Clinical leadership behaviors among critical care nurses in private and governmental hospital:A cross-sectional survey
2022-07-31HebMohmedAlAnwerAshourMrmAhmedBnkhrNglAbdElzizElseesy
Heb Mohmed Al Anwer Ashour ,Mrm Ahmed Bnkhr ,Ngl Abd Elziz Elseesy
a Nursing Administration Department,Faculty of Nursing,Alexandria University,Alexandria,Egypt
b Department of Public Health Nursing,Faculty of Nursing,King Abdulaziz University,Jeddah,Saudi Arabia
Keywords:Behavior Cross-sectional studies Intensive care units Leadership Nurses
ABSTRACT Objectives:This study aimed to investigate clinical leadership behaviors among critical care nurses and compare the differences between nurses in private and public hospitals.Methods:A cross-sectional survey including 365 critical care nurses with a bachelor’s degree in nursing science were recruited in two Egyptian hospitals (a government teaching hospital and one private hospital) from January to March 2019.A socio-demographic characteristics form and the Clinical Leadership Behaviors Questionnaire (CLB-Q) were used to collect data.For comparison and analysis,the mean score was calculated and converted to a percentage value.Results:Results showed that the overall mean score of nurses’ clinical leadership behaviors was 77.11 ± 11.87,the level was higher,and the highest score of the communication dimension was 91.84 ± 7.38.The mean score of nurses at a private hospital (90.48 ± 5.53) was higher than that at a government teaching hospital(68.29±4.21)(P<0.001).On nursing experience,nurses with 5-10 years had higher mean score in self-awareness,advocacy and empowerment,decision making,quality and safety,teamwork,and clinical excellence dimension of clinical leadership behavior than those who worked less than 5 years or more than 10 years (P <0.01).Single nurses had higher mean score in advocacy and empowerment,decision making,quality and safety,and clinical excellence dimension of clinical leadership behavior than those who married (P <0.01).Conclusions:Nurse managers should foster clinical leadership by enabling critical care nurses to practice clinical excellence and encouraging their attendance in training programs on quality and safety.Nurses in government hospitals need improvement in clinical leadership behaviors regarding all dimensions.
What is known?
● The importance of clinical leadership is emphasized in health systems worldwide.
● Clinical leadership is a relatively new term and may still be misunderstood.
● The terms “nursing leadership” and “nursing management”are often confused.
What is new?
● This cross-sectional study investigated clinical leadership behaviors among nurses in two different health sectors--private and governmental hospitals-revealing differences between them in clinical leadership dimensions such as selfawareness,advocacy and empowerment,decision-making,communication,quality and safety,teamwork,and clinical excellence.
● Based on the study findings,we highlight the importance of establishing clinical leadership development interventions in all areas of nursing practice and developing clinical leadership programs in healthcare systems.
1.Introduction
Clinical leadership is defined as nurses’ behaviors that provide direction and support for clients and the healthcare team in the delivery of patient care [1].Clinical leadership can have a positive effect on not only clinical practice but also the clinical care atmosphere,contributing to safe,quality patient care;job satisfaction;and the preservation of frontline healthcare providers [2].Therefore,nurses require research-based knowledge on the implementation of clinical leadership behaviors [3].
Many studies were designed and conducted to investigate clinical leadership as a concept,and healthcare professionals(excluding nurses and doctors) have applied clinical leadership to improve services and adopt quality initiatives [4] in terms of recognizing and defining clinical nurse leaders [5],understanding doctors’ perspective on clinical leadership [6],and examining the meaning of leadership at the bedside [7,8].
On the other hand,some studies link nurses’clinical leadership to patient care quality [9],while another study focused on clinical leadership and effective nursing teams [10] by examining the psychological and structural empowerment and clinical leadership of nurses who work in emergency departments.Factors that support and inhibit nurses’ clinical leadership abilities have also been investigated [11].
