The development and evaluation of a nurse anaesthesia model for practice in South Africa
2022-07-31JDHoltzhausenCharleneDowningMariePoggenpoelGuguNdawo
JD Holtzhausen,Charlene Downing,Marie Poggenpoel,Gugu Ndawo
School of Nursing,University of Johannesburg,Doornfontein Campus,Johannesburg,South Africa
Keywords:Nurse Anesthetists Occupation Practice model South Africa
ABSTRACT Objective:This article aimed to present a developed model for nurse anaesthesia practice in South Africa and then to evaluate the model by national and international anaesthetist experts.Methods:For the model development,a theory-generative research design was used as guided by Chinn&Kramer.The study included four steps to develop and evaluate the model:step one,concept analysis;step two,placing the concepts into relationships;step three,description and critical reflection of the model;step four,evaluation of the model.For evaluation of the model,data were collected using individual,in-depth interviews.Four South African medical specialist anaesthesiologists and four international nurse anaesthetists were interviewed.Transcribed interviews were analyzed using Tesch’s eight steps of thematic data analysis.Results:The model was described in four phases:relationship phase,working phase,termination phase,and independent phase.The model shows a development process of a student nurse anaesthetist by a nurse anaesthetist facilitator to the mastery of the scope of practice of a nurse anaesthetist.Two themes(six categories) emerged through thematic analysis:the model and guidelines for implementation were found to be appropriate(model and guidelines for implementation are important because of the need for nurse anaesthetist,the model is applicable because it is described as comprehensive,the relationship phase was found to be important and the interdependence between disciplines is imperative,the affirmation that mastery has to be attained by nurse anaesthetists due to the complexity of services rendered),anticipated limitations to the South African nurse anaesthetist (the need to identify complex patients and limitations on the setting and refer to higher level of care,limitations due to red tape).Conclusions:This model provides fertile soil to inform and outline the education (curriculum) and practice (scope of practice) and research for nurse anaesthesia practice in South Africa.
What is known?
There is a severe shortage of surgery,obstetrics,and anaesthesia providers in low-and middle-income countries like South Africa,yet there is currently no professional nurse anaesthetist registration where a nurse is permitted to independently provide anaesthesia services to patients.
What is new?
● This is a pilot study in the development of a practice model for nurse anaesthesia in South Africa.
● The model can inform and outline the education (curriculum) and practice(scope of practice) and research for nurse anaesthesia practice in South Africa.
1.Introduction
A nurse anaesthetist is an independent practitioner who is specially trained to administer anaesthesia like general anaesthesia,regional anaesthesia,or local anaesthesia,and to provide pain management services to patients across all tiers of health service delivery [1].In South Africa,there is currently no professional nurse anaesthetist registration where a nurse is permitted to independently provide anaesthesia services to patients [2-5].There is a severe shortage of surgery,obstetrics,and anaesthesia providers in low-and middle-income countries like South Africa[6,7].There is an average of 1.36 physician anaesthesia providers per 100,000 population in Africa.South Africa has the highest physician anaesthesia provider density(16.18 providers per 100,000 population) [3].Contextualizing South Africa’s higher density physician anaesthesia providers,one needs to consider the disparity in the South African healthcare system where there are two streams of services:the private and public sectors.Compared to the private sector,the public sector is overburdened,understaffed,and ill-equipped[8,9].Eighty percent(80%)of the country’s medical specialists serve the private sector,which only constitutes 27.5% of the country’s population [10].This means that although South Africa has 16.18 per 100,000 population physician anaesthesia providers,only 3.2 providers per 100,000 population serve the public sector.Given the situation,most South African health seekers suffer because of a lack of anaesthesia providers.It is estimated that nurses participate in at least 80% of anaesthesia procedures worldwide and are the sole providers for 60% of all anaesthesia cases worldwide [11].The Democratic Nursing Organization of South Africa therefore suggests that the introduction of nurse anaesthetists in South Africa would bring much relief to the already understaffed and overworked medical practitioners[2].For this reason,a model for nurse anaesthesia practice must be developed to lay a foundation for nurse anaesthetist practice to provide safe and affordable anaesthesia services in South Africa.The purpose of the present article is to first present a developed model for the independent nurse anaesthesia practice in South Africa and then to evaluate the model by national and international anaesthetist experts.
