The relationship between acceptance of illness and quality of life among men who have sex with men living with human immunodeficiency virus:A cross-sectional study
2022-07-31ChngGoXuelingXioLiZhngHehuXuMinWngHonghongWng
Chng Go ,Xueling Xio ,Li Zhng ,Hehu Xu ,Min Wng ,Honghong Wng
a Xiangya School of Nursing,Central South University,Changsha,Hunan,China
b Nursing Department,Handan Central Hospital,Handan,Hebei,China
c The First Affiliated Hospital of Zhengzhou University,Zhengzhou,Henan,China
d The Institute of HIV/AIDS,The First Hospital in Changsha,Changsha,Hunan,China
Keywords:Acceptance of illness Cognitive appraisal HIV infections Male homosexuality Quality of life Sexual and gender minorities Vulnerable populations
ABSTRACT Objectives:To explore the relationship between acceptance of illness and quality of life(QOL),and factors associated with acceptance of illness among men who have sex with men (MSM) living with human immunodeficiency virus (HIV).Methods:Three hundred and one MSM were recruited from an HIV clinic between August and December 2018.The battery of measurements consisted of the Acceptance of Illness Scale,World Health Organization Quality of Life Questionnaire for HIV brief version,HIV Cognitive Appraisal Scale and a selfdesigned questionnaire used to collect general information.Pearson correlation test was used to examine the relationship between acceptance of illness and QOL.Univariate and multivariate ordinal logistic regression analyses were used to examine whether the general data (demographic and HIVrelated clinical data) and HIV cognitive appraisal were associated with acceptance of illness levels.Results:Descriptive analysis showed the acceptance level among MSM living with HIV was moderate(Mean=26.29,SD=5.28).Those with a better acceptance of illness had a better QOL(r=0.69,P<0.01).In the multivariate ordinal logistic regression model,education level,threat appraisals (OR:1.09;95%CI[1.06-1.13]),and controllability appraisals (OR:0.82;95%CI [0.71-0.94]) were significantly associated with acceptance of illness.Conclusions:Results showed acceptance level was moderate and had a positive correlation with QOL.High level of education,low threat appraisals and high controllability appraisals were related to high illness acceptance.This finding highlights the importance of focusing on HIV-infected MSM with low education and on their perceptions of threat and controllability about HIV-related issues when designing interventions to promote illness acceptance in this vulnerable population.
What is known?
• The quality of life (QOL) of people living with human immunodeficiency virus (HIV) is suboptimal despite effective antiretroviral therapy,especially for men who have sex with men(MSM) living with HIV.• Acceptance of illness was positively related to QOL in patients with various chronic diseases and might be a clue to improving the QOL of MSM living with HIV.
What is new?
• The acceptance level of MSM living with HIV was moderate and had a positive correlation with QOL.
• High level of education,low threat appraisals and high controllability appraisals were related to a better illness acceptance.
• Improving QOL of MSM living with HIV requires not only medical treatment and routine care,but also their acceptance of HIV.Medical staff should focus on the physical and mental health of their patients and ultimately improve their QOL.
1.Introduction
The human immunodeficiency virus (HIV) epidemic in China keeps growing,and men who have sex with men (MSM) are the vulnerable population to HIV infection [1,2].The overall estimated HIV prevalence among Chinese MSM was 5.7% from 2001 to 2018,with an increasing trend over time [3].Globally,the risk of HIV infection among MSM was 25 times higher than heterosexual adult men,and MSM accounted for 23% of HIV infections in 2020 [4].Thanks to antiretroviral therapy (ART),HIV has become a chronic disease and people living with HIV (PLWH) have a prolonged life expectancy.However,quality of life (QOL)of PLWH is significantly lower than that of the general population,especially MSM living with HIV[5,6].Chinese MSM living with HIV not only face physical,psychological and social problems,but also suffer from the stress of HIV infection and the stigma and discrimination associated with HIV and sexual minorities[6,7].The above multiple stressors have been shown to increase the risk for increased viral load,nonadherence to medication,and decreased QOL [8,9].Given that QOL is an important indicator of HIV treatment and management and that the QOL of MSM living with HIV is of great concern,it is urgent to explore the factors associated with QOL of MSM living with HIV.