Other related studies focused on the background,lived experience,values,vision,beliefs,and the importance of clinical leadership such as antecedents of clinical leadership and pre-registration nursing education [12],as well as on the impact of clinical leadership on the hospital setting [13,14].The various ways nurses can adopt clinical leadership to develop patient awareness and engagement subsequently leading to the promotion of selfmanagement,clinical leadership,values,beliefs,and vision have also been highlighted [15,16].
Internationally,several projects have targeted clinical leadership such as the Clinical Leadership Pilot Evaluation Report[17]and the Clinical Leadership Competency Framework [18].Another project examined the strengths and drawbacks of clinical leadership for the improvement of service quality,productivity,and innovation[19].Furthermore,clinical leadership can be regarded as a framework for action and a guide for senior leaders to develop professional diversity on a large scale [20].
Evidentially,a review of the literature sought to determine the development and evaluation of clinical leadership interventions for frontline healthcare providers [21].In Ireland,as part of the data collection,the National Clinical Leadership Development Project’s pilot evaluation was performed by the University College Dublin(UCD).School of Nursing,Midwifery&Health Systems on behalf of the Office of the Nursing and Midwifery Services Director in 2012[22].Health and Safety Executive (HSE) published clinical leadership behaviors,based on seven clinical leadership competencies,including self-awareness,advocacy and empowerment,communication,quality and safety,decision making,teamwork,and clinical excellence.The National Clinical Leadership Development Framework especially aimed to help nurses and midwives,at all levels of proficiency,advance their clinical leadership skills.
Self-rating clinical leadership behaviors in association with the seven clinical leadership skills suggested that participants were rating themselves as frequently engaged in the leadership behaviors.The most highly rated behaviors included skills associated with decision-making.Insignificant differences were observed in the self-rating of managerial and non-managerial positions as senior and junior grades,respectively[22].
Professional nurses are responsible for and supervise patients’care,while personally managing the delivery of safe patient care.They undertake an informal leadership role not related to specific positions.This role is not prescribed or scripted;rather,the actors involved have adopted this role through negotiations that are somehow subject to others’ expectations.Moreover,patients expect professional nurses to lead the nursing teams that provide care to them.Effective leadership is now not only essential but also a challenge to professional nurses in times of diminishing resources,inadequate quality of care,and a growing number of medical injuries [2].
Critical care services are designed to help patients in an emergency or life-threatening health condition,where vital organs are at risk of failure.Critical care aims to maintain the normal functioning of organs and improve the patients’ condition so that their underlying injury or illness can be treated using advanced therapeutic,monitoring,and diagnostic technologies [23].
Clinical leadership is critical in all critical care units because of their dynamic nature,which stems from the admitted patients’severe conditions,unpredictable clinical care,rapid overturn in patients,aggressive treatment of patients on the verge of death,and the need for critical care nurses to provide highly complex care.Positive clinical role models,empowered decision-makers,clinically competent,and good communicators are all attributes of staff nurse clinical leaders.Nurses must have crucial clinical leadership abilities in this context to obtain the best results,increase the efficiency and sustainability of care processes that benefit the healthcare team,and provide good patient care.
Developing and measuring clinical leadership behaviors among professional nurses is of serious significance.However,not much is known regarding these behaviors among Egyptian nurses who are supposed to be future leaders working in critical care units.They are also in charge of evening and night shift nurses in both government and private hospitals.Therefore,this study could help assess critical care units’ professional nurses’ clinical leadership.This is a novel study conducted in the context of Egyptian nurses.It is hoped that this study will highlight dimensions of weakness in clinical leadership behaviors,providing fruitful areas for investigation.
Although the importance of effective clinical leadership to patient outcomes has been widely recognized,some considerable obstacles exist regarding nurses’participation in clinical leadership.Considering the emphasis on hospital performance,efficiency and quality improvement must be considered equally important[13].In this context,this study focused on quantifying clinical leadership in governmental and private institutions based on the assumption of macromanagement perspective,they exhibited differences.According to some studies,the investigators’ professional job expertise in both situations led them to this conclusion,that the management of the material,physical,and human resources,safety,and quality were different [24-26].
