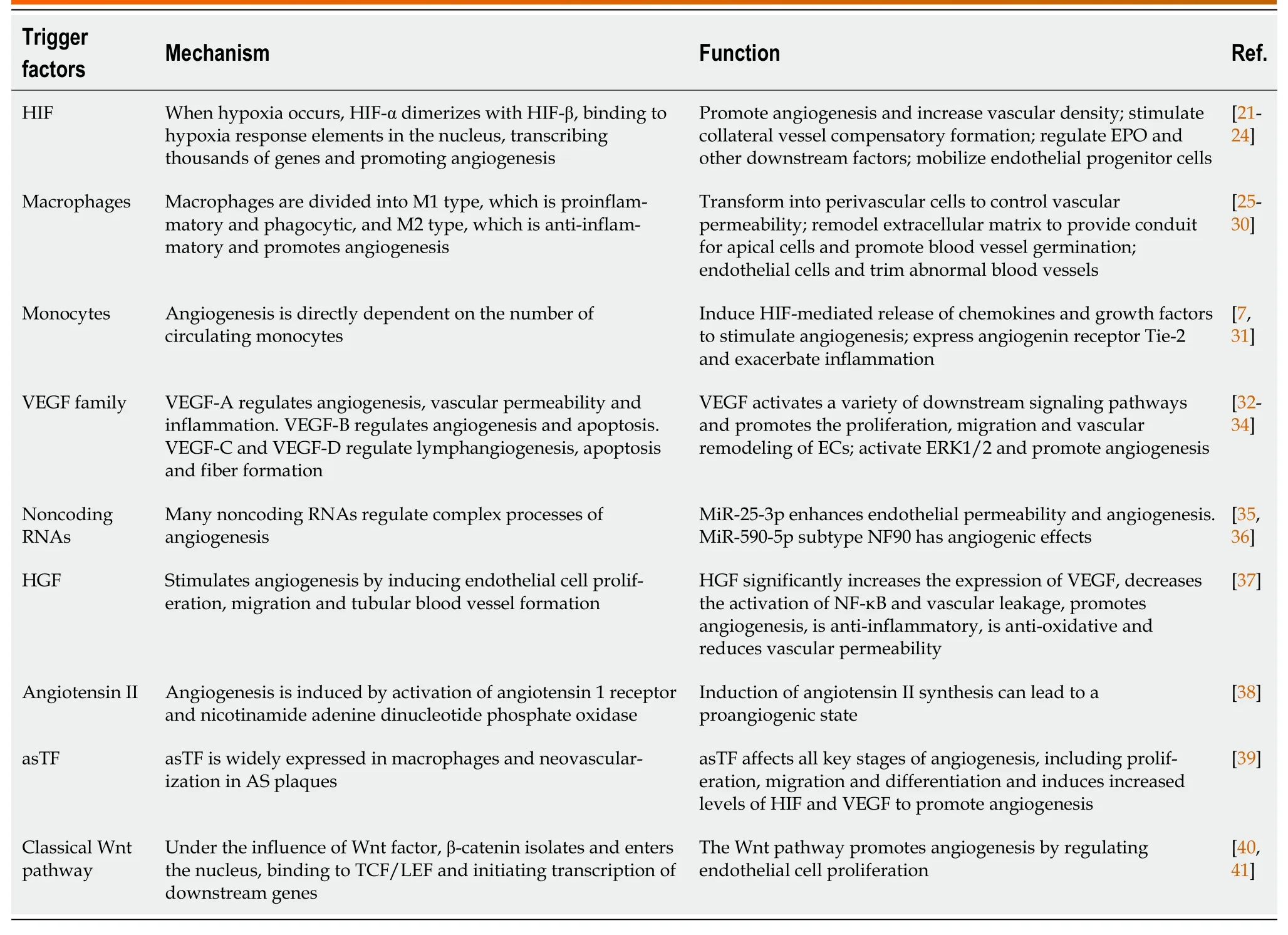
Table 1 Mechanisms and functions of proangiogenic factors
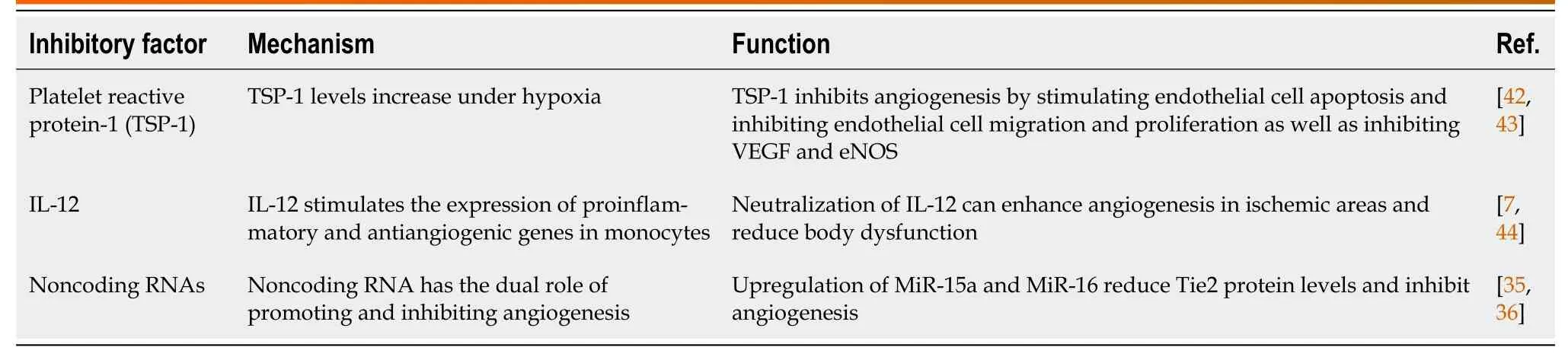
Table 2 Mechanisms and functions of the antiangiogenic factors
MECHANISMS OF NEOVASCULARIZATION AFTER DIABETIC ISCHEMIA
Glycolysis
Studies have shown that 80% of ATP in ECs is produced by glycolysis[45],mainly due to the limited number of mitochondria.The energy generated needs to be supplied to the distal tissues.In addition,the ATP generation by glycolysis is faster than that by oxidative phosphorylation.Therefore,glycolysis is the primary energy supply for ECs in normal and hypoxic states.Hypoxia or lack of nutrition can promote the production of VEGF,fibroblast growth factor and other angiogenic factors[46],the concentration and the activity of hexokinase and membrane expression of glucose transporter protein 1.The ECs differentiate into specific cells under high VEGF levels,forming platelet pseudopodia and filiform pseudopodia,promoting migration and stem cell proliferation.Stable glycolysis produces lactic acid[47],promoting VEGF expression and inducing angiogenesis under multiple effects.
6-phosphofructo-2-kinase/fructose-2,6-biphosphatase 3 (PFKFB3) transcription through HIF-1α is induced by hypoxia,which is an essential regulator of glycolysis and can be phosphorylated by activating kinases such as mitogen-activated protein kinase[48].PFKFB3 can promote the synthesis of fructose-2 6-diphosphate,activate phosphofructokinase 1 and promote glycolysis.The Notch-Delta-like ligand 4 signaling pathway can promote stem cell extension,tip cell growth and blood vessel germination[49].
