Effects of multidisciplinary exercise management on patients after percutaneous coronary intervention:A randomized controlled study
2022-07-31JieShiYuLiuTongTongJingHongRuZhngTieYingShi
Y-Jie Shi ,Yu Liu ,Tong-Tong Jing ,Hong-Ru Zhng ,Tie-Ying Shi ,*
a Department of Nursing,The First Affiliated Hospital of Dalian Medical University,Dalian,China
b School of Nursing,Capital Medical University,Beijing,China
Keywords:Coronary disease Exercise Exercise tolerance Mobile applications Percutaneous coronary intervention Self efficacy Social support
ABSTRACT Objectives:To explore the effectiveness of the mobile app-based multidisciplinary exercise management on patients who receive percutaneous coronary intervention (PCI).Methods:From January to October 2020,54 patients after PCI were randomly assigned to the intervention group (n=27) and the control group (n=27).The intervention group received the mobile app-based multidisciplinary exercise management,whereas the control group received routine care.The patients after PCI began to take intervention one month after the operation,and the intervention lasted for two months.Before and after the intervention,6-Minute Walking Distance was used to evaluate the patient’s exercise tolerance,and the patient’s exercise compliance was evaluated according to the patient’s exercise status recorded by the mobile app.The cognitive questionnaire on knowledge about PCI treatment for Coronary Heart Disease,the Self-efficacy for Chronic Disease Scale and the Perceived Social Support Scale were used to evaluate patients’disease-related cognition,self-efficacy and perception of social support.This study was registered on Clinical Trials.gov with registration number ChiCTR2000028930.Results:Totally 51 patients after PCI who completed this study(25 patients in the intervention group and 26 patients in the control group) were included in the analysis.After 2 months of intervention,the exercise compliance of patients in the intervention group was better than that in the control group.And 6-Minute Walking Distance (469.36 ± 57.48 vs.432.81 ± 67.09),and the scores of knowledge of PCI treatment for coronary heart disease (52.64 ± 9.82 vs.42.42 ± 8.54),Self-efficacy for Chronic Disease Scale(42.40±8.04 vs.36.88±7.73)and Perceived Social Support Scale(74.04±5.73 vs.66.69±6.86)in the intervention group were higher than those in the control group with statistical significance(P <0.05).Conclusions:The multidisciplinary exercise management based on the mobile app can effectively improve exercise tolerance,exercise compliance,disease-related cognition,self-efficacy,and perception of social support during exercise training for patients after PCI.
What is known?
● Exercise-based cardiac rehabilitation has been well studied,and current international guidelines strongly recommend exercise-based cardiac rehabilitation to improve health outcomes and manage modifiable risk factors after PCI.
What is new?
● The multidisciplinary exercise management based on the mobile app is an effective intervention for patients after PCI.Nurses play an important role in the process.
● In this study,the mobile app was used to timely and objectively reflect the exercise status of patients,which not only ensures the safety of patients’ exercise in the rehabilitation stage outside the hospital,but also ensures the objectivity of the data collected in the experiment.
1.Introduction
1.1.Background and literature review
Coronary heart disease (CHD) refers to the accumulation of plaque in the coronary arteries,which restricts the blood perfusion of the heart [1].CHD is still one of the main causes of death and disability worldwide and places a huge economic burden on society[2].According to the WHO,the death rate attributable to CHD was 7.4 million in 2015 [3].In China,CHD affects more than 11 million people and is still one of the leading causes of death[4].Therefore,CHD has become a major burden for both the global and Chinese public health.The recommended treatments for CHD are percutaneous coronary intervention(PCI)and long-term drug therapy[5].Although PCI is very effective in reducing discomfort symptoms and improving prognosis,patients continue to live with chronic heart disease and may experience complications,including restenosis in the stent,adverse cardiac events,and even death.Therefore,these patients still contend with high morbidity,mortality,rehospitalization rates,and increased medical expenses.Exercise-based cardiac rehabilitation (CR) has been well studied,and current international guidelines strongly recommend CR to improve health outcomes and manage modifiable risk factors after PCI[6,7].The benefits associated with exercise-based CR include a reduction in mortality by 20-47%,a reduction in rehospitalization by 18%,improved physical activity,reduced cardiovascular risk factors,and improved quality of life [8-10].However,the prevalence of physical inactivity after PCI is high,and patient compliance with CR is around 30% [11].Thus,it is very important to develop effective exercise management strategies for patients who undergo PCI.The CR team is a multidisciplinary assistance team composed of cardiologists,nurses,rehabilitation specialists,dietitians,pharmacists,psychological counselors,and other healthcare professionals.Nurses coordinate the multidisciplinary team members,arrange reasonable rehabilitation programs for patients,and also assist with exercise,nutrition prescriptions,and medication orders from rehabilitation specialists,dietitians,and pharmacists,thereby playing a connecting role in the cardiac rehabilitation team.Nurses are the primary personnel for cardiovascular care and play a key role in fostering a healthy lifestyle and reducing cardiovascular risk factors [12].Nurse-led management interventions have been reported to improve cardiovascular risk factors,such as systolic blood pressure and triglycerides,patient self-efficacy,and quality of life and are highly feasible,acceptable,and effective.Nurses are most suited to manage the behavior of patients after PCI and coordinate with other medical staff to promote changes in exercise behaviors.