Hence,this study aimed to assess and compare clinical leadership behaviors among critical care nurses in private and governmental hospitals.
2.Methods
2.1.Study setting and participants
From January to March 2019,a cross-sectional survey was conducted at critical care units of two hospitals:the main university hospital (7 units),which is a teaching hospital affiliated with the University of Alexandria,and another hospital Mabret El Asafera East and West (two branches affiliated to same private hospital)(7 units),which are for-profit,private,multi-specialty hospitals with a high occupancy rate in Alexandria Governorate.The participants in the current study included all professional nurses who are working in critical care units in previously selected hospitals(n=365)classified as from the Main University Hospital(n=220)and East &West Mabret El Asafera Private Hospital (n=145).Inclusion criteria:nurses had experienced more than one year in the pre-selected hospitals,had a bachelor’s degree in nursing science,provide direct and indirect patient care,and had a willingness and eagerness to cooperate.
2.2.Measurement tool
2.2.1.Socio-demographic characteristics
Questions on the nurses’ socio-demographic characteristics(e.g.,age,gender,marital status,and experience)were included as a section in the study.
2.2.2.The clinical leadership
The Clinical Leadership Behaviors Questionnaire (CLB-Q) was developed by Fealey and colleagues (2012),which was used to collect data to measure clinical leadership behavior among bedside nurses as part of a clinical leadership education and evaluation program derived from the United Kingdom National Health Service(NHS) healthcare leadership initiatives [27].This scale has strong internal consistency reliability in previous studies[27,28].The selfreport questionnaire assesses clinical leadership behaviors.It consists of 46 items with 7 subscales,including self-awareness(n=6),decision making (n=7),advocacy and empowerment (n=6),communication (n=6),teamwork (n=6),quality and safety(n=7),and clinical excellence (n=8).Each statement was presented on a simple five-point Likert scale ranging from“rarely=1”to“always=5”and respondents were asked to rate the frequency with which they engaged in individual items.The actual scoring level of this questionnaire is ranging from 46-230.For comparison and analysis,the mean score was calculated and converted to a percentage value,with 100 as the highest score and 0 the lowest.The converted mean score range 0-33.3 indicates lower level of nurses’clinical leadership behaviors,33.4-66.6 indicates moderate level and 66.7 -100 indicates higher level.
The CLB-Q was validated among nurses and midwives during a pilot clinical leadership development program in Ireland.The Cronbach’s α coefficient for internal consistency among the subscales ranged from below acceptable to good,using the criterion of 0.70 or greater:advocacy and empowerment (0.677),communication (0.745),decision making (0.758),clinical excellence (0.810),quality and safety (0.815),self-awareness (0.829),and teamwork(0.842) [27,28].
The survey adopted in the current study did not fall under the committee’s jurisdiction because all participants were professional nurses.The CLB-Q was in English,and its content validity was verified by five experts in the same field.For reliability assessment,the Cronbach’s α coefficient was 0.959.The Cronbach’s α coefficient was determined for all instrument subscales,ranging between 0.755 and 0.912.
2.3.Data collection
A pilot study was conducted on 10% of the participants.The questionnaires were hand-delivered to staff nurses in their work setting,after an individualized interview with each nurse for about 5 min to explain the study’s goal,and instructions were given before distributing the questionnaire.Informed consent was taken from nurses before data collection.Participation in this study was voluntary and based on willingness.The participants were assured about the confidentiality of their information.The required time to fill out the questionnaires was 15-20 min.
2.4.Ethical consideration
Official approvals were obtained from the Faculty of Nursing,Alexandria University,Alexandria Main University Hospital,and the private hospital to collect data.The privacy,anonymity,and confidentiality of data were maintained and assured.We obtained participants’ informed consent to participate in the research before data collection.They had the right to withdraw from the study at any time.
