The perceptions on good death of the older adults in the semi-urban community:A qualitative study
2022-07-31AryTipwongTnwtRumsookThitvnHongkittiynonKnitKgowsiri
Ary Tipwong ,Tnwt Rumsook ,Thitvn Hongkittiynon ,Knit Kgowsiri
a College of Nursing and Health,Suan Sunandha Rajabhat University,Bangkok,Thailand
b Faculty of Nursing,Rambhai Barni Rajabhat University,Chanthaburi,Thailand
Keywords:Attitude to death Aged Community health services Qualitative research
ABSTRACT Objective:This study aimed to explore the perceptions of good death of the older adults living in Bang Nang Li Sub-District,Amphawa District,Samut Songkhram Province,Thailand.Method:The data of the study was collected using in-depth interviews between October 2019 to January 2020.The data collected a total of 14 older adults who had firsthand experience in caring for terminally ill patients were recruited for the study.Content analysis was employed to analyze qualitative data.Results:The results of this study revealed the perceptions of good death which were categorized into three main themes and eight sub-themes,including 1) death without suffering (not suffering from life support devices,dying with care);2) natural death (death with the end of life expectancy,death with illness or ailments);and 3)death without the worries(preparation for death,spiritual and belief practice toward preparation for death,family and property management before death,death among family members and at their familiar place).Conclusion:The findings of this research provided the insight to clarify the understanding of the perceptions on a good death of older adults.The findings can be used to support the practice and management of nursing education and health care providers who have to be involved in palliative care for terminally ill older adults.
What is known?
• Palliative care using the medical technology model to assist terminally ill patients and the perceptions of a good death in the context of rural and semi-urban communities.
• The knowledge on a good death according to the experience of the elderly who had firsthand experience in caring for terminally ill patients.
What is new?
• Perceptions of a good death under the way of Buddhist beliefs and practice,and the needs of older adults living in semi-urban areas.
• Perceptions of a good death according to the experience of the elderly who had firsthand experience in caring for terminally ill patients.
1.Introduction
The world population has increased steadily from the past to the present days.Presently,the United Nations reports that the expected amounts of older people have risen from 962 million worldwide in 2017 to 2.1 billion in 2050 and 3,100 million by 2100[1].Thailand is considered one of the world’s rapidly aging societies with a total population of 66.5 million,of which 12.1 million are older people or approximately 18.2% of the total population [2].In 2018,the proportion of the elderly population reached a hundred[3].Thailand will become a “full-fledged aged society” when the proportion of older people reaches 20%,and the country is expected to enter a “super-aged” society in 2031 with the proportion of the population aged 60 years and over reading 28% of the total population [2].
As medical technology has been developed to be more efficient.As a result,the average age of the population is longer.In Thailand,the average life expectancy at birth is increasing [4].The report from Population Projection of Thailand,2005-2025 by the Institute for Population and Social Research,Mahidol University,the life expectancy of Thai people has increased and people live longer,men have an average age expectancy of 69.1 years in 2010,which increased to 71.1 years in 2020;and women have an average age expectancy of 75.7,increased to 77 years respectively [5].The increasing number of older people indicates the likely future trend of morbidity in the population.Older people will have to deal with greater risks of illness and chronic diseases which require longterm care;for instance,diabetes,amnesia,paralysis,bone and dental diseases,cancer,etc.These chronic conditions require ongoing treatment [6].
Discomfort feelings from illnesses in older adults may affect the health of the elderly themselves and their caregivers,including the long life span and increasing age of life with increased complicated illness[8].Increasing longevity means more people will be dying in very old age,but little is known about the preferences of older people regarding their care at the end of life[9,10].Knowledge and understanding of older persons’ perspectives about death,dying and the last period of life are prerequisites for the health care provider to enable good palliative care.
In accordance,the concept of a good death is gaining attention among people from both domestic and overseas.It can be seen from the National Strategic Plan about the end-of-life enhancement of well-being,in the years 2014-2016;which defined the meaning of good dying as“to die well means dying with enough appropriate and relieving symptoms from physical and mental sufferings;taken care of spirituality corresponding to one’s beliefs,religion,and culture,including being able to complete one’s unfinished intention or mission,being able to express one’s desire for the final care for the peaceful death and human dignity [11].” Meanwhile,the changes in the Thai social context there has been a change from the past relatives have intimacy,sickness has relatives to take care of,children take care of parents when death occurs often in the home,and children learn to prepare for the sick.But in the current state,deaths often occur in hospitals.The role of caregiver for relatives is shifted to focus on care in a nursing home,which deprives relatives or caregivers of the opportunity to care for elderly patients who are in the later stages of life.Some elderly people may want to receive palliative care at home to provide being in a familiar place and environment,being well cared for,and being warmed by family members.