Many studies have shown that health intervention can change the exercise behavior of patients after PCI.A research panel composed of exercise experts and dietitians conducted up to five face-to-face interviews with patients who underwent PCI,mainly related to exercise and nutrition.The results showed that compared with non-recipients,the exercise and cholesterol levels of intervention recipients were improved [13].A patient-centered Web application was provided to patients with CHD to share data with medical staff (cardiologist,psychologist,general practitioner,or informal carers)and engage in video counseling so the medical staff could help patients adjust their rehabilitation goals in real-time,perform supervisory training,and other activities.The results showed similar rehabilitation effects and better rehabilitation behavior among patients that used the application compared to those that underwent standard rehabilitation management in cardiac rehabilitation centers [14].Although these studies have achieved good results through the role of multidisciplinary teams,the role of nurses in multidisciplinary teams is not well reflected.
The Information-Motivation-Behavioral Skills (IMB) model was first proposed in 1992.It includes three factors:information,motivation,and behavioral skills,all of which are necessary to engage in specific health behaviors [15].Motivation is defined as the combined effect of personal motivation and social motivation.Behavioral skills include individual self-efficacy and the objective skills to perform a certain behavior[16].Information is the basis of behavioral change.Motivation factors are the driving forces for behavioral change while behavioral skills are direct factors that influence behavioral change.The IMB model was first applied to high-risk groups such as individuals with AIDS and was subsequently applied to people with chronic diseases such as diabetes[17].This model is especially used as a framework for interventions focused on self-care behavior and risk prevention [18].Therefore,the IMB model can be used to explain factors that affect healthy behavior.However,according to our literature review,the application of the IMB model in multidisciplinary exercise management has not been reported.It is necessary to investigate whether this model can help guide the exercise behavior of patients in multidisciplinary exercise management programs.Previous studies have shown that low levels of disease-related cognition,self-efficacy,and social support for the disease can lead to poor exercise rehabilitation behavior [19,20].Moreover,there is an interaction between disease-related cognition,self-efficacy,and social support.Zarani[21]demonstrated that IMB model-based intervention plays a significant role in promoting treatment compliance and changing the lifestyle of patients after coronary artery bypass grafting.In China,Yuan [22] applied the IMB model to conduct lifestyle intervention for patients with chronic heart failure for 6 months,and the results showed that IMB model-based intervention could improve the lifestyle of patients and thus their quality of life.Therefore,using the IMB model,we selected disease-related cognition as the knowledge factor for this project,with the perception of social support as the motivation factor,self-efficacy as the behavioral skill,and exercise tolerance and exercise compliance as the outcomes of behavior change.The theoretical framework for this research is presented in Fig.1.This study was designed to explore the effectiveness of multidisciplinary exercise management on the results of exercise training for patients after PCI,and the results are expected to be beneficial for standardizing exercise management.
1.2.Research purpose
The aim of the study was to determine whether participants who received multidisciplinary exercise management would show greater improvements in exercise capacity,exercise compliance,disease-related cognition,self-efficacy,and perceived social support compared with those that received routine care.
2.Methods
2.1.Study design and setting
This study was designed as a single-blind randomized controlled trial,comparing the effects in the intervention group(IG) and the control group (CG),and was conducted in a Class A tertiary hospital in China during the period from January to October 2020.A Class A tertiary hospital is a relatively high-level hospital in China.The hospital has a cardiology department and a cardiology rehabilitation department,ensuring that the study had enough patients after PCI for a sufficient sample size.
2.2.Participants
Potential participants were screened and contacted by telephone,then patients were recruited in the outpatient department of the hospital.The inclusion criteria were:(a) meeting the PCI indications in the Guidelines for Percutaneous Coronary Intervention Therapy in China [23];(b) undergoing PCI for the first time successfully;(c)the cardiac function according to the New York Heart Association classification was in grades I-II;(d)age ≥18 years old;(e) ability to cooperate actively;and (f) informed consent and voluntary participation in this study.Participants were excluded if they (a) had other serious diseases,such as thrombotic diseases;and (b) were suffering from mental illness or had a personal or family history of mental illness.
A study explored the effects of early progressive exercise rehabilitation on the exercise performance of patients undergoing PCI after acute myocardial infarction[24].The results showed that the 6-min walk distance for the CG was 452.1±111.2 m,and that of the IG was 519.7±79.3 m.According to the sample size two-sided test calculation formula:N=(Zα+Zβ)2× 2σ2/δ2,where σ is the estimated standard deviation (SD),δ is the mean difference between two groups,α is the significance level,and β is the power of the test.We set α=0.05 and test power 1-β as 0.80 to yield Zα=1.96 and Zβ=0.84.We set n1=n2=22,considering a 20%dropout rate,and a sample size of 27 in each group was required.A random number table was used to assign a random number to each patient who met the criteria according to the order or recruitment.The patients with an odd random number were allocated to the IG and those with an even random number to the CG.Finally,there were 27 patients in each group.The IG received multidisciplinary exercise management,while the CG received routine care.