Some intermediate products of glycolysis enter the pentose phosphate pathway.The NADPH produced during this process is necessary for nitric oxide (NO) biosynthesis,promoting angiogenesis.When macrophage metabolism shifts to glycolysis,M1 proinflammatory macrophages facilitate glycolysis,interrupting the tricarboxylic acid cycle and producing lactic acid rather than metabolizing pyruvate to acetyl-CoA.Anti-inflammatory M2 macrophages inhibit the pentose phosphate pathway.
Lactylation
Lactic acid has long been considered as a metabolic waste.Recent studies have shown that lactic acid can be expressed as a signaling molecule in wound healing and angiogenesis[50].Lactic acid can modify histones to regulate macrophage polarity and expression of tissue repair genes such as arginase-1[51].In inflammatory diseases such as atherosclerosis,macrophages secrete proinflammatory cytokines such as tumor necrosis factor γ and interleukin 12 to cause extensive damage to surrounding tissue,and anaerobic glycolysis causes lactic acid accumulation[51].The macrophage polarity transition is a hallmark of the disease,and lactic acid converts macrophages from a proinflammatory phenotype into a repairing phenotype,removes cell debris and promotes wound healing.Inflammatory macrophages undergo modifications,which promote the repair characteristics of macrophages in response to inflammatory damage[52].In addition,lactic acid can covalently couple with various histone lysine residues during histone acetylation to promote the transcription of homeostasis-related genes.In the late stage of lactic acid and histone lactate modification and accumulation,the cells switch to a steady-state phenotype,in which inflammatory genes are difficult to induce.