From the literature review on a good death,it was found that most studies reflect the variety of perspectives from health care teams [12-18],patients [15,19],caregivers [20],and relatives[17,20].The knowledge gained from these studies confirms and reflects a good death through experiences from many perspectives of those involved.Although,a good death has been a central concept of palliative and end-of-life care since the beginning.The original model was to keep patients free from unpleasant symptoms without discomfort in areas of psychological,emotional,social,and spiritual [21].The meaning of a good death and its composition of it has,however,been changing[21,22].It is a subject that is difficult to quantify scientifically but is influenced by philosophical ideas,which are believed to be culture-based issues.This has been affirmed by the evidence that decision-making about good death and end-of-life issue was different among racially and ethnically diverse groups and being aware of dying and accepting that the death will occur [23,24].
According to the previous studies,the perceived good death was mostly obtained from a group of health personnel [12-18],terminally ill cancer patients,and their caregivers [17,20].It was found that there was no study among the group of older adults whose roles and responsibilities are to provide care and have direct experience in caring for older people who are living in the final stage of life or dying,and to differences in culture,Western culture has values concerning the process of dying,dignity,and autonomy[25].The characteristics of dying with dignity and privilege of Westerners emphasize the self-determination of death ways,and having the power to control one’s own life,including not being dependent on others,or not being a burden on others,even in the final moments of life.Whereas in Eastern cultures there is acceptance of death.It is considered that life does not end at death but begins a journey to a new world [25].Therefore,the researcher viewed their experiences and perceptions toward the phenomenon of mortality as valuable to gain insights because the information was obtained directly from experienced older adult caregivers for preparation for a good death.
The gap that causes the lack of knowledge even partially may affect the healthcare team professionals to miss an opportunity to understand the various aspects of giving a comprehensive view of mortality and care among the older adults.Therefore,to understand the real needs and perceptions towards the meaning of the good mortality of the older adults in the community that will lead to the provision of services among the healthcare team professionals must be taken into account.The knowledge gained from this study can be used as a guideline for providing comprehensive knowledge-based services entirely to the needs of the older adults with diverse health conditions,lifestyles,and treatment or being in the terminally ill conditions as in the context of Thai society.
Consequently,the researcher was interested in understanding how“gooddeath”is perceivedbyolderadults inthe communityliving in a semi-urban district of a province in the central region of Thailand,and the importance and necessity of doing this research clearly on the issue will benefit the development a care system that provides the needs for the older adults who are in the final stage of life.
2.Methods
2.1.Study design
This study was qualitative research that seek knowledge and perceptions on a good death according to the experience of the elderly who had firsthand experience in caring for terminally ill patients.The perceptions of individuals towards the study issue are subjective and complex.The researcher obtained data using a semistructured interview as a guideline in the in-depth interviews along with field observations and field recordings.Data were obtained from interviews and analyzed using qualitative content analysis.
2.2.Setting
The researcher obtained the data at Bang Nang Li Sub-District,Amphawa District,Samut Songkhram Province.The physical location of an area is approximately 5.58 square kilometers or 3,488 Rai,a lowland area with rivers and canals scattered throughout the area,consisting of 5 villages,802 households,987 families,a total population of 3,828 people,1,868 males,and 1,960 females.Most of the people are Buddhists,and the main occupation of recruited key informants is agriculture,such as planting coconuts,grapefruit,bananas,lychees,etc.,followed by employment in industrial plants such as coconut mills,palm sugar mills,etc.This selected district showed the diversity of the populations in terms of educational and occupational levels and backgrounds.In addition,the surrounding of the study area is a semi-rural sub-district,semi-urban.This should represent the reflection towards the way of life and the perceptions of a good death in the community.
2.3.Participants
The data were collected between October 2019 to January 2020.The researcher approached key informants through gatekeepers who are village health volunteers (VHV) who meet the inclusion criteria by employing a purposive sampling method.There was a total of 14 key informants.The researcher set the inclusion criteria for selecting the informants as follows:1) older person aged 60 years and over;2)having direct experience in caring for terminally ill patients;3)able to communicate in the Thai language;4)living in Bang Nangli Sub-district,Amphawa District Samut Sakhram Province;and 5) willing to participate in providing information.