2.3.Study intervention
2.3.1.Intervention group
Four patients who met the standard for PCI were selected for the pre-experiment assessment and intervention measurement modification.Patients in the IG received multidisciplinary exercise management besides routine care.Patients in the IG received the exercise management intervention for two months,from one to three months after PCI.
2.3.1.1.Creating a nurse-led multidisciplinary exercise management team.The multidisciplinary exercise management team consisted of two nurses (one cardiac rehabilitation nurse,one exercise manager),one cardiac rehabilitation doctor,one rehabilitation therapist,one psychotherapist,and one computing engineer.The cardiac rehabilitation nurse had professional qualifications for cardiovascular nursing and was responsible for the coordination of the multidisciplinary sports management team,the consultation and guidance of patients,and the assistance of exercise managers in the exercise management of patients.The exercise manager was responsible for guiding,supervising,managing,and collecting data on the exercise training of patients in the IG.The cardiac rehabilitation doctor was responsible for disease assessment,rehabilitation guidance,and health education and consultation.The rehabilitation therapist was responsible for the formulation,modification,consultation,and guidance regarding the exercise regimens.The psychotherapist was responsible for providing advice and guidance regarding psychological confusion and anxiety.The computer engineer was responsible for maintaining the software platform used during the intervention and dealing with related problems.
2.3.1.2.Pre-implementation preparation.Cardiac rehabilitation nurses and exercise managers received training in the use of remote ECG monitoring equipment and the mobile app to ensure that they were familiar with the instructions for the exercise management of patients using the equipment.The specific training details included the composition and use of remote ECG monitoring equipment,the practical utilization of the mobile app,and potential problems and their solutions.The training method was explained through a PowerPoint presentation and practical demonstrations.The cardiac rehabilitation nurse and researchers took unified assessments involving theoretical and practical applications at the end of the training period and scored greater than 90 points out of 100 in the theoretical and practical assessments before they conducted exercise management.
2.3.1.3.Exercise management.The exercise management mainly included individual mobile app guidance,individual remote exercise monitoring,reminders,health education,and individual counseling.
Mobile app for patient exercise guidance and monitoring.The researchers instructed and demonstrated the remote ECG monitoring equipment and the corresponding mobile app to the patients until the patients could complete the process independently and operate the app smoothly.The details are summarized as follows.1) After the patient was re-examined in the cardiac rehabilitation department for a cardiopulmonary exercise test one month after the PCI,the patient installed the mobile app and registered an account under the guidance of the researcher.The researcher guided the patient to add each member of the multidisciplinary exercise management team as friends and taught the patient how to use the mobile app to communicate with the team members online and in real-time.2) The researcher input the exercise regimen prescribed for the patient after the cardiopulmonary exercise test into the mobile app and taught the patient to use the remote ECG monitoring device and the specific operation flow of the mobile app until the patient could operate the app independently.3)The researcher also taught the patient to use the mobile app to record their exercise and blood pressure to generate a diary automatically.
Individual remote exercise monitoring and reminder.1) Patients wore the remote ECG monitoring device while exercising,and the researchers could receive dynamic ECG data during the exercise session.If an abnormality wave was found,the cardiac rehabilitation doctor could be notified in time for further resolution.The researchers could also monitor the overall movements of the patient.The app could be used to coordinate and communicate with patients and rehabilitation therapists in time to promote the completion of the exercise regimen.2) Researchers set daily exercise reminders for patients through the mobile app,and patients’daily exercise could be monitored.After each exercise,the mobile app automatically recorded the exercise details and generated corresponding exercise reports.Patients could learn about their exercise progress through the intuitive reports,and researchers could determine their exercise compliance in this manner.3) The researchers summarized the exercise status of all patients in a form once a week and share the data in the patient group to help patients understand their overall exercise situation,encourage them to communicate with each other,and promote the improvement of exercise compliance.
Health education and individual counseling.1) A communication group was established,including various members from the multidisciplinary exercise management group and patients.The researchers released relevant disease knowledge to the patients through the platform and provided timely guidance and assistance.2) The researchers followed up with the patients through the mobile app every week,mainly to help patients identify possible obstacles,offer guidance,and encourage them to promote exercise behavior.Further,the researchers also encouraged patients to communicate with nurses or the corresponding team members individually through the mobile app if they had any questions or concerns,and provided the corresponding individual guidance and help.The researchers would also help patients get professional responses from the team members if necessary.
2.3.2.Control group
Participants allocated to the CG received routine care.A cardiopulmonary exercise test(CPET)was performed on patients who visited the outpatient department of the hospital for reexamination one month after PCI.According to the results of the test,rehabilitation doctors prescribed exercise regimens suitable for the condition of each patient.The prescribed exercise regimen included details on the intensity,frequency,time,exercise type,and exercise precautions.The patients were instructed to visit the outpatient department for re-examination at the end of the third month after the PCI.During this period,the nurses followed up on the patients’exercise plans by telephone once a month according to a unified outline and offered advice on the difficulties encountered by the patients in the process of implementing the exercise plan.Patients were encouraged to find solutions to the problems that they encountered to enhance their confidence in performing the exercise.