2.5.Data analysis
Data were analyzed using SPSS software (version 20.0).Quantitative data were presented with numbers and percentages,mean,and standard deviation.The normal distribution of data was verified using the Kolmogorov-Smirnov test.The level of significance for the obtained results was determined at 0.05.The two studied groups were compared using an independent sample t-test for normally distributed quantitative variables.Moreover,a one-way analysis of variance (ANOVA) was adopted for normally distributed quantitative variables,to compare between more than two groups,and a post hoc test (Tukey’s using least significant difference) was used for pairwise comparisons.
3.Results
In total,375 critical care nurses completed the questionnaires between January and March 2019,with a response rate of 100%.The obtained feedback was classified based on the type of hospital--government teaching hospital (n=220) and private hospital(n=145).
The two study groups were compared according to the demographic characteristics in Table 1.The mean age of nurses was 41.05 years (SD=10.07).The majority of government teaching hospital nurses (84.5%) and private hospital nurses (82.8%) were female.Over two-thirds of the nurses working at the government teaching hospital had more than 10 years of experience,while 13.2% of nurses had between 5 and 10 years of experience.Moreover,89.5% and 76.6% of nurses who were working at the government teaching hospital and private hospitals,respectively,were married.
A comparison between the two studied groups based on clinical leadership behavior dimensions is presented in Table 2.The overall mean score of staff nurses’ clinical leadership was high(77.11 ± 11.87);they were 90.48 ± 5.53 at private hospitals and 68.29±4.21 at the government teaching hospital.However,nurses at both the government teaching hospitals and private hospitals gave the highest rating to the communication dimension(89.56±6.01 and 95.31±7.93,respectively),while private hospital nurses gave the lowest rating to the quality and safety dimension(78.21 ± 6.49) and government teaching hospital nurses gave the lowest rating to the clinical excellence dimension (51.78 ± 7.83).The obtained results reveal that private hospital nurses obtained higher mean scores for all dimensions of clinical leadership than government teaching hospital nurses did (P <0.01).
There was no difference in the comparison of clinical leadership behavior mean score among nurses of different ages and genders(P>0.05).Significant differences in the overall mean score of CLB-Q was found by experience in the current position and marital status(P <0.01).On nursing experience,nurses with 5-10 years had higher mean score in self-awareness,advocacy and empowerment,decision making,quality and safety,teamwork,and clinical excellence dimension of clinical leadership behavior than those who worked less than 5 years or more than 10 years (P <0.01).Single nurses had higher mean score in advocacy and empowerment,decision making,quality and safety,and clinical excellence dimension of clinical leadership behavior than those who married(P <0.01).(Table 3).
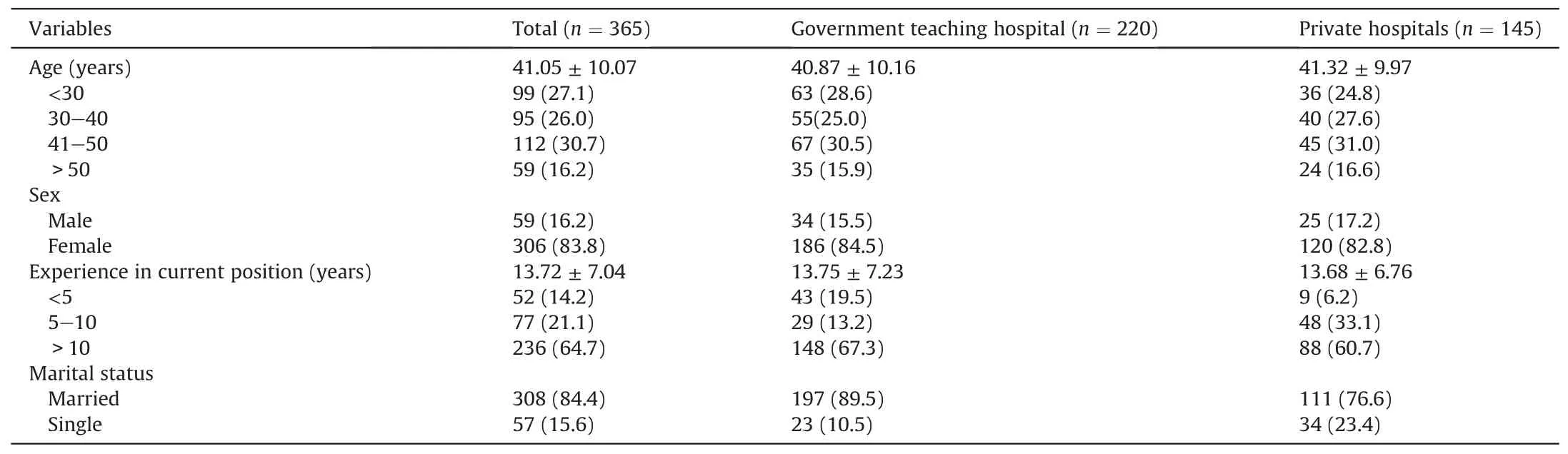
Table 1 Demographic characteristics of participants.