Studies have shown that lactic acid can promote the secretion of VEGF,activate the nuclear factor kappa-B/C-X-C motif chemokine 8 pathway and stabilize HIF-1α,playing a role in promoting angiogenesis signaling molecules.The overall function of lactic acid is to transform the inflammatory phenotype of macrophages into a repair phenotype.We hypothesized that lactic acid was associated with angiogenesis.However,the integration mechanism of lactic acid and hypoxia,such as HIF,chromatin remodeling and other processes extending to angiogenesis,is still unclear and needs further research (Figure 1).
Oxidative stress
When the body is subjected to various diabetic stimuli,the mitochondria is stimulated to produce superoxide,leading to the formation of the powerful oxidant nitrite,which damages DNA and depletes intracellular NAD (+)[53],resulting in a pathological state.Two common mechanisms[54] contribute to increased oxidative stress[55] in diabetes: One is an increase in free radical production and the other is a decrease in the levels of protective endogenous antioxidants.Also,natural antioxidants include dandelion[56],saffron[57,58],hawthorn[59],vitamin C and vitamin E[60].However,rhizoma polygonate in traditional Chinese medicine can dephosphorylate DNA to damage DNA[61].In addition,hyperglycemia activates nuclear factor kappa-B,which can lead to changes in the inflammatory response,upregulation of COX-2,inducible NO synthase (NOS)[62],tumor necrosis factor α and interleukin 1,promotion of cell proliferation and inhibition of cell death.The increased expression of inducible NOS catalyzes the production of large amounts of NO[63].The inhibition of TLR2/4 signaling can avoid nuclear factor kappa-B translocation,ultimately reducing cell apoptosis[64].The hyperglycemic environment can stimulate the mitochondrial respiratory chain to produce a large number of oxygen free radicals,activate protein kinases C[65] and promote the NADPH-related processes of oxidative stress,leading to endothelial cell apoptosis.A small number of ROS can maintain normal physiological function[66];however,an excess of ROS causes oxidative stress[67],which can activate multiple stress kinases and related proteases and affect their activities[68],aggravate cytotoxicity and attack cells,leading to endothelial progenitor cell senescence,apoptosis and inhibition of migration and proliferation.Superoxide anions and H2O2in the ROS family play a major role in this process.In addition,the activity of endodermal NOS is reduced,the metabolism of tetrahydrobiopurine (BH4) is abnormal,and dihydrobiopterin (BH2) cannot be recovered in diabetes,resulting in a lower level of BH4[69].NOS induces the formation of many superoxide anions instead of NO,aggravating oxidative stress.Advanced glycation end products lead to an imbalance in ROS production and clearance and increased endothelial permeability[70].Oxidative stress impairs angiogenesis through multiple mechanisms.
Endothelial progenitor cells
Endothelial progenitor cells (EPCs) are fusiform cells with limited proliferative capacity in the early stage and cells with high proliferative capacity in the late stage[71].During tissue ischemia,EPCs can be mobilized from bone marrow to damaged blood vessels for vascular repair or angiogenesis,or the number of circulating EPCs increasesviavarious factors,including VEGF,stromal cell-derived factor-1 or stem cell factor.EPCs can proliferate,migrate,adhere and differentiate into ECs,repair damaged ECs and secrete angiogenic factors such as VEGF to promote angiogenesis in ischemic tissues[72].