2.4.Measurements
2.4.1.General demographic characteristics
The general demographic characteristics were collected at the baseline using a questionnaire,including age,sex,marital status,place of residence,education level,occupation,family income,medical payment method,smoking and drinking status,and whether the patient had other chronic diseases or a family history of CHD.
2.4.2.6-Minute Walking Distance (6MWT)
This outcome was used to evaluate the cardiopulmonary function of patients with cardiovascular disease and to predict their maximum exercise tolerance.The 6MWT was performed following the protocol recommended by the American Thoracic Society(ATS)guidelines to assess the patient’s exercise tolerance[25].According to the requirements of the experiment,patients walk continuously in a horizontal closed corridor with a straight-line length of 25 m,and complete as much ground distance as possible in 6 min [26].Exercise tolerance is quantified by walking distance,with longer distances indicating higher exercise tolerance.
2.4.3.Exercise compliance
A total weekly exercise time of 80% or more of the minimum recommended weekly exercise time is considered good compliance,50%-80% is partially compliant,and less than 50% is noncompliant [27,28].In this study,a remote ECG monitoring device and mobile app were used to record patients’ exercise frequency and exercise time.Researchers could know the patient’s exercise time intuitively through the mobile app.
2.4.4.Cognitive questionnaire on knowledge about PCI treatment for CHD
The disease cognition of CHD patients after PCI was assessed using a questionnaire developed by Chinese scholars [29].The questionnaire consisted of 14 questions.Each question was multiple-choice,and each option was assigned 1 point,with a total score of 70 points.Higher scores indicated higher levels of cognition.The questionnaire had good reliability and validity.The Cronbach’s α coefficient and content validity of the questionnaire were 0.912 and 0.924,respectively.
2.4.5.Self-efficacy for Chronic Disease Scale (SECDS)
The SECDS was compiled in 1996 to reflect the self-efficacy of patients with chronic diseases in many aspects [30].The scale contains six items divided into two dimensions:confidence in controlling symptoms and maintaining functions.The total mean score ranges from 1 (not at all confident) to 10 (totally confident),with higher scores indicating higher self-efficacy.A score of 1-3 indicates low self-efficacy,a score of 4-7 indicates medium selfefficacy,and a score of 8-10 indicates a high level of self-efficacy.The SECDS has been used to assess the self-efficacy of patients with CHD and was found to be reliable with a Cronbach’s α coefficient of 0.91 [31].
2.4.6.Perceived Social Support Scale (PSSS)
PSSS was compiled by Zimet et al.to assess the various social support sources recognized by research participants[32].The scale contains 12 items divided into three dimensions:family support,friend support,and other support.The scale uses the 7-point Likert scoring method,with scores ranging from 17 to 84 points.A total score of 12-35 is classified as low-level social support,36-61 is classified as medium-level social support,and 62-84 is classified as high-level social support.Higher scores indicate more social support received by the patient.The Chinese PSSS has been used among Chinese patients and shows good reliability [33,34].
2.5.Date collection procedure
The investigator collected the general demographic characteristics at baseline (one month after the PCI,T1).A set of questionnaires,including the cognitive questionnaire on knowledge about PCI treatment for CHD,the SECDS and the PSSS were used to collect data at T1 and three months after the PCI(T2).Patients’6MWD and exercise compliance were evaluated at T1 and T2.
2.6.Date analysis
In this study,SPSS 24.0 was used for data sorting and analysis,and P <0.05 was considered statistically significant.In the descriptive statistical analysis of the data,the count data were presented as the frequency and composition ratio (%),and the measurement data were presented as the mean and standard deviation.The two independent sample t-test,and the chi-square test were used to compare the data between the two groups.
2.7.Ethical approval
This study was approved by the Institute's Hospital Ethics Committee (PJ-KY-2019-137) and was conducted following the ethical standards of the Declaration of Helsinki.The research report followed the Consort 2010 statement [35].All patients were informed of the study procedures and provided informed consent before being included in the study.In addition,this study was registered on Clinical Trials.gov with registration number ChiCTR2000028930.
3.Results
3.1.Study flowchart
Sixty-eight patients undergoing PCI were evaluated for this study.Among them,14 patients were excluded,and 54 participated in this study,with 27 in the IG and 27 in the CG.Fifty-one patients complete the study and were included in the analysis.No adverse reactions occurred during the study process.The flowchart of the study is shown in Fig.2.
3.2.Comparison of baseline data between the two groups
The general demographic characteristics of the 51 participants at baseline are shown in Table 1.There was no statistically significant difference between the two groups in general demographic characteristics(P>0.05).Table 2 shows the comparison of 6MWD,exercise compliance,and scores of the cognitive questionnaire on knowledge about PCI treatment for CHD,SECDS,and PSSS.There were no significant differences between the two groups at baseline(P >0.05).