2.Methods
2.1.Study design
The research methodology was described as guided by Chinn and Kramer’s theory[12].In step one,concept analysis took place.First,a situational analysis was done by means of concept identification of existing nurse anaesthetist conceptual frameworks,and secondly,these identified concepts were defined and classified.In step two,the concepts were placed into relationships.In step three,the model was developed and evaluated by model-specific experts.In step four,the model was evaluated by anaesthetist experts.
2.2.Ethical consideration
This article forms part of a doctoral study titled:A model for nurse anaesthesia practice in South Africa in which theory construction for nurse anaesthesia practice in South Africa took place.Ethical approval was granted by the University of Johannesburg in 2018 and renewed every year till 2021(Certificate no:REC-01-151-2018).All of researchers sought to comply with sound ethical principles in all aspects of the study,and these included autonomy,beneficence,non-maleficence,and justice [13,14].
2.3.Development of the model
2.3.1.Step one:concept analysis
Gathering evidence to identify the central concept may arise from a plethora of sources [12].Literature of nurse anaesthetist practices from around the world were examined to identify the central concepts on which nurse anaesthetists’practice hinges,thus permitting an all-inclusive sampling method.The sample included literature of nurse anaesthetists’ practices,the scope of practice,practice standards,and competencies as defined by the South African Nursing Council[13],from countries where nurse anaesthesia is practiced.In this study,data was collected from countries where nurse anaesthesia was practiced during the year 2018,as guided by the World Federation of Societies of Anaesthesiologists [5],Kempthorne,et al.[3],and the International Federation of Nurse Anaesthesia [11].Data was collected by systematically accessing a host of databases as guided by the University of Johannesburg’s subject librarian for published journal content on nurse anaesthetist’s practices,the scope of practice,practice standards,and competencies.The World Wide Web was searched,within reason,of public websites of nurse anaesthetist associations,nurse anaesthetist councils,nurse anaesthetist federations,and nursing councils from countries,regions,or states where nurse anaesthesia is practiced to see if these address nurse anaesthetist practices,the scope of practice,practice standards,and competencies.Searches were conducted between April 2019 and July 2019 and reviewed for accuracy in February 2021.The following databases were searched:EBSCOhost(Academic Search Premier,AHFS Consumer Medication Information,CINAHL,E-Journals,Health Source -Consumer Ed,Health Source -Nursing Academic Ed,MasterFile Premier,MEDLINE,PsycARTICLES,PsycINFO,SocINDEX);ScienceDirect;Scopus;Web of Science;African Journals;Index to South African Periodicals;PubMed Central;Cochrane Library;Google Scholar;Nexus.The following Boolean operators were used:nurs* anesthes*;OR nurs* anaesthes*;NOT anesthes* technician;NOT anaestes* technician;AND model/s;OR scope of practice;OR service standard/s;OR practice standard/s;OR competencies.
Unpublished literature was excluded from the study as it is inaccessible.Also,literature where the nurse anaesthetist is not defined as a primary and independent practitioner of anaesthesia was excluded.Where no data was available from the International Federation of Nurse Anaesthetists[11]and the World Federation of Societies of Anaesthesiologists [3,5],these countries,islands,or regions were also excluded.Furthermore,where literature is not presented in English,it was excluded from the study.Moreover,countries,islands,and regions were excluded if non-relevant or too little information was found on the search as explained above.
As a result of the searches,the following purposively selected existing nurse anaesthetist practices from around the world were explored and described.These were of Belize [5,15],Cambodia[16,17],Democratic Republic of the Congo[11],Ethiopia[18],Ghana[3,5,19],Haiti [5,20],Indonesia [11],Jamaica [5,11],Kenya [5,21],Rwanda[3,5,22],United States of America[1,3,5,11],Zambia[5,23],and Zimbabwe[5,24].