In diabetes,endothelial dysfunction and delayed angiogenesis promote the occurrence and development of diabetic vascular complications.In the high glucose environment,the number of EPCs is reduced and their functions are impaired[73].In addition,EPCs are less responsive to ischemia,VEGF,stromal cell-derived factor-1 and other stimuli,and the mobilization mechanism is damaged.EPCs may also secrete antiangiogenic factors.The high glucose environment leads to the excessive production of ROS,excessive activation of NADPH oxidase and a significant decrease in the levels of manganese-containing superoxide dismutase and other antioxidant enzymes,resulting in EPC dysfunction[74].The excessive production of ROS significantly increases the levels of oxLDL,inhibits Akt phosphorylation and endothelial NOS (eNOS) expression,decreases NO activity,inhibits the PI3K/Akt/eNOS signaling pathway and induces the apoptosis of EPCs,migration of EPCs and formation of functional defects in the lumen[75].In addition,the severe inflammatory environment of diabetes causes impaired adhesion and proliferation of EPCs as well as neovascularization.
However,when patients with diabetes suffer from vascular complications,the number and function of EPCs in different parts (microvessels and large vessels) are different.For example,when such patients suffer from peripheral artery disease,the number of EPCs decreases.However,the proliferative capacity of EPCs is increased in patients with proliferative retinopathy.
Slit2/ Roundabout 1/PI3K/Akt/VEGF signaling pathways
Endothelial cell-derived Slit2 plays a proangiogenic role in EC migration and lumen formation through its Roundabout 1 (Robo1) receptor.High glucose levels directly induce Slit2 production or Slit2/Robo1 binding.Robo1 inhibits the activation of the PI3K/Akt pathways and HIF-1α/VEGF signaling pathways and inhibits angiogenesis.PI3K inhibitors also inhibit the HIF-1α/VEGF signaling pathway.Hence,Robo1 may be a potential therapeutic target in diabetic ischemic complications with abnormal angiogenesis,such as diabetic nephropathy and diabetic retinal disease[76].The interference of this signaling pathway can inhibit angiogenesis (Figure 2).
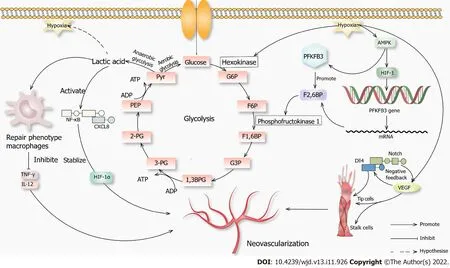
Figure 1 Novel mechanisms of neovascularization.When glucose enters the cell through channels that initiate glycolysis in an aerobic environment,when the anaerobic glycolysis,lactic acid can cause macrophages to convert to a repair phenotype.These macrophages will not produce inflammatory factors such as tumor necrosis factor γ and interleukin 12,which promotes angiogenesis.Lactic acid can activate the nuclear factor kappa-B-C-X-C motif chemokine 8 pathway,promote vascular endothelial growth factor (VEGF) secretion,stabilize hypoxia-inducible factor-1α (HIF-1α),and promote angiogenesis.When hypoxia occurs in the environment,it promotes hexokinase,which promotes glycolysis,and AMPK,which promotes hypoxia-inducible factor-1.It then acts on 6-phosphofructo-2-kinase/fructose-2,6-biphosphatase 3.AMPK also acts directly on 6-phosphofructo-2-kinase/fructose-2,6-biphosphatase 3,and they jointly promote fructose-2,6-biphosphatase,which acts on phosphofructokinase 1 and promotes glycolysis.Hypoxia also promotes VEGF secretion,and a high concentration of VEGF activates the Notch-DLL4 pathway,directly or indirectly promoting the proliferation of tip cells.VEGF also promotes the growth of stalk cells,and both promote angiogenesis.1,3BPG: 1,3 diphosphoglycerate;2-PG: 2-phosphoglycerate;3-PG: 3-phosphoglycerate;F1,6BP: Fructose 1,6-diphosphate;F2,6BP: Fructose 2,6-diphosphate;F6P: Fructose 6 phosphate;G3P: Glyceraldehyde-3-phosphate;G6P: Glucose 6-phosphate;PEP: Phosphoenolpyruvate;Pyr: Pyruvic acid.