Acceptance of illness is the cognition of the positive meaning of an illness,and it restores personal control by integrating illness experience into patients’ lifestyles [10].It is also a psychological indicator used to measure the degree of disease adaptation [11].Acceptance of illness might be a clue to improving the QOL of MSM living with HIV given that acceptance of illness has been demonstrated to be associated with QOL among people with various chronic diseases,such as lung cancer,renal disease,and HIV[12-14].Andrinopoulos and his colleagues[15]conducted a crosssectional study to explore the relationship between acceptance of illness and QOL among PLWH,and they found that PLWH with a higher acceptance of illness had a significantly better QOL.Although evidence has been found between acceptance of illness and QOL,the relationship between acceptance of illness and QOL among MSM living with HIV has not yet been reported.Moreover,understanding the acceptance of illness of Chinese MSM living with HIV is meaningful since they are struggling with social,mental,and physical problems.This may provide a different perspective for constructing intervention strategies to improve QOL in MSM living with HIV.Therefore,to provide information that is useful in the development of acceptance of illness-driven QOL promotion interventions among HIV-positive MSM,this study focused on acceptance of illness,particularly on the status of acceptance of illness among MSM living with HIV,on the relationship between acceptance of illness and QOL,and the factors related to acceptance of illness.
According to the Stress and Coping Model,HIV becomes a stressor when MSM are diagnosed with HIV infection,and the process of cognitive appraisal and coping determines their QOL.Acceptance of illness is a psychological indicator of the degree of disease adaptation [11].A study has reported that cognitive appraisals are a strong predictor of adaptation to chronic illnesses[16].Illness cognition is associated with personality,experience,disease burden,and treatment response,and it ranges from adaptation to maladaptation[17].In addition,acceptance and cognitive reappraisal are two emotion regulation strategies that are positively associated with beneficial psychological outcomes [18].Acceptance and cognitive defusion are the core processes of acceptance and commitment therapy [19].Theoretically,acceptance of illness is associated with cognitive appraisals of a disease(Fig.1).Yet,little is known about the relationship between acceptance of illness and cognitive appraisal,especially in the MSM population.
Previous studies reported that age,education,and financial status were associated with acceptance of illness [20,21].Cipora et al.[22] reported that,among women with breast cancer,age is negatively correlated with acceptance of illness compared with education,marital status,and place of residence.By contrast,the marital status of patients with epilepsy was related to acceptance of illness compared with age,sex,and level of education[23].Diabetic women with a better financial status showed a higher acceptance of illness[24].Some social demographics of patients are undoubtedly associated with acceptance of illness,but such associations differ in various diseases.MSM living with HIV are confronted with HIVrelated and sexual orientation-related issues concurrently,and the relationships between their sociodemographic characteristics and acceptance of illness are more complex.Understanding the sociodemographic factors related to acceptance of illness in MSM would help researchers develop interventions targeting at specific MSM.
Illness-related factors affecting patients’ acceptance have been previously identified.A study reported that illness duration was negatively associated with acceptance of illness in patients with osteoarthritis [25].However,no significant correlation was found between the duration of disease,the type of seizure,as well as the kind,dosage,and generation of medicine in patients with epilepsy[23].Another study involving patients with ulcerative colitis showed that disease symptoms did not affect illness acceptance,whereas the type of treatment influenced illness acceptance [26].Illness-related factors reflected the effects on acceptance caused by the illness itself.A better understanding of how clinical factors influence acceptance could help researchers to choose the timing of intervention during the occurrence of the illness.
Our study aimed to determine 1) the current status of HIV acceptance of MSM living with HIV;2) the relationship between acceptance of illness and QOL;3) the influencing factors of acceptance of illness,including cognitive appraisals,sociodemographic and illness-related characteristics.
2.Methods
2.1.Study design and participants
This cross-sectional study was conducted in Changsha,Hunan,China,between August and December 2018.We used consecutive sampling to recruit participants from an HIV clinic in Changsha First Hospital.After obtaining the informed consent of the eligible participants,four investigators explained each item of the structured questionnaires and assisted them in filling in questionnaires.The investigators double-checked to ensure that each item was filled in correctly and,if not,asked the participant to make it up in time.Finally,we enrolled 301 MSM living with HIV,which was sufficient to examine the ordinal logistic regression analysis,since the ideal sample size was at least 5-10 times per variable.Eligible participants have met the following criteria:1)diagnosed with HIV;2)18 years old or older;3)willing to participate with informed consent;4) able to communicate;and 5) self-reported homosexual or bisexual men.MSM living with HIV with cognitive impairment or active psychosis were excluded.