2.4.Data collection
The researcher collected data from all the key informants.The duration of the interviews lasted about 45-60 min for each key informant.Interviews were scripted and tape-recorded using an audio recorder after obtaining consent.Text data were analyzed using field note analysis and content analysis.The transcripts were read,and responses were categorized by themes.The researcher analyzed along with the data collection and reviewed all the data with the informants afterward for triangulation purposes.To determine the trustworthiness of the study,Lincoln and Guba’s criteria including credibility,dependability,transferability,and conformability were considered [26].
The researcher learned the concepts,theories,and practice regarding qualitative research skills including research methodology,data collection tools,research analysis,ethics,and related topics.The researcher developed a semi-structured interview guideline to use in the process of data collection to obtain relevant information using observations and in-depth interview techniques.
Regarding the process of data collection,the researcher started asking general questions with the purpose to build relationships and assess key informants’ attitudes with common questions including “How are you today?“or “Are there any interesting activities today?etc.”The researcher started asking questions related to their experiences and perspectives of a good death by using indepth interview guidelines and semi-structured interview questions with initial questions covering the perceptions and experiences of care for terminally ill patients.For instance,“How do you feel about being a primary caregiver for terminally ill patients,could you please describe?”“What are your perceptions towards a good death?” and “Could you tell me about your experience in taking care of terminally ill patients?” In case the key informants were not able to clearly explain their feelings or situations,the researcher would ask additional questions using “probing questions”.Types of questions included“Could you please explain more about the issues you told me?And is it possible to provide further detailed information?” This technique could help create meaning about a good death described by the key informants.During each interview,the interviewer first introduced the background and aim of the study and ensured the principles of confidentiality and voluntary participation were clear to the participant.Data collection was stopped when data saturation was achieved.
2.5.Ethical considerations
This study was approved by the Suan Sunandha Rajabhat University Ethics Committee Human Research,Thailand.The approval number was COA.1-047/2018.The researcher informed key informants regarding the objective and detailed information before performing the study,the informed consent forms were obtained from the older adults.Key informants gave informed consent before taking part in the study.The researcher was concerned about their privacy and respected their decision to participate in the study.Key informants were able to withdraw from the study anytime without having any impact on their decisions.The rights of the informants were protected.The results of this study and the moral principles were also considered as follows:1) respect for a person and 2) beneficence or non-maleficence and justice.
2.6.Data analysis
The researcher analyzed the qualitative data using the content analysis method which applied the process of step-by-step analysis[27].The procedures started by listening to the recorded conversations,transliterating conversations into letters word for word,and reading carefully the transcripts of the dialogue to gain insight and understanding of the main points.The researcher took the key points and created a list and code of information individually;then general information was analyzed and categorized.Codes samples of the transcripts identified the similarities and differences.The researcher started looking for the relationships of each category until creating a conclusion by considering relationships from different categories and writing them as the main subject matter to answer the study [27].
2.7.Trustworthiness
Regarding the credibility of research trustworthiness [28],the study covered the accuracy and reliability of the data operated by a team of experienced researchers in the field of qualitative research.The researchers checked the quality of the obtained information.After the research was completed,an analysis and a review were concluded.The research team provided an opportunity for the group of informants to participate in the research during the review of the data and the analysis of the findings.The collaborative review was conducted between the researchers and key informants using the triangulation technique to confirm the validity of the data(dependability).In addition,the researcher was aware of the verification of the data (conformability) [29];so that the informants would review the data after the data collection was completed.
The researchers’process uses a triangulation technique[28].The researchers used multiple methods of data collection such as observations,in-depth interviews,field recordings,etc.,and the researcher confirmed the correctness of the data with member checking by bringing the data obtained from the interview to check the data with the informant to verify the correctness with all informants[29].If any doubtful issues are found,the researcher will ask additional questions for the same understanding.The interpreted data will be consulted with a peer debriefing to obtain the correct guidelines and information in conducting research,and in the presentation of the research results,the words of the informants will be used to confirm the truth and clarity in all aspects of the analysis and reporting of the research results.
3.Results
The results showed that most of the respondents were older adults aged between 62 and 74 years,and half of them were in agricultural areas(50%)and had finished primary school education(57%).(Table 1).
The results of the research reflected the perceptions of the older adults on a good death in three themes:painless death,natural mortality,and carefree mortality(Table 2).The details are as follows.