NEOVASCULARIZATION AFTER DIABETIC ISCHEMIA
Diabetes atherosclerosis
Atherosclerotic plaques lead to local hypoxia and trigger angiogenesis of the outer membrane of the vessel.The newly formed vessels are immature and leaky due to the lack of a tight connection between the pericellular cells and ECs.Lipids,inflammatory factors and red blood cells invade the plaques,leading to vessel rupture within the plaques.Proteolytic enzymes released by neovascularization promote inflammatory cell infiltration,and inflammatory factors trigger angiogenesis[77].At the same time,intraplaque bleeding leads to a rapid increase in plaque volume,the fibrous cap changes to a contraction phenotype,and the fibrous cap becomes thinner[78],increasing the risk of plaque rupture[79].However,Brezinskiet al[80,81] put forward an opposite view that plaque rupture is caused by insufficient angiogenesis.The axial extension of neovascularization allows the healing of most plaques,while insufficient angiogenesis cannot sustain the growth of ECs in long necrotic plaques,resulting in plaque rupture and acute coronary syndrome.
Under high glucose conditions,the senescence and death of EPCs are accelerated,the PI3K/Akt/eNOS signaling pathway is inhibited,advanced glycation end products are increased,and fibrin formation is accelerated[82,83].This triggers endoplasmic reticulum stress and oxidative stress,resulting in insulin resistance and accelerated atheromatous plaque formation.The endothelial cell differentiation is blocked,and angiogenesis is damaged (Figure 3).
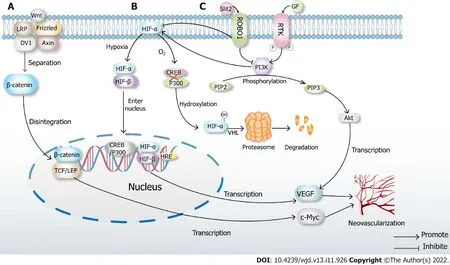
Figure 2 Classical mechanisms of neovascularization.A: Classical Wnt pathway.When there is no Wnt signal,LRP,Frizzled,DV1 and Axin are closely combined with β-catenin.In the presence of Wnt signaling,the complex disintegrates,and β-catenin enters the nucleus,binds to TCF/LEF,transcribes multiple downstream signals such as c-Myc and ultimately promotes neovascularization;B: Under normoxic conditions,hypoxia-inducible factor (HIF)-α inhibits the binding of cAMP-response element binding protein (CREB) and P300,which causes hydroxylation of HIF,then leads to proteasome degradation and inactivation after VHL ubiquitination.When hypoxia occurs,prolyl hydroxylase domains become inactive,allowing HIF-α to migrate to the nucleus,where it dimerizes with HIF-β.The dimer binds to the hypoxia response elements of specific genes in DNA,transcribes thousands of genes such as vascular endothelial growth factor (VEGF) and promotes neovascularization;C: High glucose induces Slit2/Roundabout 1 (Robo1) binding,and Robo1 inhibits the activation of phosphatidylinositol 3kinase (PI3K)/protein kinase B (Akt) and HIF-1α/VEGF signaling pathway and inhibits angiogenesis.PI3K inhibitors also inhibit the HIF-1α/VEGF signaling pathway.After activation of the PI3K/Akt signaling pathway,a variety of cytokines including VEGF will be transcribed to promote angiogenesis.
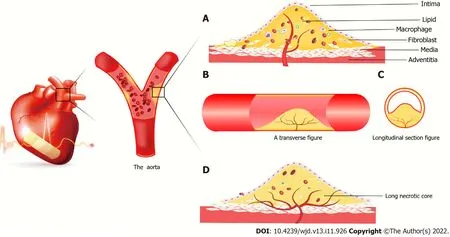
Figure 3 Atherosclerotic plaque forms in coronary vessels.A: New blood vessels from the outer membrane to the media and intima,macrophages and smooth muscle cells gobble up from the film in lipid foam cell formation.The red blood cells,cytokines,etc extend the blood vessels into the plaque.It is because the spin-off of new blood vessels leads to unstable plaques,plaque hemorrhage and rupture resulting in acute coronary syndrome;B: Axial slice of intravascular plaque and neovascularization grows axially in the plaque;C: Transverse view of intravascular plaque;D: It is believed that neovascularization grows in the axial direction in plaques.Due to insufficient growth of neovascularization,long necrotic plaques are ruptured due to ischemia and hypoxia in the plaque,resulting in acute coronary syndrome.