2.2.Measurements
2.2.1.Sociodemographic and HIV-related information
Sociodemographic information,including age,marital status,education level,monthly personal income,and employment status,were collected.Data related to HIV status included the number of months since diagnosis of HIV infection,ART status,and most recent results for CD4+T-cell count and viral load.
2.2.2.Acceptance of illness
To assess the MSM’s acceptance of living with HIV,we used the Acceptance of Illness Scale(AIS)developed by Felton[27].With the consent of the original authors,our team did the translation,backtranslation,expert consultation and preliminary experiment to obtain the formal Chinese version of AIS with good reliability and validity [28].The content validity index was 1.0,and the Kaiser-Meyer-Olkin test value was 0.854.The Cronbach’s α coefficient was 0.801.The AIS measures the acceptance levels of adult patients suffering from any diseases.These questions focus mainly on the limitations caused by an illness,lack of self-sufficiency,dependence on others,and low self-esteem.The AIS consists of eight items,each of which was rated using a five-point Likert scale,with 1 representing strongly agree and 5 representing strongly disagree.The total scores range from 8 to 40.Low scores(8-18 points)suggest the lack of acceptance and a strong feeling of mental discomfort.Moderate scores (19-29 points) indicate that patients have managed to partially accept the disease.High scores(30-40 points)show good acceptance of illness and few negative moods related to the illness[29].The Cronbach’s α coefficient in this study was 0.804.
2.2.3.Quality of life
The World Health Organization Quality of Life Questionnaire for HIV brief version(WHOQOL HIV BREF)was used to assess the QOL of MSM.The WHOQOL HIV BREF was designed to evaluate the QOL of PLWH,and it has been widely used worldwide [30-32].It consists of 29 items and 6 domains:physical,psychological,level of independence,social relationship,environment,and spiritual health.Two items,namely,perceived QOL and perceived physical health,examine the general QOL[33].Each item was rated using a five-point Likert scale with a total maximum score of 130.High domain scores and total scores indicate a better QOL.The Chinese version of the WHOQOL HIV BREF was used and was validated in Chinese PLWH[34].The Cronbach’s α coefficient for this scale was 0.913,whereas that for each domain was between 0.602 and 0.757[35].
2.2.4.Cognitive appraisal
The HIV Cognitive Appraisal Scale(HCAS)was used to assess the MSM’s appraisals of threat,challenge,and controllability when confronting HIV-related issues[16].Six threat appraisal items were rated using a seven-point scale (1=no harm;7=extremely harmful) to determine the potential harm that HIV-related problems may cause in different aspects of one’s life,including important life goals and self-respect.Three challenge appraisal items were also rated using a seven-point scale (1=no potential;7=high potential) to determine the potential of HIV-related problems to promote personal growth and personal challenge or strengthen a relationship.Controllability was measured by two items rated using a seven-point scale.These two items were used to evaluate the extent to which problem 1) could be changed and 2)must be accepted or adjusted to.The Chinese version of the appraisal questionnaire was developed by Gao L [36],and it had good reliability and validity.The Cronbach’s α coefficient was 0.738 in this study.
2.3.Statistical analysis
Raw data were entered using EpiData version 3.1 and analyzed using SPSS version 18.0.Continuous variables were presented as mean ± standard deviation (SD),and categorical variables were expressed as frequency and percentage.Pearson correlation test was used to check the relationship between acceptance of illness and QOL.Univariate ordinal logistic regression analysis was used to examine whether variables including age,education,marital status,employment status,personal income,ART status,and duration of HIV infection,threat appraisals,challenge appraisals and controllability appraisals were associated with AIS levels(using low AIS as reference category).Factors with a statistical significance of P<0.10 in the univariate ordinal logistic regression analysis were included in the multivariate ordinal logistic regression analysis.The critical level of statistical significance was set at P <0.05.