All four authors critically examined the nurse anaesthesia practices of these countries using strategies of triangulation,prolonged engagement,persistent observation,and member checking[14,25] and agreed on a central concept,namely ‘facilitation to mastery of scope of practice’as it applies to the nurse anaesthetist in the South African context.The central concept is divided into three concepts,namely ‘facilitation,’ ‘mastery,’ and ‘scope of practice.’ By means of concept analysis [14],the concepts are defined using the dictionary and subject definitions,and the results are presented in Table 1.
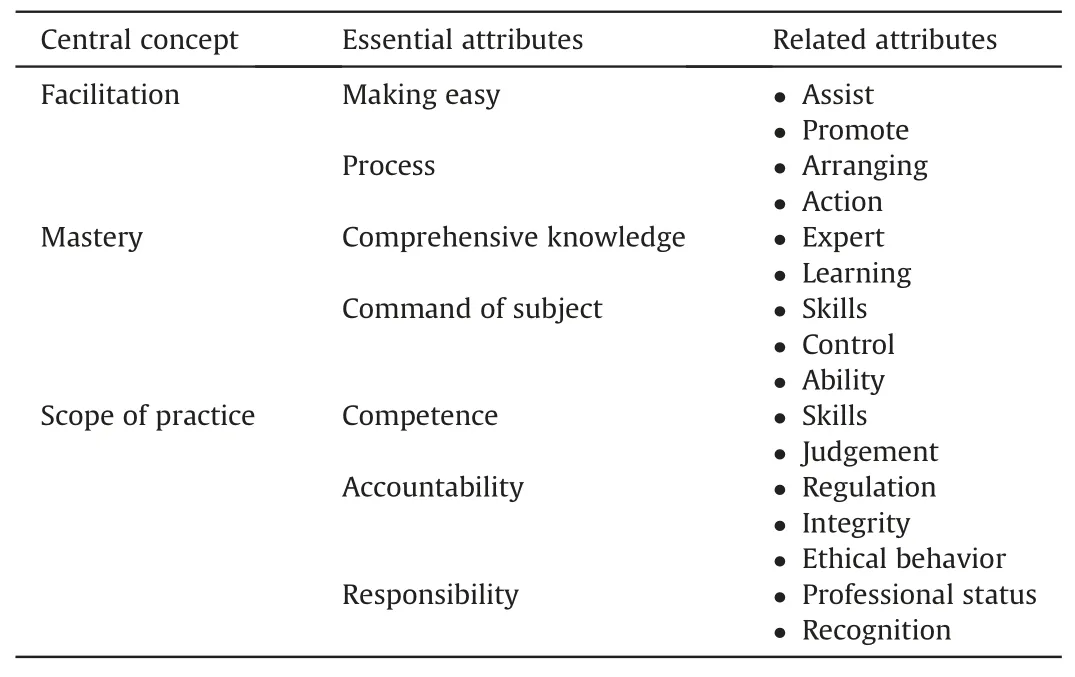
Table 1 A summary of attributes of‘facilitation’,‘mastery’,and‘scope of practice’defined by concept analysis.
The concept ‘scope of practice’ as it applies to the nurse anaesthetist in South Africa can be defined as the individual’s competence,accountability,and responsibility as a health professional.A nurse anaesthetist is 1)competent:ready to use skills and judgment in practice;2) accountable:able to be registered as a nurse anaesthetist and willing to abide by the regulations;and 3)responsible:upholding professionalism and demanding recognition from the public and peers [26].
2.3.2.Step two:placing the concepts into relationships
The concepts identified and defined in step one were then placed into contextual relationships with each other [12].These inter-relational statements formed a tentative model.Using Dickoff,James,and Wiendenbach’s[27]survey list,the central concepts were classified by asking:Who is the agent?Who is the recipient?What are the dynamics? What is the procedure? What is the context? What is the outcome?
Who is the agent?A nurse anaesthetist facilitator performs the activity,but who is this?In the novice days of nurse anaesthesia in South Africa,the profession will have to rely on South African medical anaesthesiologists for ontological facilitation to mastery in the practice.The reason for this medical influence allowance is that there is no nurse anaesthetist in South Africa.Prospective nurse anaesthetists will be able to gain epistemology and methodology from textbooks,international nurse anaesthetist,and foundational embedding into the nursing model of care.However,as nurse anaesthesia in South Africa matures,the senior nurse anaesthetist will eventually be able to train nurse anaesthetists.From here on,these two parties will collectively be named the nurse anaesthetist facilitator in this study.