Table 2 Comparison of two studied groups based on clinical leadership behavior dimensions.
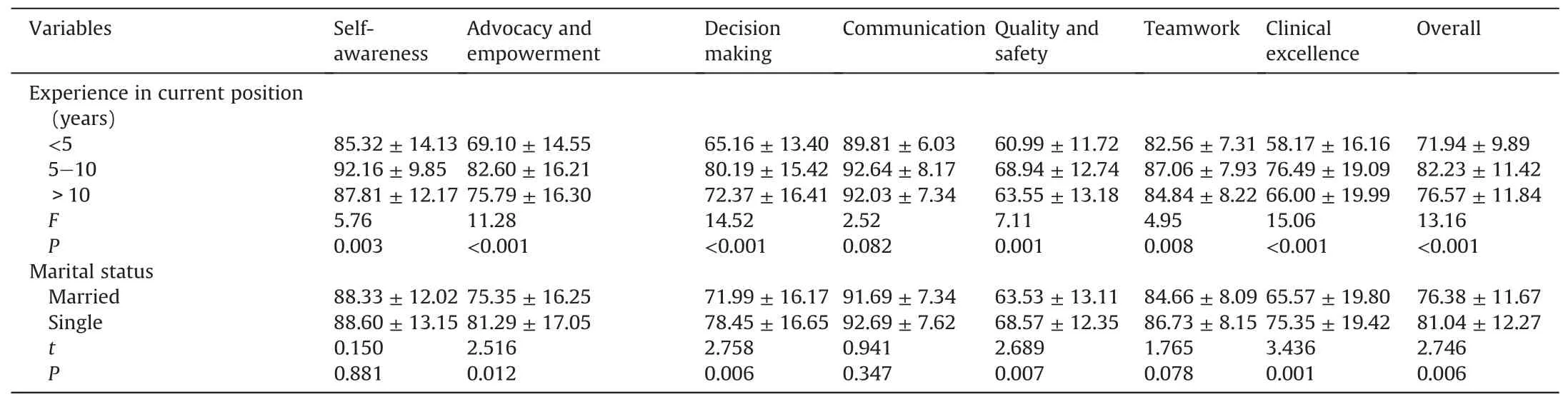
Table 3 Differences in clinical leadership by demographic (n=365).
4.Discussion
This study draws attention to the importance of the role of clinical leadership played by professional nurses through several clinical leadership behaviors such as self-awareness,advocacy,empowerment,decision-making,communication,quality and safety,teamwork,and clinical excellence.
The findings of this study reveal that the overall clinical leadership behaviors are high,which may be attributed to the wide range of aforementioned behaviors followed and reported by nurses,which are considered key competencies that develop clinical leadership behaviors.The results of the present study confirm those obtained by others [3,28-31] who reported similar findings that participants’ clinical leadership qualities were found to be at high levels in all sub-dimensions.Moreover,most nurses reported the frequent adoption of clinical leadership behaviors in a clinical setting by developing certain competencies.