2.4.Ethical considerations
This study was approved by the institutional review board of the Xiangya Nursing School of Central South University(NO.2018019).Prior to the conduct of this study,all the four investigators were briefed on the details of study,and they were trained on the procedure of data collection.The investigators explained the aim of the study,the process of participation,risks or benefits of participation to the potential participants.The participants were aware of their rights and responsibilities,and they were told they could refuse to participate at any time in this study.A verbal or written informed consent was obtained from all participants.
3.Results
3.1.Sociodemographic and HIV-related characteristics
The mean age of the 301 MSM was 29.43 years (range:18-57 years).Most of them (93.7%) were of Han nationality,and about 15.0% of the participants had a religious affiliation.A total of 33(11.0%) MSM married a woman,and 41 (13.6%) had stable sexual partners.Nearly half of the MSM had a bachelor’s degree or higher.More than 50%of the MSM did not know their viral load,and only 29.2%had a viral load below the detectable level.Fifty-four(17.9%)of them kept their HIV status confidential;the rest opted to disclose their condition to others,and they answered the item in the questionnaire that deal with the extent they perceived social support from the people to whom they have shared their condition.The average duration of HIV infection was 30.4 months (range:0.5-136.0 months),and the median was 23.0 months.Table 1 shows the characteristics of the MSM living with HIV.
3.2.Descriptive analysis of acceptance of illness,HIV cognitive appraisal,and quality of life