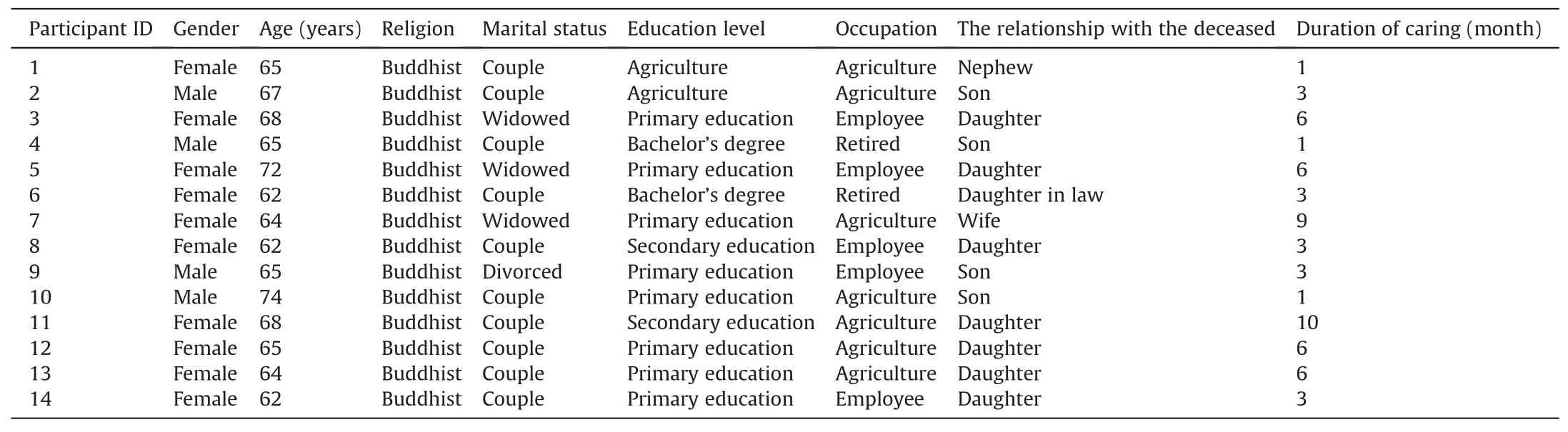
Table 1 Demographic data of the participants (n=14).
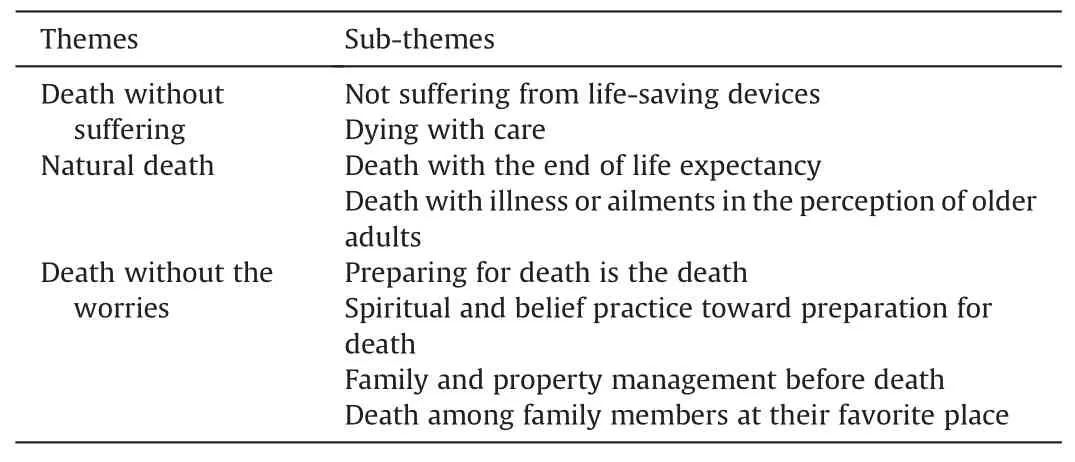
Table 2 Themes and sub-themes that emerged from in-depth interviews.