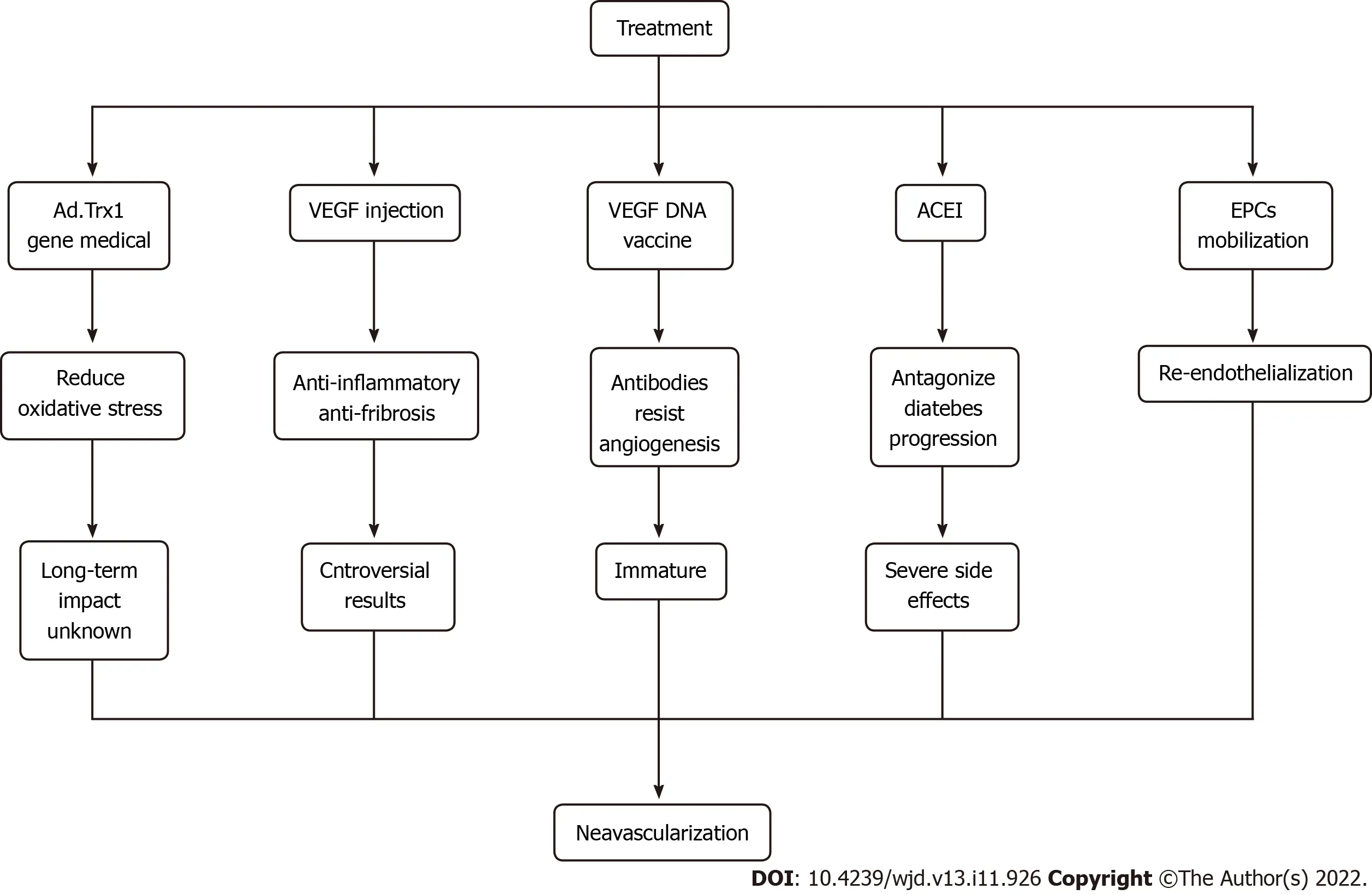
Figure 4 Cutting-edge approaches to therapeutic angiogenesis.ACEI: Angiotensin converting enzyme inhibitors;EPCs: Endothelial progenitor cells;VEGF: Vascular endothelial growth factor.