Who is the recipient?A student nurse anaesthetist (prospective nurse anaesthetist)in South Africa will be facilitated to master the scope of practice of a nurse anaesthetist as described by the regulatory authority.Thus,the student nurse anaesthetist is the recipient.
What are the dynamics?There is a need for a nurse anaesthetist in South Africa on account of the severe shortage of surgery,obstetrics,and anaesthesia providers in low and middle-income countries like South Africa.There is currently no professional registration available in South Africa to regulate nurse anaesthetists by which they can prescribe and administer anaesthesia and chemical pain management services to patients.
What is the procedure?The agent must engage with the recipient to facilitate the recipient to master the scope of practice in anaesthesia,sedation,and chemical pain management services as practiced by the nurse.This is done by making it easier for the student nurse anaesthetist to follow the process to gain comprehensive knowledge and command of the subject of nurse anaesthesia.Consequently,this allows the recipient to apply the scope of practice of a nurse anaesthetist in South Africa with competence,accountability and assuming responsibility for actions and omissions.
What is the context?South African nurse practice environment is unique in that there are two main sectors:the private sector and the public sector.In the private sector,patients are financially liable for the medical care received;in the public sector,the financial liability rests either with the government or(according to an income scale)with the patient.The public sector provides services on tiers levels of intervention complexity.These tiers-arranged from least complex care to most complex care-are a clinic,community health center,district hospital,regional hospital,and tertiary hospital.Ideally,the agent’s focus is to provide services where a need is identified-either in the private sector or in the public sector.
What is the outcome?The activity’s terminus or endpoint is mastery of the scope of practice of a nurse anaesthetist in South Africa.
2.3.3.Step three:description and critical reflection of the model
Flowing out steps one and two,the researcher described a model that forms a framework of reference for nurse anaesthetists’practice which is contextually appropriate for South Africa.
This model was then evaluated by model-specific experts regarding the model’s clarity,simplicity,generality,accessibility,and the importance [12].Academic model-specific experts from around the world,who are familiar with nursing science models and theory generation,were consulted to evaluate the model.The researcher presented the study’s background and rationale,research questions,research purpose and objectives,and research methodology,and strove to inform the participant of the description of the complete model via secure and private internet telecommunication.The model-specific experts were then asked to evaluate the model via an online survey which asked basic demographic questions and the following questions:How clear is the model?How simple is the model?How general is the model?How accessible is the model? How important is the model? Any additional comments?
In accordance with the critical reflection of the model-specific experts,the model was adapted.The model in Fig.1 has already been adapted according to the evaluation of the model evaluation experts.An in-depth discussion of the evaluation by model-specific experts falls outside the scope of this article.
2.4.Evaluation of the model
Based on the nurse anaesthetist’s practices,scope of practice,practice standards,and competencies (step one) and the model description and evaluation (step three),the practice model was evaluated by anaesthesia specific experts.
2.4.1.The setting and participants
Individual,in-depth interviews were conducted with the chosen sample.In-depth interviews seemed appropriate as their purpose is to provoke the participants’ opinions,attitudes,beliefs,experiences,perceptions,thoughts,and feelings[28,29].These interviews were conducted over a secure and private internet telecommunication medium to ensure confidentiality and anonymity.
South African medical specialist anaesthesiologists and international nurse anaesthetist constituted the study population.Both purposive and snowball sampling methods were used to recruit participants.Purposive sampling refers to the selection of participants based on the researcher’s judgment,knowledge,and representative value[29].Snowball sampling is when one participant is asked to invite another participant based on appropriateness [28].The researcher formally invited anaesthesia experts based on their experience and acquaintance with the research process.Some anaesthesia experts were identified by contacting university faculties;others were suggested by these experts as valuable prospective participants.Participants had to comply with the inclusion and exclusion criteria as stipulated in the research proposal and approved by the relevant scientific and ethics boards.These criteria are that the participants be registered as an anaesthesiologist with the Health Professional Council of South Africa or as a nurse anaesthetist in the country of practice (where there is no council registration for the nurse anaesthetist in his/her country of practice,the individual had to be able to legally work as a nurse anaesthetist in his/her country) and be able to communicate in English.Participants were not identified by name,organization,or registration number at any point.