3.3.Comparison of outcomes between the two groups
Table 3shows that the proportion of patients with high exercise compliance in the IG was more than that in the CG,and results of 6MWD,scores of the knowledge of PCI treatment for CHD,the SECDS,and the PSSS in the IG were higher than those in the CG after the intervention (P <0.05).
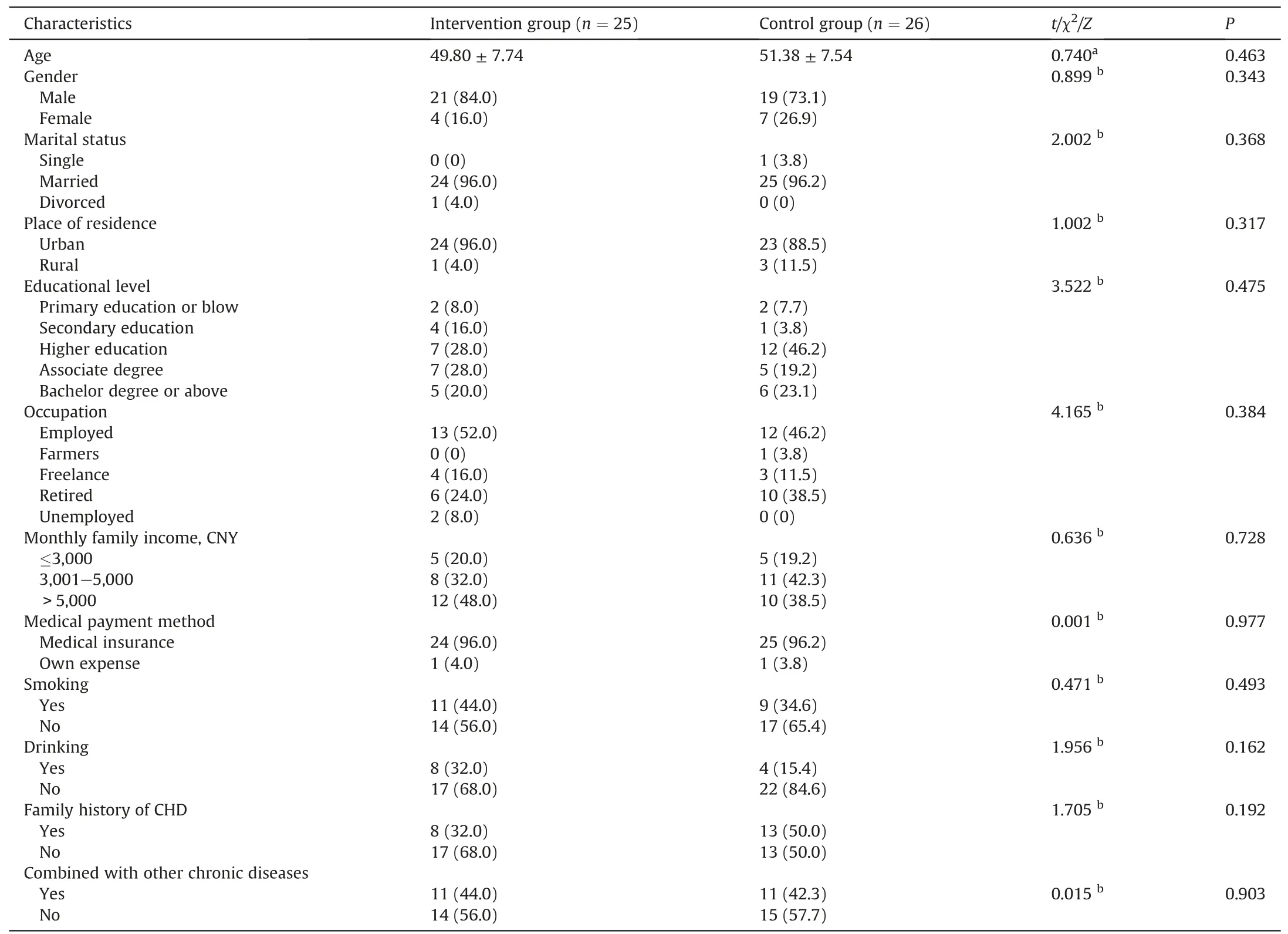
Table 1 General demographic characteristics between the two groups at baseline.