In this study sample,the overall AIS level was moderate(Mean±SD:26.29±5.28).Low illness acceptance(1-18 points)was noted in 8.0% (24/301) of the MSM,moderate (19-29 points) in 64.8% (195/301),and high in 27.2% (82/301).The minimum and maximum AIS scores were 12.0 and 40.0,respectively.The scores for threat appraisals ranged from 6 to 42 (Mean±SD:21.18 ±9.01).The average result for the challenge appraisals was 9.00 ± 4.25(range:3-21) and that for controllability appraisals was 10.57 ± 1.94 (range:5-14).The total score for WHOQOL HIV BREF was 83.77±11.81,and the highest and lowest scores were observed in the dependence domain (15.35 ± 2.23) and social relationship domain (12.77 ± 2.74),respectively.Table 2 shows the WHOQOL HIV BREF scores.
3.3.Correlations between AIS and WHOQOL HIV BREF
The total AIS score was significantly correlated with every domain of WHOQOL HIV BREF,and the relationship was moderately powerful(Table 2).The two items that examined the general QOL were associated with AIS.The total AIS score had a positive relationship with the total score of QOL (r=0.69,P <0.01).
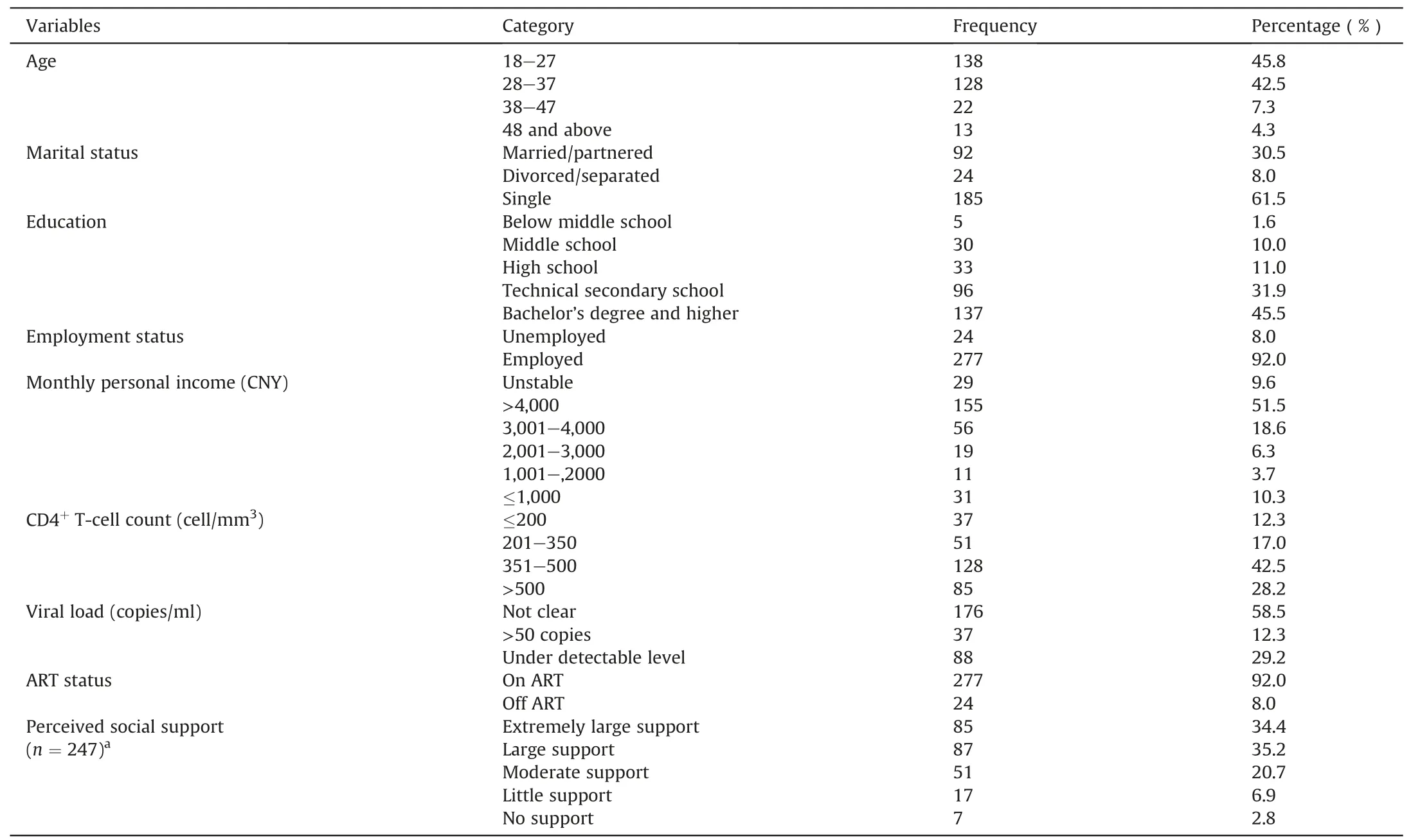
Table 1 Characteristics of men who have sex with men living with HIV (n=301).
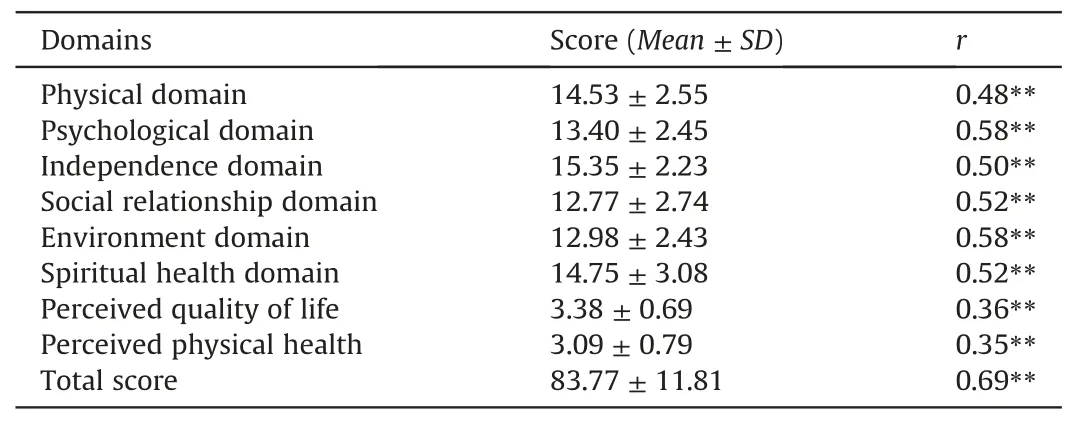
Table 2 WHOQOL HIV BREF scores and their correlation with acceptance of illness(n=301).
3.4.Determinants of acceptance level
Three variables were found to be associated with acceptance level,including education,threat appraisals and controllability appraisals in the univariate ordinal logistic analysis.
In the multivariate ordinal logistic analysis,the MSM with lower education were less likely to accept their disease (Middle school:OR=2.97,95%CI [1.23-7.19];Technical secondary school:OR=2.18,95%CI [1.21-3.90]).MSM living HIV with higher threat appraisals were more likely to have a lower level of acceptance of HIV(OR=1.09,95%CI [1.06-1.13]).Better acceptance of HIV was associated with higher controllability appraisals (OR=0.82,95%CI[0.71-0.94]).The results were detailed in Table 3.