Most importantly,the results revealed that the overall mean score of clinical leadership in a private hospital is more than that in a government teaching hospital.This could be attributed to enabling working factors in a private hospital that enhance nurses’clinical leadership behaviors such as nurses’ empowerment,management support,good supervisor-subordinate relationship,attention to staff training and development,and nurses’ higher autonomy.In addition,private hospitals select and recruit professional nurses based on specific criteria to deliver high standards ofclinical performance,which will be reflected not only in the hospital’s quality of care but also in its image in a competitive market.This result is supported by several studies [1,10,29,32-34],which reported that private hospitals generally provide better quality care compared to public sector hospitals.Nurses also appear to be more satisfied with their relationship with nurse supervisors,tend to be highly empowered,and are committed to their hospital while remaining financially viable and creating a positive nursing environment to support clinical leaders by encouraging independent practices.
Self-awareness had a higher mean score among private hospital nurses than among government teaching hospital nurses,which can be explained by the fact that nurses in private hospitals are supported by training programs to improve their professional and personal development,creativity,and commitment,all of which promote nurses’emotional intelligence,as reflected by their higher self-awareness.This finding is supported by a study that revealed the importance of training programs,creativity,work commitment,and performance to ensure the employees’ awareness about working together to achieve the goals of the organization.Positive behavior along with awareness is the initial phase of professional development [35].
Based on the obtained results,private hospitals had a higher level of advocacy and empowerment than the government teaching hospital did.This may be because nurses in private hospitals are more capable of perceiving patients’ and peers’ needs for support,advocating for and empowering others to meet their own needs,and supporting their colleagues to act based on the best evidence and reach the highest standard in their work.This finding was in line with a study that found a higher empowerment factor in a private hospital than in a government teaching hospital[32].It was also found that nurses’ loyalty and sense of belonging to their hospitals are greatly influenced by their understanding of empowerment [36,37].
This study found that private hospitals had the highest mean score regarding decision making because nurses in private hospitals are more willing to take decisions,a responsibility that affects patients and colleagues,and are accountable for their decisions.All these decision-making skills could be related to the management system that supports nurses.This result corresponds to several studies that revealed that the increase in self-confidence supports decision-making skills and facilitates the determination of interventions [38-40].
However,this result contradicts the findings obtained by two other studies,which reported that nurses who worked in government hospitals are more involved in decision-making than those in private hospitals are [41,42].Since private hospitals offer health services to patients who pay for them,hospital authorities do not usually involve nurses in their decision-making process.
The mean score of the communication dimension was higher among private hospital nurses than among government teaching hospital nurses.This is because there is a system for communication that improves work facilities and influences clinical leadership behaviors among nurses in private hospitals.This finding confirms the results of two previous studies,which suggested that for the majority of respondents,improvements in facilities and wage increases are essential to improve communication within their teams[43,44].
In the quality and safety behaviors dimension,private hospital nurses reported higher mean scores than nurses in the government teaching hospital did.This finding can be explained by the fact that nurses in private hospitals encourage a culture of quality and safety through their actions and collaborations with others to meet high quality and safety standards.This is in line with the findings of several studies,all of which revealed that the quality of healthcare in private hospitals was higher than that in government hospitals because private sectors focus on the needs and wishes of patients[45-47].
The mean score of private hospital nurses was higher than that of government teaching hospital nurses for the teamwork dimension.This result may be due to the small number of employees in private hospitals who can assist in creating a culture of teamwork through collaboration and celebrating team achievements.It has been consistently revealed that private hospital nurse teamwork,organizational commitment,and performance scores were higher compared to those of government hospitals [48].
In addition to clinical excellence,nurses in private hospitals reported that they are more responsible for creating clinical practice policies,participating in continued professional development activities,and effectively using available resources,equipment,and information technology to guarantee the provision of top clinical care.The existence of a supportive work atmosphere that examines the quality of care through clinical audits,clinical research,and patient satisfaction surveys also increases nurses’ enthusiasm.These results correspond to a study that found a higher clinical practice performance among nurses in private hospitals than among those in government teaching hospitals.This result can be explained by some supportive aspects of the work atmosphere and organizational climate that improve nurses’autonomy and interest associated with decentralized decision-making [49].