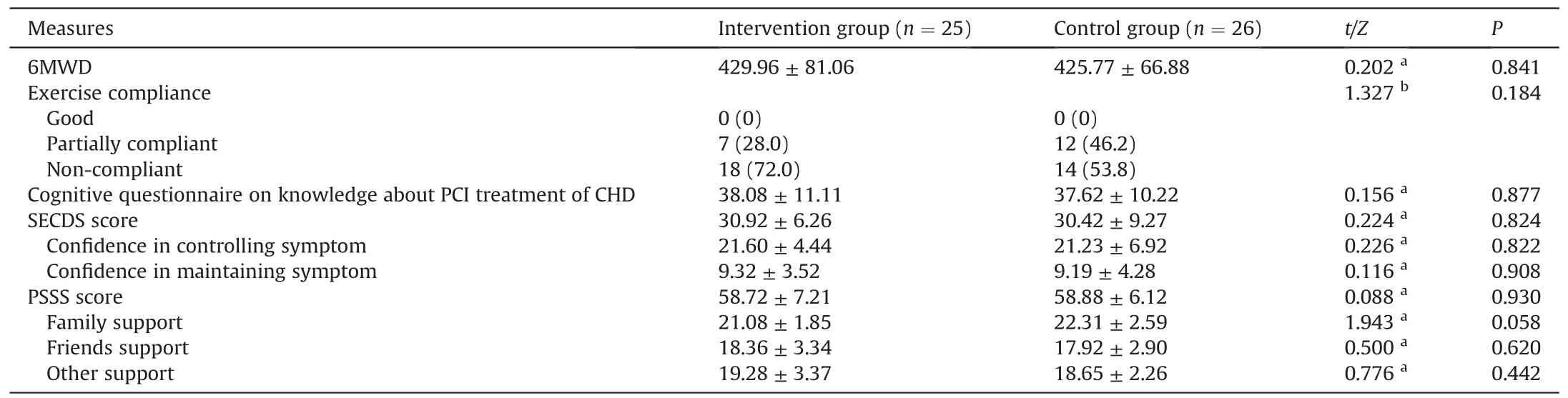
Table 2 Comparison of measurements between the two groups at baseline.
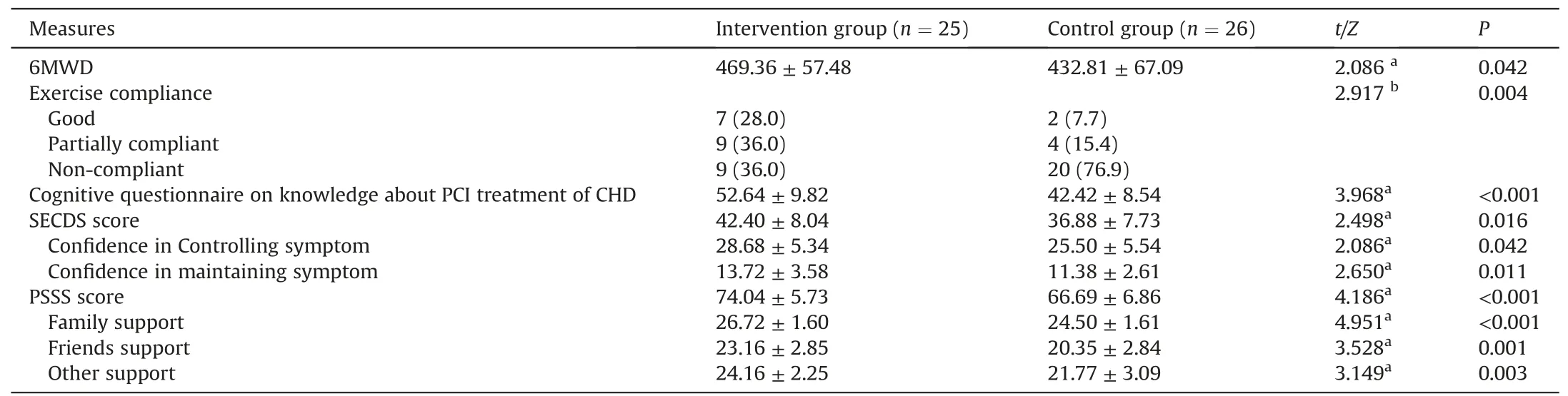
Table 3 Comparisons of outcomes between the two groups.