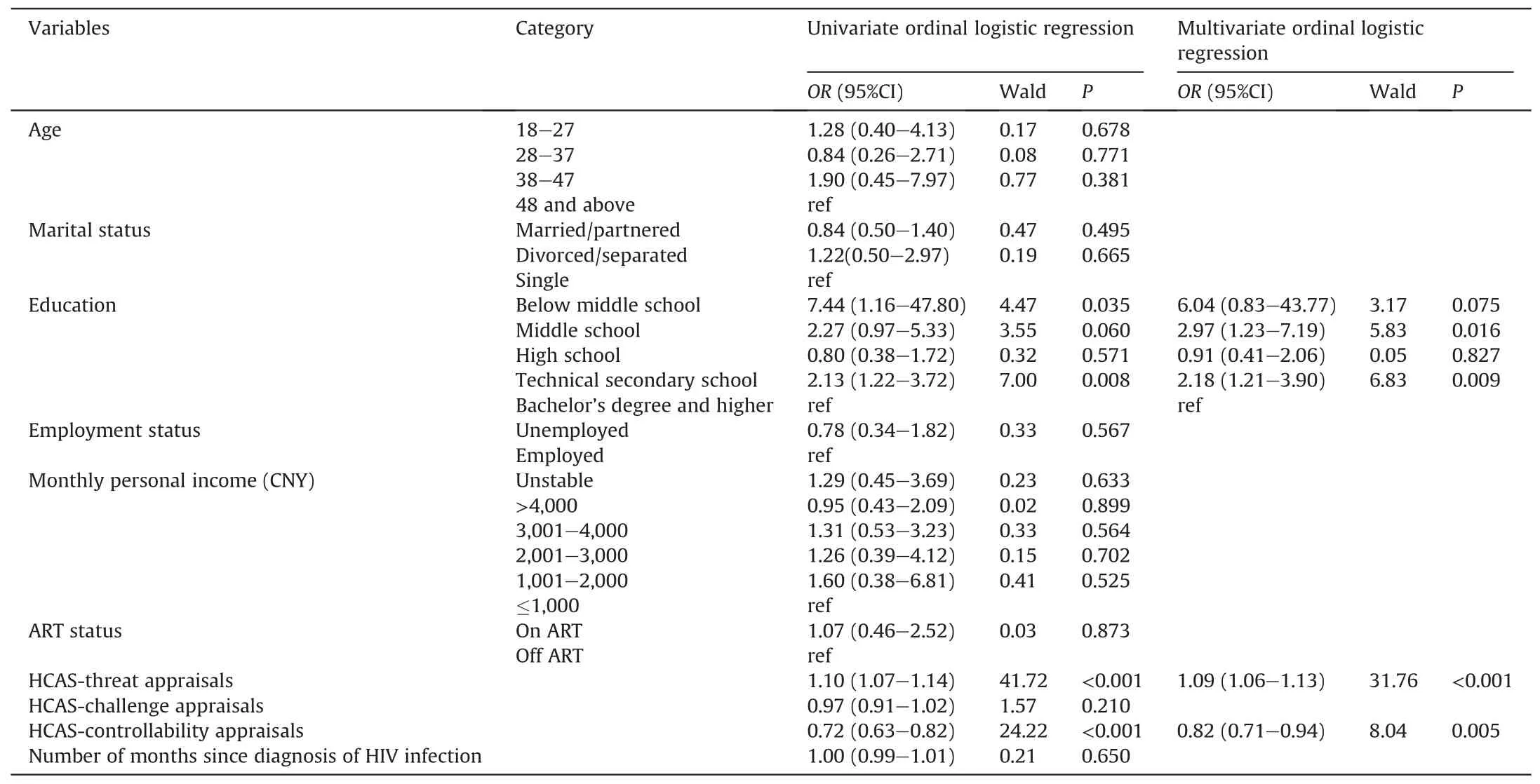
Table 3 Factors associated with acceptance of illness (n=301).