3.1.Death without suffering
Nonsuffering death meaning for older adults means the death that doesn’t torture the physical body and the death in the state of painless and without agonization when it is near the time of death,or there is no distress and it takes a short time before dying.Painless death can be divided into two characteristics:1) not suffering from life-saving devices and 2) dying peacefully.Details are as follows:
3.1.1.Not suffering from life-saving devices
Not suffering from life-saving devices means that dying by not using the end-stage treatments for the older adults;or critical patients may suffer from the use of life-saving equipment,such as throat piercings for intubation,heart-pumping,or the use of other equipment which helps prolong death but cannot improve the quality of the patient’s life.The perception of good mortality of the older people is the condition that many of them do not want to live with a ventilator for a long time from life-prolonging medical treatment and from being able to live against nature.One example is the case of key informant 3,a female,68 years old,who told us about her experience of perceiving a good death from her mother whom she had taken care of by the end-stage before she died.
“Before my mother died,she had been staying in hospital.I saw her still alive by being used various and messy medical cords of treatment.She wanted to lie quietly in the bed and did not want to be in the conditions of using tumultuous devices and heart pump like this;intubation use,sucking phlegm,etc.All of those things made the conditions so pitiful for me.When the physician come to do those,she always flinched at a time.She didn’t want to die like that.When I said that,it was miserable.If I have to die,I want to die well,I don’t want to die in this condition.” (Participant 3)
Another example,the female had an experience living with her husband’s mother,who was a bedridden patient at the age of 86 before her death.
“I was always with her.I took care of her by helping her to take a shower and fed her every meal.Before she died,she was unconscious.I took her to the hospital.The doctor inserted a ventilator to save her.When she regained consciousness,she pointed to her chest,signaling about being so painful.Her facial expression showed us that she was suffering a lot.She couldn’t speak,and when she passed away two weeks later.If we let her get unconscious just like she was sleeping from the beginning,she would have gone nicely.” (Participant 3)
In addition,the older adults had a perception of good mortality,in terms of a painless and non-torture death.When the time of death almost arrived,there was no discomfort or agitated manner,and within a short time death.Also,it would not be a burden to the descendants,as told by a male.
“A good death,in my point of view,is a normal death,which means dying without agitated manner,painless and no need to be put on many medical life support devices,no piercing,not wearing any instruments.I don’t want to feel tortured.When it’s time for me to die,just die easily and shortly.The longer we struggle to stay alive,the more our children have to suffer for that.” (Participant 4)
3.1.2.Dying with care
Dying with care means that an older adult is not being neglected by healthcare providers,family,and relatives.Older adults should still be taken care of by doctors,nurses,or family members and caregivers to get comfort until they calmly die by nature.
“For the phrase of good mortality,a person who dies well is like my grandmother.She just closed her eyes dying peacefully as a philanthropist.Her offspring could have a chance to take care of her first.She passed away so well by just falling asleep.”(Participant 1)
“Good death means when you die,you are not agitated or distressed.If you are hurt,there is a doctor to take care of you.When it’s time to die,it’s nothing.Go comfortably,if it’s time.” (Participant 4)
“When talking about good death I think of my father when he was passing away.He was not agitated at all.He was lying ill for some time.Before bedtime,I got him medicine and water.Then,before dawn,he passed away.” (Participant 7)
3.2.Natural death
The older adults perceived good mortality as a natural death.Natural death is divided into two characteristics:1) death with end-of-life expectancy and 2) death with illness or ailments.The details were as follows:
3.2.1.Death with the end of life expectancy
Death with the end of life expectancy in the perceptions of older adults means that the body gradually collapses naturally,does not have to be in illness conditions for a long time,and dying persons are not a burden for the offspring to take care of,as the following statements:
“I know all people have to die sooner or later.People who die well,in my sense,is when the time comes,they just die at the right age because they reach their time to depart.” (Participant 7)
“For me,death is normal.When the time comes,everyone must go.If it’s time to go,we’ll go.For me,I have always warned my only child that if my time comes,just let it be.I won’t feel sorry about that because time is over.It must be the right time to leave so don’t be sad.When it’s time,everyone has to go.” (Participant 3)
3.2.2.Death with illness or ailments in the perception of older adults
Death with illness or ailments in the perception of older adults means that dying persons from illness or ailments have time to stay with their family members before passing away.Family members can have an opportunity to take care of and can determine to accept their departure of them as described below.