Having invited an individual anaesthetist participant to an interview and received confirmation of their interest,the interview date and time were agreed upon between the participant and the researcher.Hereafter,the researcher sent the participants a‘Knowledge Pack’ at least one week ahead of the interview containing the informed consent,a PowerPoint© presentation of the study,and the model.
The participants brought a diverse array of experiences to the table.This promoted diversity of thought and view of the future.This panel of experts consisted of four South African medical specialist anaesthesiologists and four international nurse anaesthetists.The South African medical specialist anaesthesiologists represented and contextualized South African anaesthesia practice,whereas the nurse anaesthetists represent nursing anaesthesia practice on the international tier.The size of the panel proportionally increased until data saturation had been reached.Data saturation occurs when few or no new ideas,themes,or codes appear [30].Participants had the freedom to participate in the study or not and had the choice to withdraw their participation at any point.
2.4.2.Data collection
Qualitative data collection seemed appropriate to evaluate this research as information is gathered by direct interchange with an individual who the researcher expects to have knowledge of a particular context [31].This interchange was interpretative [31].Therefore,the values and judgments of the researcher were openly stated.Informed consent for the interview was requested from all participants willing to participate in the study via secure end-toend encrypted communication internet telecommunication using Zoom © or WhatsApp © [32].Verbal permission to record the interview was requested at the beginning of each interview.Participants were asked,“How is the model for you?” During the interview,probing and prompting were applied to enrich the data,and data were collected until data saturation was achieved [30].
2.4.3.Data analysis
Data analysis occurred in parallel with data collection.All interviews were transcribed by the researcher allowing additional immersion of the data.Researchers also made field notes which entailed observational notes,theoretical notes,and methodological notes.The transcriptions and field notes were then analyzed using Tesch’s eight steps of thematic data analysis by the researcher[33,34].Data was then sent to an independent coder who holds a doctoral degree in nursing and is well-versed in qualitative research.Both independent coder and the researcher met together,and consensus of the data analysis was reached.
3.Results
3.1.Description of the model
The model (Fig.1) is divided into four phases,namely relationship phase,working phase,termination phase,and independent phase.
In the relationship phase,a student nurse anaesthetist embarks on the journey to mastery of the scope of practice of the South African nurse anaesthetist.The nurse anaesthetist facilitator builds a professional relationship with the student nurse anaesthetist through rapport,trust,and open communication.Additionally,the nurse anaesthetist facilitator creates a conducive learning environment.This is achieved by stimulating higher-order learning,ensuring an emotionally and psychologically safe facilitatorstudent relationship,enabling open communication,and providing support.The nurse anaesthetist facilitator,throughout all next phases,will influence the student nurse anaesthetist in changing attitudes,habits,skills,ways of thinking,and ways of doing and working(practice),as well as maintaining these changes.
In the working phase,the nurse anaesthetist facilitator introduces the scope of practice of the nurse anaesthetist in South Africa to the student nurse anaesthetist.By assisting and promoting,the nurse anaesthetist facilitator makes it easier for the student nurse anaesthetist to master the scope of practice of a nurse anaesthetist.The student nurse anaesthetist is facilitated in the realization that facilitation to mastery is a process that involves arranging tasks systematically and applying theory to practice and therefore generates effective decision making.
‘Comprehensive knowledge’ is when the practitioner is an expert in the field of chosen practice and due to learning.An expert is someone who has superior skills,a knack for,and a well-polished grasp over the subject in question.To attain the status of expert,the individual must have acquired facility in the activity by promoting competence in and understanding of the content of the subject which was learned.Furthermore,the individual displays learning by gaining a formal education.Through learning the student nurse anaesthetist will attain comprehensive knowledge about nurse anaesthesia in South Africa and hence become an expert in the field.The nurse anaesthetist facilitator promotes the student nurse anaesthetist to have superior skills and complete facility over the subject through formal education.The student nurse anaesthetist will also be assisted to deal effectively with challenging situations in practice.Having comprehensive knowledge and command of the subject of the scope of practice of nurse anaesthesia,the student nurse anaesthetist achieves mastery.