4.Discussion
This study aimed to find out the relationship between acceptance of illness and QOL,and factors associated with acceptance of illness among MSM living with HIV.The acceptance level of the MSM living with HIV was moderate and was positively correlated with QOL.High level of education,low threat appraisals,and high controllability appraisals were associated with a better acceptance of illness.
4.1.Comparison with previous studies
The acceptance of illness of the MSM living with HIV was at a moderate level.AIS has been used in Polish culture,and studies found a medium level of acceptance in patients suffering from different diseases [23,37,38].Studies conducted in other countries and populations showed similar results[10,12].Our finding showed that the mean AIS score among the MSM living with HIV was at the medium level and was even higher than that of patients with other diseases,such as chronic obstructive pulmonary disease (COPD)and cancer [38-40].We recruited the participants from an HIV clinic where they undergo regular tests,such as viral load,CD4 count,and liver function tests,and where they receive antiretroviral drugs.Most of them were in a chronic condition of HIV infection because of timely administration of ART,and experienced fewer symptoms than patients with other illnesses,such as COPD and cancer[14,39].Another reason may be the innate personality of men and the responsibilities and obligations the Chinese society assigns to men;these factors lead men to accept their disease condition more quickly.Notably,45.5%of participants in our study had a bachelor's degree or higher,and the high level of literacy led to a higher level of acceptance of HIV.The above reasons may explain why the MSM living with HIV had higher mean AIS score than those with COPD and cancer.However,only 27.2%of the MSM living with HIV had a high AIS score,and 8%of them did not accept their condition.Most of them only partially or rarely accepted that they would spend the rest of their life with HIV,and this denial hampered their adaptation to this illness and influenced their lifelong commitment to HIV management.This finding suggests the need to assess the level of acceptance and to provide interventions and support for those HIV-infected MSM with a moderate or low level of illness acceptance.
Interestingly,the total QOL score in this sample was higher than the national norm for WHO QOL-100 in China [41].The scores for the environment and spiritual health domains were higher than the national norm;however,the scores for the physical,psychological,independence and social relationship domains were lower than the national norm.The increase in scores for the environment and spiritual health domains might be because of the development in the Chinese economy and in health services and to the openness and tolerance of HIV infection in the Chinese society over the past 20 years.We also found that the overall QOL in our sample was lower than that reported by a study involving HIV-infected MSM aged 16-24 years in Zhejiang province [42].Younger participants living in developed regions may contribute to the differences in findings.However,the QOL of MSM living with HIV is not optimal,and it warrants attention.
We found AIS level was significantly associated with QOL,consistent with other findings [12,43,44].A study involving HIVinfected adolescent and young adult women showed that every domain of the HIV-Health Related Quality of Life was correlated with acceptance,indicating that high current life satisfaction,low illness-related anxiety,and low illness burden are associated with a high acceptance of illness [15].Acceptance is an important link in the process of adaptation to illness,and it means recognition of the need to adapt to chronic illness and to cope with its aversive consequences[45].Acceptance of illness promotes patients’adherence to medication,promotes their active participation in the treatment,and instills a positive and hopeful attitude toward life [46].A high AIS score indicating the ability to overcome limitations caused by an illness and to be independent and self-sufficient corresponded to a high overall QOL and a high score in every domain of QOL.This finding demonstrates the feasibility of acceptance of illness-driven QOL promotion interventions.
As hypothesized,a high acceptance of illness was associated with low threat and high controllability appraisals,but not with challenge appraisals.Studies indicated that low threat and high controllability appraisals are associated with a better psychosocial adjustment to HIV/AIDS[16].The appraisals of an illness as a threat are likely to affect adjustment negatively because threat appraisals may generate stress that exceeds a person's coping resources and skills [47].When a patient sees illness as a controllable event,it means they can confidently cope with the disease and they can overcome the difficulties caused by the illness.Thus,controllability appraisal was positively related to acceptance of illness,whereas threat appraisal negatively influenced the acceptance of illness.