Nurses in private hospitals were also found to be better leaders.Nurses were praised and recognized for achievement by their supervisors and took responsibility for the level of care provided.This may be associated with a supportive work atmosphere that encourages enthusiasm,autonomy,recognition of achievement,as well as professional and educational growth.
Concerning the relationship between clinical leadership behavior dimensions and participants’ demographic data,nurses’behaviors did not differ significantly between age groups and sexes.Concerning experience,their clinical leadership behaviors varied significantly(P<0.01).Further,nurses who had from 5 to 10 years’experience had higher mean scores than nurses with other durations of experience did,perhaps because nurses with more years of experience are well oriented with most clinical practices that improve and enhance their beliefs or values combined with their knowledge and experiences that were acquired over time,through which they could practice autonomy and develop their clinical leadership behaviors.This result is supported in the literature.Experienced nurses were found to be effective clinical leaders and manifested clinical leadership behaviors [50].It is believed that years of experience are an influential factor in leadership in terms of the leaders’ skills and the followers’ understanding of their capabilities [51].Years of experience in nursing were highly associated with clinical leadership behaviors in nurses.However,other findings revealed that highly experienced nurses had fewer clinical leadership behaviors [52-54].
The findings of this study showed a significant difference in nurses’ overall mean scores concerning their marital status,single nurses having higher total scores in overall clinical leadership and its dimensions in term of advocacy and empowerment,decision making,quality and safety,and clinical excellence.This could be related to the disturbances in the social life of nurses,which lead to a sense of separation or failure.Nurses then consider this as a challenge and opportunity for success in their work-life by developing their competencies,autonomy,and independence,while engaging in clinical leadership activities and decision-making processes.In this respect,personal life factors,including marital status,may significantly impact the development of clinical leadership skills among nurses [55].
5.Limitations
This study reported several limitations.At first,this study used a self-report questionnaire for clinical leadership behaviors.Therefore,we suggest further studies on clinical leadership behaviors by using observation techniques and applying training programs to upgrade clinical leadership behaviors among staff nurses.Secondly,the data were collected from two hospitals only.Also,we suggest selecting a representative,an adequate sample of hospitals to represent data about clinical leadership behaviors among staff nurses.
6.Conclusion
This study adds to the existing academic literature by concluding that nurses’ overall clinical leadership behaviors were high,including self-awareness,advocacy,empowerment,decision making,communication,quality and safety,teamwork,and clinical excellence,all of which are considered key competencies that develop clinical leadership behaviors.Designing clinical leadership development interventions in all areas of nursing practice and developing clinical ladder programs in healthcare systems is essential in the five focus areas of research,quality,education,service excellence,and leadership.We should aim to establish a system within hospital organizations to reward and recognize excellence in practice and leadership behaviors.
CRediT authorship contribution statement
Heba Mohamed Al Anwer Ashour:Conceptualization,Data Curation,Formal analysis,Investigation,Methodology,Software,Validation,Writing -original draft.Maram Ahmed Banakhar:Methodology,Writing -original draft,Writing-reviewing and editing.Naglaa Abd Elaziz Elseesy:Conceptualization,Data curation,Formal analysis,Investigation,Methodology,Software,Validation,Writing -original draft.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
We would also like to express our gratitude to the critical care nurses who participated in the study.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.06.017.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of white noise on procedural pain-related cortical response and pain score in neonates:A randomized controlled trial
- Preventive strategies for feeding intolerance among patients withsevere traumatic brain injury:A cross-sectional survey
- Effects of multidisciplinary exercise management on patients after percutaneous coronary intervention:A randomized controlled study
- Implementation strategies to improve evidence-based practice for post-stroke dysphagia identification and management:A before-andafter study
- Development and validation of a rapid psychosocial well-being screening tool in patients with metastatic breast cancer
- The relationship between acceptance of illness and quality of life among men who have sex with men living with human immunodeficiency virus:A cross-sectional study