Diabetic retinopathy
Diabetic retinopathy (DR) can be divided into early nonproliferative DR and late proliferative DR in terms of progression,leading to pathological retinal angiogenesis[84].Neovascularization extends along the surface of the retina into the vitreous cavity.Still,such vessels are fragile and easily broken,easily leading to vitreous hemorrhage,retinal detachment or macular nonperfusion and related photoreceptor dysfunction[85].The earliest change is the thickening of the vascular basement membrane.In a high glucose environment,the basement membrane hardens and changes the elasticity of blood vessels,affecting the retinal blood flow and the dynamic balance between the inside and outside of blood vessels[86].
After the blood glucose level increases,the blood-retinal barrier degrades briefly in a few days or weeks,and then Muller cells are activated.Pericytes are lost in about 2 mo,followed by ECs,leading to vascular degeneration 6 mo after diabetes[85].Vascular degeneration is caused by the loss of pericytes that control vascular patency,resulting in decreased vascular patency,vascular blockage,endothelial cell fusion/degeneration and finally basal membrane dissolution,vascular degeneration and formation of capillaries without ECs.However,under physiological conditions,ECs of retinal capillaries express a high level of tight connections,limiting the circulation of nutrients,soluble factors and cells into tissues[87],and vascular degeneration destroys this structural function.
Consistent with numerous pathological processes,in a hypoxic and ischemic environment,angiogenesis-related factors are promoted,retinal neovascularization occurs,and newly formed blood capillaries migrate to other capillaries and merge to form new blood capillaries[87].However,the high glucose environment can promote the development of diabetic retinal neovascularization.Proliferative retinopathy is accompanied by tractional retinal detachment and vision loss.Therefore,the treatment aims to inhibit neovascularization.The standard treatment methods include laser therapy and anti-VEGF therapy.The intravitreal injection of VEGF inhibitors has excellent short-term safety.However,whether long-term anti-VEGF may have long-term adverse effects on the function of retinal neurons is unclear.
Diabetic nephropathy
In the early stage of diabetic nephropathy,hypoxia induces HIF generation,and endothelial growth factor or angiopoietin maintains renal vascular density,resulting in increased abnormal angiogenesis,vascular immaturity,plasma protein leakage,increased proteinuria and significantly increased glomerular filtration rate.In the late stage,glomerular capillaries are sparse,and the production of nephrogenic erythropoietin is increased,which aggravates renal hypoxia,and glomerular cells lose vitality[88].In this process,eNOS activity declines,the utilization rate of NO decreases,oxidative stress abates HIF activation,and VEGF expression is significantly lowered.Also,the levels of antiangiogenetic factors such as platelet response protein 1 and endothelial inhibition significantly increase,the levels of inflammatory cytokines increase,and VEGF expression is inhibited.Further,EPC function is impaired,the inflammatory response is enhanced,and the expression of adherence factors is upregulated,which is accompanied by impaired capillary ECs,endothelial barrier dysfunction and reduced angiogenesis,resulting in abnormal angiogenesis and vascular leakage.Podocytes are an important source of growth factors that regulate endothelial cell proliferation and angiogenesis.Their number increases in the early stage of diabetes and decreases in the late stage.The number of mesangial cells increases,the capillary basement membrane thickens,and the capillary number and area increase,directly or indirectly resulting in glomerular hyperplasia and mesangial expansion.
At present,no precise treatment is available for diabetic nephropathy to inhibit angiogenesis.VEGFA inhibitors can be used,but their levels need to be maintained at an appropriate levelin vivo[89].A deviation from moderate levels can cause damage.
Diabetic foot ulcer
Diabetic foot ulcer (DFU) is characterized by neuropathy caused by hyperglycemic levels,arterial stenosis caused by lipid deposition,and ischemic lesions of lower extremities.The DFU healing process can be divided into three overlapping phases: early steady-state and inflammation,arteriogenesis and matrix deposition;mid-late reshaping;and epithelial cell remodeling[90].Neutrophil granulocyte and macrophages produce cytokines and promote cell proliferation;fibroblasts are rich in collagen fibers and induce angiogenesis and vascularization[91].Neurological and ischemic lesions lead to impaired healing.