“A good death is the death of a very old age person who has been able to prepare for dying even though he may die unaware.But,that is because he has merit.Those who die badly die in an accident or a terrifying event.So,this is called a bad death.Those who die well must die from the very old age of expectancy or by illness,not by accidents.” (Participant 7)
“Well,when the time comes,that one comes to us and takes us.It doesn’t matter.Supposedly,my relative in the family,assumes that he has quarreled or argued with anybody when he gets sick at a young age or has some congenital disease and he has to die suddenly.I won’t feel depressed because I know this person has been ill.When it’s time that he can’t stand the disease,he has to leave.”(Participant 3)
3.3.Death without the worries
Older adults have a perception of a good death as a carefree death.It is the death that they have been prepared for before dying in terms of physical,mental and family matters;for instance,dying persons have time to prepare for death with their family members and relatives to accept their death incident one day.So that they can depart without worries or any concerns.There are four categories:1)preparation for death,2)spiritual and belief practice preparation for death,3)family and property management before death,and 4)death among family members and at their favorite place.Details are as follows:
3.3.1.Preparing for death is the death
Preparing for death is the death that a dying person has prepared for physical illness conditions.The medical treatments have been planned together with the physician,the patient,and relatives to provide treatment options for the terminally ill patient to make decisions,and to get ready to leave without concern in any matters as the following statements:
“I used to meet an acquaintance who was dying.He had no opportunity to talk to his children or his wife because he had been on intubation,then passed away,with no preparation for death.If I have to die,I want to go free;no need to worry about anybody or anything.I want to be prepared,without having intubation life support,just let go.All I want is that I can talk to my loved ones and say goodbye to them.No one will have to deal with difficulties because of me.” (Participant 4)
“Regarding death,I think we all have to surely meet one day.Now,ask me if I’m afraid.I am.But we have to be prepared to take care of things early.When it’s time,my children will make their own decisions for what kind of treatment will be.” (Participant 5)
3.3.2.Spiritual and belief practice toward preparation for death
The perception among older adults who religiously believe in Buddhism means that at the end of life,dying persons should not be attached to anything or even themselves,freeing their minds from all attachments.According to the Buddhism religious,when a person is dying,he/she has to give up all the material possessions and stop worrying about anything;moreover,a peaceful mind at the moment of death was very important for Thai people since,according to Buddhism,it will lead to beneficial next life;whereas a negative state of mind will contribute to a harmful one.The atmosphere around the dying,therefore,was to be peaceful.Cousins would gather around the dying,reminding them of their good deeds in the past and helping to relieve them of all anxiety.If dying in that kind of mental state,it is a good death as the following statements:spiritual practice.
“If she had been able to go back before she died,what would she prepare for? She said if she had money from selling rice fields,as she had wished for,she would have donated each amount of money to the temple.The certain amount is about ten thousand baths for each temple.She had the intention and said it out loud,but she hasn’t died yet.She wants to make merit by donating.Thus,when you die,you cannot take anything with you,except merit and sin.”(Participant 5)
“For me,I always warm my child that if my time has come,I mean dying,I won’t be sorry because my time is over.It is the truth of life.” (Participant 3)
3.3.3.Family and property management before death
Family and property management before death,which means that the older adults want to be unworried about family and property by pre-management before death.The property,such as inheritance,land,and various assets should have been premanaged to reduce quarreling between family members and for the satisfaction of everyone,not a burden to offspring as the following statements:
“For me,I think that if it is very close to death time,then everything must be done before dying.The inheritance must be identified.Do not let descendants argue or quarrel.I think like this.”(Participant 4)
“Before my mother died,she had said the same.She said that if she died,she didn’t want her children to quarrel with each other because of her money.She had saved some money and I thought I would make merit for her,for my parents.I didn’t think about money a lot.When she lived,she didn’t bother us.She had her saving.Children didn’t have to worry.She didn’t have to bother kids financially at all.” (Participant 3)
“I’m still worried a bit.I have two children,ages 37 and 33.They both are government officers and are still single.I’m a little worried about them building their own family.If they have families,then I would be more satisfied.” (Participant 9)
3.3.4.Death among family members at their favorite place
Death among family members at their favorite place means that older adults have perceived a good death as a carefree death meaning dying among their loved ones and at their favorite place;and dying persons can have an opportunity to communicate with their family members and their offspring while they are still sensible,such as saying goodbye to family members,relatives,or friends,or they can choose to die at home as they want,etc.Dying at their favorite place where they want to and are surrounded by family members and offspring causes terminally ill patients or older adults to pass away in a warm atmosphere.The older adults,therefore,want to die at home because it is believed that if someone dies among the loved ones and the familiar places,this will help the elderly to die well as the following statements:
“My father didn’t say anything,he wanted to stay at home where he had spent his life building and living in.My parents had built their home together.They had started their lives with nothing.Both of them had nothing.They had gotten 7-8 children then they built a house.Because of this,he wanted to die at home.Like my mother,as she is over 90 now,she also wants to die at home.She doesn’t want to go to the hospital,she would rather stay at home.”(Participant 3)