Among the demographic factors,only education level was significantly associated with acceptance of the MSM living with HIV.A study on ulcerative colitis,ankylosing spondylitis,and COPD[26,29,48] showed that patients with a high educational attainment had high AIS scores,consistent with our findings.Patients with high education are more aware of the consequences associated with the deterioration of diseases,and they are more willing to learn skills or knowledge to integrate the diseases into their lifestyle;such attitude promotes their acceptance of their illness[49].For those who are less educated,health care providers are the best way to get information about HIV.However,they are afraid to ask their doctors questions because they fear their care will suffer and they will be perceived as a difficult patient,which is called“whitecoat silence” [50].Doctors and nurses should give explicit permission and encourage patients to ask questions.Most HIVinfected MSM believe that good attitudes of doctors and nurses also have a positive impact on acceptance of illness.The other demographic factors,such as age,marriage,employment status,and monthly personal income,were not associated with acceptance of illness,and this finding is inconsistent with that of previous studies[22,48].
Unexpectedly,HIV-related variables were not associated with acceptance of illness.This finding is consistent with the study of Staniszewska et al.[23],who investigated patients with epilepsy;they found that there is no correlation between acceptance and medical factors,such as duration of illness and kind or dosage of drugs.Specifically,our finding revealed the absence of a relationship between length of HIV diagnosis and acceptance of illness,inconsistent with previous findings which showed that a longer duration of illness and the resulting limitations contribute to a low level of acceptance[24,48].The median of duration of illness in our study was 23.00 months,and only 11%of the MSM living with HIV had other coexisting diseases.This factor might explain why acceptance of illness and infection duration were not significantly associated with each other.Further study needs a larger sample size to explore the relationship between acceptance of illness and disease-related factors.
4.2.Implications for clinical practice
Acceptance of illness is an influencing factor of QOL and this study suggested that interventions for acceptance of illness might have the potential to promote QOL in MSM living with HIV.In addition,MSM living with HIV with low education levels are the neglectful and vulnerable population.Clinicians and nurses should pay more attention to their acceptance of illness and provide timely interventions or guidance.For those with low acceptance level,healthcare providers could assess their cognitive appraisal and give interventions to adjust their perception and ultimately improve acceptance of illness.Acceptance of illness is a dynamic process,so timely measurement is necessary.
4.3.Strengths and limitations
As far as we know,our study was the first to discuss the acceptance of illness among MSM living with HIV in China.This study revealed that it might be possible to improve QOL by enhancing illness acceptance.There are some limitations to our study.First,given the cross-sectional design of our study,we could not determine the causal relationship between relevant factors and acceptance of illness.However,our findings could provide lines of evidence and recommendations for future studies.Second,all participants in our study were below 60 years old.The factors that influenced the acceptance of illness among MSM living with HIV over 60 years need further investigation.Third,the participants were recruited from an HIV clinic in Changsha,limiting the generalizability of the results.
5.Conclusions
Chinese MSM living with HIV had a moderate level of HIV acceptance.In this population,acceptance of illness and QOL were correlated,consistent with the findings for different populations.Education level,threat,and controllability appraisals were significantly associated with acceptance.Acceptance of illness helps patients to live a normal life despite their disease-related restrictions and limitations.Future studies could design interventions that promote patients’acceptance level and help them restore normalcy and functions.
Declaration of competing interest
The authors have declared no conflict of interest.
Funding
Nothing to declare.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
CRediT authorship contribution statement
Chang Gao:Conceptualization,Methodology,Data curation,Formal analysis,Investigation,Writing -original draft,Writing -review &editing.Xueling Xiao:Conceptualization,Methodology,Data curation,Formal analysis,Writing -original draft,Writing -review&editing.Li Zhang:Investigation.Hehua Xu:Investigation.Min Wang:Conceptualization,Methodology,Resources,Supervision,Writing -review &editing.Honghong Wang:Conceptualization,Methodology,Resources,Supervision,Writing -review &editing.
Acknowledgments
The authors thank the staff members of the HIV clinic and all the participants in this study for their support.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.05.001.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of white noise on procedural pain-related cortical response and pain score in neonates:A randomized controlled trial
- Preventive strategies for feeding intolerance among patients withsevere traumatic brain injury:A cross-sectional survey
- Effects of multidisciplinary exercise management on patients after percutaneous coronary intervention:A randomized controlled study
- Implementation strategies to improve evidence-based practice for post-stroke dysphagia identification and management:A before-andafter study
- Development and validation of a rapid psychosocial well-being screening tool in patients with metastatic breast cancer
- Implementation and evaluation of the peer-training program for village health volunteers to improve chronic disease management among older adults in rural Thailand