DFU arteriogenesis is reduced in diabetes.Hypoxia and ROS decrease transcriptional activities of HIF,VEGF,angiopoietin 2 and fibroblast growth factor and inhibit collateral development and arteriogenesis after limb ischemia[92].Hyperglycemic levels result in impaired growth factor production and macrophage function,collagen accumulation inhibition and poor migration and proliferation of keratinocytes and fibroblasts,leading to impaired angiogenesis[91].At the same time,wound infection reduces the active matrix metalloproteinase 8 (MMP-8) level,increases the active MMP-9 level,inhibits laminin,enhances keratinocyte migration,reduces arteriogenesis and slows wound healing[93].
For the treatment of DFU,the current strategy is to increase arteriogenesis,eliminate oxidative stress and ulcer infection[94].The best strategy for DFU treatment is to inhibit MMP-9 without affecting MMP-8,which can reduce inflammation and increase arteriogenesis.Applying prolyl hydroxylase domain inhibitors with clinical potential can stabilize HIF and increase its activity to promote arteriogenesis.Mesenchymal stem cells produce growth hormones that drive arteriogenesis and re-epithelialization.
TREATMENT
For treating diabetic ischemic neovascularization,the most crucial way is to control blood glucose levels.On this basis,various therapeutic methods,including gene therapy and vaccine research,have been proposed,which have broad prospects.For example,Ad.trx1 gene therapy can stabilize the microenvironment in the myocardium,reduce oxidative stress and cell death and induce neovascularization and maturation.This is a novel treatment that may improve disease progression and patient recovery[95].Injection of VEGF and hepatocyte growth factor can promote neovascularization and exert anti-inflammatory and anti-fibrotic effects,but gene therapy is still controversial due to its insignificant effect and needs further study.
Antiangiogenesis antibodies can be generated by the intramuscular injection of the VEGF DNA vaccine;however,the technology is still immature,and the efficacy and long-term impact are not apparent.Hence,further clinical research is needed.Also,angiotensin-converting enzyme inhibitors can antagonize inflammation,increase the number of EPCs and improve the mobilization ability in patients with diabetes.However,this treatment causes an irritating cough,bilateral renal artery stenosis and other adverse side effects[96].In addition,EPC mobilization promotes re-endothelialization,repairs damaged ECs,promotes angiogenesis and restores blood flow[97,98].It is believed that with further research,more treatments can be developed to benefit mankind (Figure 4).
CONCLUSION
The advantages and disadvantages of neovascularization to the body are based on different environments.For,MI,peripheral arterial disease,coronary collateral circulation and DFU,neovascularization needs to be promoted to restore the perfusion of the ischemic area and reduce body damage.Neovascularization should be inhibited for DR and tumors to reduce the risk of retinal stripping or tumor metastasis.Although the involvement of neovascularization in disease pathogenesis is still not specific,it has huge prospects for treating ischemia in diabetes.
FOOTNOTES
Author contributions:Cai Y,Zang GY,Huang Y and Sun Z designed,collected and interpreted data and drafted,revised and approved the manuscript;Zhang LL,Qian YJ,Yuan W and Wang ZQ interpreted data and drafted,revised and approved the manuscript.
Supported bythe National Natural Science Foundation of China,No.82 070455;the Related Foundation of Jiangsu Province,No.BK20 201225;the Medical Innovation Team Project of Jiangsu Province,No.CXTDA2 017010;and the Postgraduate Research and Practice Innovation Program of Jiangsu Province,No.KYCX20_3051.
Conflict-of-interest statement:All the authors report no relevant conflicts of interest for this article.
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is noncommercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Zhong-Qun Wang 0000-0003-3590-9313.
S-Editor:Gong ZM
L-Editor:Filipodia
P-Editor:Gong ZM
杂志排行

World Journal of Diabetes的其它文章
- Risk factor analysis and clinical decision tree model construction for diabetic retinopathy in Western China
- Dietary Nε-(carboxymethyl) lysine affects cardiac glucose metabolism and myocardial remodeling in mice
- Role of defensins in diabetic wound healing
- Combination therapy of hydrogel and stem cells for diabetic wound healing
- Nutritional supplementation on wound healing in diabetic foot: What is known and what is new?
- Orthotic approach to prevention and management of diabetic foot: A narrative review