4.Discussion
Older adults have perceptions of a good death as a painless and non-agonizing death.When it is near departure time,there is no distress and it takes a short time before dying.Based on the results of the study,the older people provided the meaning of a good death in terms of receiving care without suffering from illnesses or any discomfort.The suffering from ailments,chronic diseases,and/or incurable diseases among older people at the end of their life is a reflection of the torture in terms of both physical and mental.Those symptoms disturb their lives and cause various discomforts,including suffering,worries and the thought of not needing to be a burden to their offspring.They also suffer from the very painful condition of diseases.At this stage,the dying patients often think that if their lives may be prolonged through medical technology,for example,they would be a burden to their families[19],causing the patients to become depressed and cannot leave peacefully.Besides,the patients,caregivers,their families,and nurses who are taking care of them wish that the dying patient could die peacefully,without prolonging their lives [13].It is also the desire of dying persons in many cultures to peacefully pass away[30],which is as well as the goal of the end-stage among patient care [20].Therefore,the results of this study reinforce the perceptions among older adults towards good death that in case of illness before death patients should not require unnecessary treatment or prolonged death.Dying persons should be in the state without suffering and not being treated as an object,or as the condition that not being able to help themselves.
The natural death of older adults can be explained by the beliefs of Thai people who are influenced by Buddhism.It is believed that a good death is a natural death,a peaceful death,a lifelong death,or old age.But if it’s a bad death or a fatal death,it’s an untimely death that may be caused by murder,suicide,or death from an accident.By these deaths before death,there will be suffering,especially the suffering of bodily pain[31].From the study,the older adults have perceptions of a good death as death by life expectancy since the body has been naturally deteriorated.This can be explained that due to the aging of the older adults,preparation for death idea is becoming more pronounced;older adults think of death more often.Elderly people who perceive the condition of actual health will be aware of planning to prepare for death.Preparing for death occurs with patients who are aware of their dying process and how long they will live [32].The findings are consistent with several other studies [32,33] which could explain how well-prepared for death is understood by the patient and caregiver.
People who are dependent and have faith in religions will believe that religions can influence anxiety,concerns,and attitudes about death and near death[34].Moreover,the patients who have a bond with God and believe in the next life will feel satisfied with dying with honor,resulting in acceptance of the coming death.They have hope and peace and are more likely to be well prepared to die.The strictly religious person is a statistically significant predictor of their own pre-mortality needs [35].Therefore,in this research,it is believed that older adults with religious beliefs about death are likely to be more prepared to face death and near-death conditions than ones who have less religious beliefs concerning death.
In addition,in terms of managing family and property before death,older people have to communicate directly to those around them to let them know the final will.When communication is clear,the family and relatives will know what and how to fulfill the wishes of the departing person.Because when entering the last stage of life,older adults will encounter pain or disturbances from near-death conditions [36].Therefore,for the elderly to die,they elderly may think of not only themselves but also those around them,especially loved ones,and do not want themselves to be a burden to those who are still alive.Which concerns or having unsettled things will prevent the patient from leaving peacefully.Moreover,if the older patients die among their loved ones and at their beloved place,do not let them die alone at home and/or at the hospital[19].This mortality caused the patient’s peaceful departure with the feeling of warmth and companionship [37].Due to the importance of being the care of the family for people,this shows the interaction between family members.From the research evidence [38],it was found that the family is a source to support the members in terms of emotions,love,encouragement,value giving,information possession,and money.So,the family is an important context for a dying person.When changes occur in a family,whether positively or negatively,there will be impacts on family members.This concept reflects that families have important responsibilities,roles,and mechanisms in caring for family members both in normal conditions,during health deviations,and at the end stage of their lives[38].
The perspectives of patients about the need to always be with their families at all times by the end of their lives,especially before dying,even when they are already unconscious could help them to die peacefully;especially when someone they love only sits beside them make them feel warm and not alone[19].It also corresponds to having enough time with the family,expressing feelings to family members,and believing that the family will take care of their body afterward.The death in which the family is ready and supportive of their death is one of the attributes of good mortality of a dying person[39].Consistent with studies of terminally ill patients in America and Europe [40],the characteristics of a good death were control of pain and other symptoms,clear decision-making,feeling of not being alone accepted as a person prepare to die,and helping others.It can be seen that the perception of death is good in both Thai contexts,and Western contexts have both things in common,namely no physical suffering,and the different part is being in the midst of a family.In which the Thai context and Asian countries place a greater emphasis on family than in Western societies that emphasize recognition as a person with selfdetermination [40].