4.Discussion
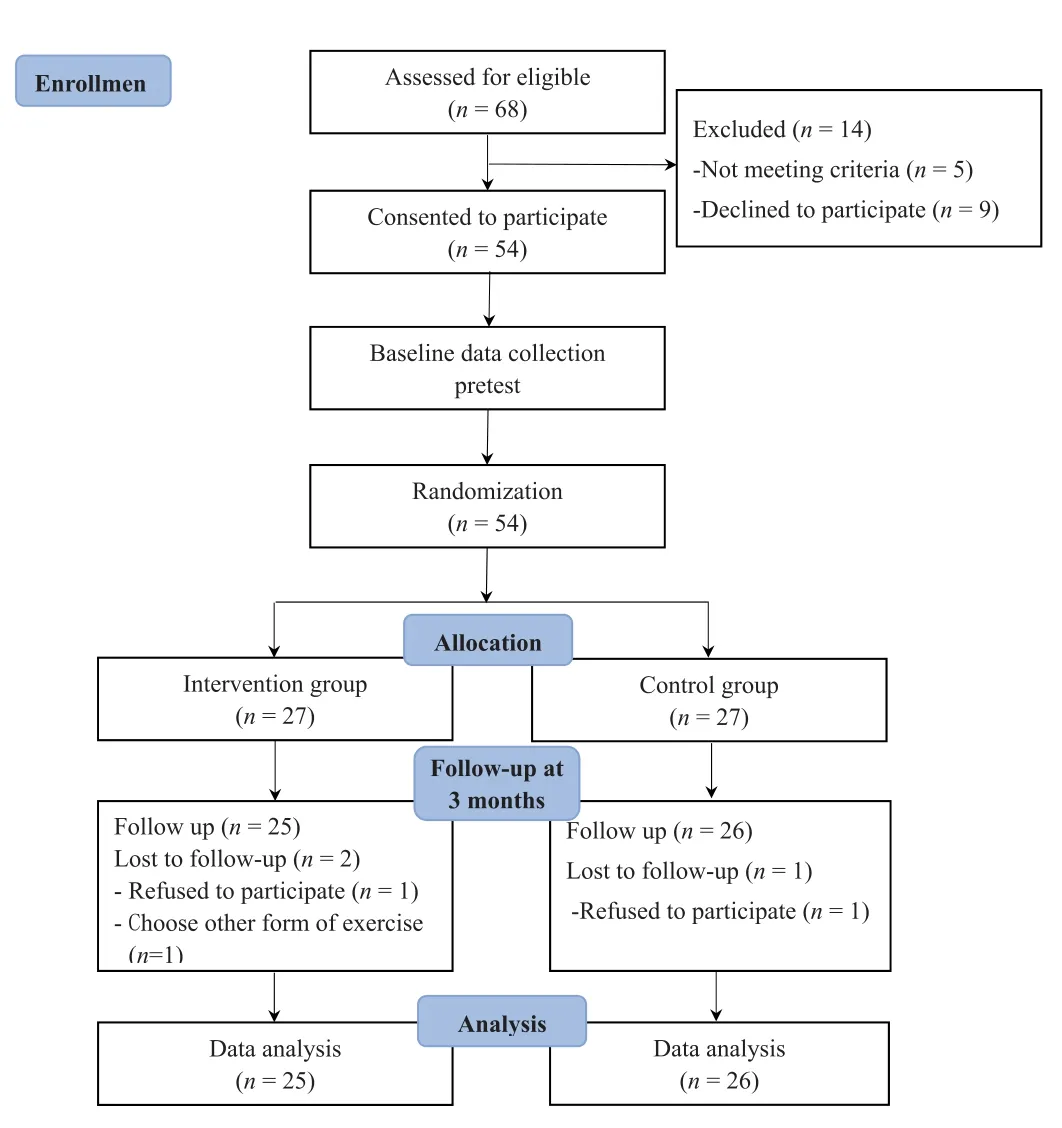
Fig.2.CONSORT flowchart of the study.
As one of the few studies on mobile app-based multidisciplinary exercise management using the IMB model after PCI,this study demonstrates the effectiveness of mobile app-based multidisciplinary exercise management in improving patients’ exercise tolerance,exercise compliance,disease-related cognition,selfefficacy,and perceived social support.
4.1.Effects of the mobile app-based multidisciplinary exercise management on exercise tolerance and compliance
In the present study,the intervention improved exercise tolerance.This finding was consistent with the results of related studies that showed improved exercise tolerance [34,36,37].The management planning method employed may explain the remarkable results.The specific details include the following.1)The intervention measures were initiated within a short period after the patients completed the operation.The patients may have felt they were at high risk and therefore were more likely to be motivated to learn and adopt healthy behaviors.2) The results may be related to the application of dominant scientific and standardized management strategies for the exercise regimen,remote monitoring to ensure reasonable safe movements and exercise intensity,and nurse supervision for sports management.The patients gradually developed clearer cognition of their exercise capacity,recognized the appropriate exercise intensity for their bodies,and avoided the negative effects of uncomfortable exercise on the body.Additionally,the patients received exercise reminders and incentive information during regular exercise sessions led and supervised by nurses and therefore gradually developed regular exercise habits in the process of limb function recovery as well as rehabilitation confidence,improving their exercise tolerance.Although research had shown that the intervention has a positive effect on exercise behavior,some patients had low compliance and further improvement of the exercise management program is necessary.Poor exercise behavior may be related to a busy work schedule and low awareness of the importance of exercise.This observation also suggested that medical staff should improve health education for patients.
4.2.Effects of the mobile app-based multidisciplinary exercise management on disease-related cognition,self-efficacy,and perceived social support
Negative attitudes regarding exercise can be corrected by providing the correct information to patients,thereby establishing healthy behaviors.Nurses continuously provided disease-related knowledge to patients and promoted further understanding of their diseases and rehabilitation process.The results of this study also showed that the intervention can improve disease-related knowledge.This may be related to the use of a mobile app platform for health management and interactive communication.In addition,the researchers took the initiative to push disease-related knowledge to patients,ensuring the patients could obtain information conveniently,which not only gradually enhanced the patients’ awareness of the disease,but also enabled them to avoid incorrect information.When the patients had any doubts or confusion,they could actively communicate with their doctors and nurses through the mobile app platform.Patients were not limited by time and space;they could obtain the correct information at any time and thereby improve their disease-related cognition.Therefore,medical support is essential to a certain extent to improve patient awareness of their disease.Moreover,the flexibility,convenience,and combination of active and passive education may also be the reason why the patients in the experimental group had higher disease-related cognition than those in the CG.Cognitive change is an intrinsic motivator of individual behavioral change when individuals realize that bad behavior has a close relationship with the occurrence and development of diseases and therefore changes their behavior [38].The results of this study confirm this point.