A good death is related to the perceptions,beliefs,religion,culture,and experience of Thai society;in which the patients in the final stage of life desire to die at home in a familiar atmosphere,among family members,relatives,and loved ones [41,42].In Thai culture,taking care of the parents is the duty of the offspring to express their gratitude to elders [43].As it can be seen from the findings,informants who provided qualitative information are a child,a daughter-in-law,and/or a partner who acts as a caregiver for terminally ill older adult patients.The context of Thailand especially in rural societies often shows that people have a close relationship with each other,pay respect to older adults,and take good care of older people when they are sick.Although the study area is a large provincial area with the natural context of a semiurban community,people still have close relationships with older adults.
In addition,Thai culture,Buddhism religion,social community,and family have contributed to making people view a good death as a part of nature.Generally,when someone in the community is sick,neighbors,relatives,and family members often come to visit and have a small talk with the sick.The offspring and related family members often take turns to provide care for the sick [44].Therefore,most of the deaths occurred at home in the surrounding of familiar people and the atmosphere would help the dying person to leave peacefully.Moreover,understanding the life circle (Birth,Aging,Sickness,and Death)enables the dying person to cope with death and support the family members to let go of the dying person easier.The community also helps support the family of the death through performing religious rituals that are consistent with the beliefs and traditions of Thai people.
The people’ perceptions toward a good death reflect the social and cultural aspects of the local community that view a good death as a meaningful and valuable moment of life;as well as reflect the social relationship among family members,neighbors,relatives,and health personnel through the care,the home visit,and religious rituals within the community.If health providers,nurses or everyone involved in caring for terminally ill patients lack knowledge in care in the dimension of cultural and social value,it will cause disrespect to patients’ dignity,and not allow the patients to enter a peaceful death.Therefore,gaining a better understanding of a good death in-depth in terms of social and culture is very important in nursing practice to participate in palliative care for older adult patient.
5.Limitations
The study employed a gatekeeper approach in a selected subdistrict.Therefore,the context of each area must be considered when interpreting the results of this study.
6.Conclusions
The findings of this study indicated an important understanding and perceptions of a good death which its information was obtained from the experience of the older adults.Nurses,families,and communities should take part in the holistic care of terminally ill older adults.The findings of this study could be used to suggest implications for nursing practice,education and research.The recommendations are as follows;nursing practice should design nursing care based on the perspectives and the need for a good death according to the experience of the older adults,and encourage the primary caregivers of older adults to participate in palliative care.For nursing practice;educational institutions should coordinate with hospitals in providing care and design a short course of palliative care training for older adults.And nursing research;nursing institutions should develop a research project in the community to strengthen palliative care management for older adults.
Funding
The research grant for a potential lecturer was supported by Suan Sunadha Rajabhat Thailand.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
CRediT authorship contribution statement
Araya Tipwong:Conceptualization,Methodology,Software,Formal analysis,Investigation,Data curation,Writing -original draft,Writing -review &editing,Visualization,Project administration,Funding acquisition.Tanawat Ruamsook:Validation,Resources,Writing -review &editing.Thitavan Hongkittiyanon:Methodology,Validation,Resources,Writing -review &editing,Supervision,Funding acquisition.Kanit Kgowsiri:Methodology,Validation,Resources,Writing -review &editing.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
We would also like to express our gratitude and thanks to the older adults and who kindly agreed to provide information,the research and development institute Suan Sunandha Rajabhat University,the College of Nursing and Health at Suan Sunandha Rajabhat University for sponsoring the research.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.06.001.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of white noise on procedural pain-related cortical response and pain score in neonates:A randomized controlled trial
- Preventive strategies for feeding intolerance among patients withsevere traumatic brain injury:A cross-sectional survey
- Effects of multidisciplinary exercise management on patients after percutaneous coronary intervention:A randomized controlled study
- Implementation strategies to improve evidence-based practice for post-stroke dysphagia identification and management:A before-andafter study
- Development and validation of a rapid psychosocial well-being screening tool in patients with metastatic breast cancer
- The relationship between acceptance of illness and quality of life among men who have sex with men living with human immunodeficiency virus:A cross-sectional study