Self-efficacy is the ability of individuals to change their behaviors and is the basis for improving the health of patients with chronic diseases [39].Chinese patients usually rely on the physician’s suggestions for disease treatment.In this research,patients were helped and supported by nurses.Self-efficacy and selfmanagement behaviors are directly related to the medical support system.Nurses provide information to promote self-efficacy,help patients play an active role in their recovery process,and exert control over their health [40].The results are due to the following factors:first,nurses led the multidisciplinary sports exercise for patients with PCI postoperative team management,ensuring the patients received comprehensive and ongoing management and care at home.The nurses also provided reminders to the patients and used affirming language to strengthen the patient’s confidence in rehabilitation.Secondly,disease-related knowledge and instructions for attention were regularly pushed to the patients,facilitating improvements in their awareness of the disease and enhancing their confidence in overcoming the disease.Finally,patients could communicate with other patients within the communication group on the platform.Some patients with more active exercise might offer positive motivations to patients with little exercise.Consequently,the self-efficacy of the patients improved under the multidisciplinary exercise management program.
Research has shown that social support is one of the best resources for patients undergoing treatment.It helps patients maintain healthy behaviors and plays an important role in the recovery of their physical and mental state [41].The perception of social support can help improve compliance with treatment plans and provide decision-making motivation for symptom management[42].The results of this study showed that the perceived level of social support for patients in the IG was better than that in the CG.This highlights the importance of nurses being listeners.When patients have doubts or negative emotions,nurses can listen,help them analyze the situation,and offer suggestions in time.In addition,the researchers pushed disease-related information to the patients,which not only improved their cognition of the disease,but also promoted communication,such that the patients could effectively express their emotions and solve any problems they encountered.Patients also recognized the sincere help from the nurses,which promoted their understanding of the social support level.Additionally,the platform communication groups promoted communication between patients.The patients could personally experience sincere and friendly help from others,which elevated their perception of the social support level and promoted changes in their health behaviors.Therefore,the level of perceived social support for the patients in the IG was higher.
4.3.Limitations
The study had some limitations.First,the general demographic characteristics collected in this study did not include height,weight,and other indicators,which may lead to some bias.Secondly,this study only studied the short-term effect of this intervention on out-of-hospital cardiac rehabilitation of patients after PCI,and lack of observation on the effect of early exercise management intervention and long-term intervention in patients after PCI.Thirdly,all participants were recruited from one hospital.Differences in the customs and lifestyles of the participants should be taken into consideration when the research results are extended to other populations.
5.Conclusion
The mobile app-based multidisciplinary exercise management is an effective intervention to improve patients’ exercise behavior and tolerance,knowledge of the disease,self-efficacy,and perceived social support.The results also show that nurses play an important role in the whole team,such as establishing a cooperative relationship with patients to promote patients' exercise behavior and coordinating the multidisciplinary team members.Hence the team members work together to achieve better results.In future studies,we need to expand the sample size and prolong the study time to further confirm the effectiveness of the intervention measures.We also recommend that nurses apply this method of exercise management in routine care for patients after PCI to improve their exercise behaviors.
CRediT authorship contribution statement
Ya-Jie Shi:Conceptualization,Methodology,Validation,Formal analysis,Data curation,Writing-original draft,Writing-review&editing,Project administration.Yu Liu:Conceptualization,Methodology,Validation,Formal analysis,Writing -review &editing.Tong-Tong Jiang:Conceptualization,Methodology,Validation,Formal analysis,Writing -review &editing.Hong-Ru Zhang:Conceptualization,Methodology,Validation,Writing -review &editing,Project administration.Tie-Ying Shi:Conceptualization,Funding acquisition,Writing -review &editing,Supervision,Project administration.
Funding
This study was provided by The Scientific Reuter Foundation of Liaoning Provincial Education Department,China (grant no.LZ2020039).
Data availability statement
The datasets in the current study are available from the corresponding author on reasonable request.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
We would also like to express our gratitude to the patients,nurses and doctors in the Cardiac Rehabilitation Center of the First Affiliated Hospital of Dalian Medical University.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.06.012.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of white noise on procedural pain-related cortical response and pain score in neonates:A randomized controlled trial
- Preventive strategies for feeding intolerance among patients withsevere traumatic brain injury:A cross-sectional survey
- Implementation strategies to improve evidence-based practice for post-stroke dysphagia identification and management:A before-andafter study
- Development and validation of a rapid psychosocial well-being screening tool in patients with metastatic breast cancer
- The relationship between acceptance of illness and quality of life among men who have sex with men living with human immunodeficiency virus:A cross-sectional study
- Implementation and evaluation of the peer-training program for village health volunteers to improve chronic disease management among older adults in rural Thailand