Through this process of mastery,the student nurse anaesthetist comes to recognize that the scope of practice is a synthesis of competence,accountability,and responsibility.With regards to competence,the student nurse anaesthetist is facilitated to display skills and use clinical judgment through critical thinking.Reciprocally,the student nurse anaesthetist becomes capable of being a nurse anaesthetist in practice and performing anaesthetist duties with much expertise,backed up with the necessary experience.
Furthermore,the student nurse anaesthetist is facilitated to be accountable for the scope of practice of nurse anaesthesia.Included and related to this are the permissions and limitations,and acts and omissions as provided by the relevant professional regulatory body.Moreover,the student nurse anaesthetist comes to understand what ethical behavior in nurse anaesthesia practice entails and is facilitated to act with integrity.This is illustrated by the student nurse anaesthetist gaining consent before performing a procedure,and being consistent and uncompromising concerning patient gender,race,social status,economic status,and religion,thus protecting the patient’s basic rights.The student nurse anaesthetist is facilitated also in the full appreciation of the responsibility a nurse anaesthetist carries in practice.As such the student nurse anaesthetist learns to portray themselves as a nurse anaesthetist being a professional person and holding recognition towards the profession.
The termination phase is the third phase.This phase is the assessment of the student nurse anaesthetist and‘saying goodbye’between the nurse anaesthetist facilitator and the student nurse anaesthetist.Assessment is realized by evaluating if the student nurse anaesthetist has achieved mastery of the scope of practice of a nurse anaesthetist.‘Saying goodbye’ is realized by the nurse anaesthetist facilitator re-enforcing the scope of practice into clinical practice and allowing the student nurse anaesthetist to transition towards independent practice.Thus,that which has been learned is reviewed so that the student nurse anaesthetist will have self-efficacy and self-confidence in the practice of a nurse anaesthetist.
Lastly,the independent phase allows the nurse anaesthetist to step into practice and execute services,having achieved mastery of the scope of practice of nurse anaesthesia in South Africa.The student nurse anaesthetist is no longer a student but an independent practitioner.The nurse anaesthetist can practice in all of the South African healthcare contexts,namely clinics,community health centers,district hospitals,regional hospitals,and tertiary hospitals.
During any stage,‘stagnation’may occur.Stagnation is when the student nurse anaesthetist dwindles off the path of becoming an expert.A stagnation may occur due to personal or professional factors.When a stagnation becomes apparent,the nurse anaesthetist facilitator assists the student nurse anaesthetist by backtracking to a mutually agreed upon,non-compromised phase,and builds on its foundations.Model-specific experts found the model to be clear,simple,general,accessible,and important.
3.2.The step of evaluating the model
The panel of anaesthetist experts (Table 2) consisted of four South African medical specialist anaesthesiologists and four international nurse anaesthetists.The South African medical specialist anaesthesiologists represented and contextualized South African anaesthesia practice,whereas the nurse anaesthetists represent nursing anaesthesia practice on the international tier.All four medical specialist anaesthesiologists had master’s degrees in medicine.Two of the nurse anaesthetists had a doctoral level of education,one had a postgraduate diploma,and one had an undergraduate qualification.No participant withdrew from the study,although they had the option to do so.
Thematic analysis of the interviews whereby the model was evaluated yielded two themes (Table 3).Theme one is ‘the model and guidelines for implementation was found to be appropriate.’In this first theme,participants expressed that the model and guidelines for implementation are important and comprehensive.Moreover,participants highlighted the importance of the relationship phase and affirmed that mastery has to be attained because of the complexity of anaesthesia services rendered.Theme two is the ‘anticipated limitations to the South African nurse anaesthetist.’ The anaesthetist experts advised that if there is a nurse anaesthetist in South Africa,the provider ought to know what their limitations are and be able to refer to a higher level of care.In addition,the anaesthetist experts also cautioned that there may be red tape in implementing this model.Red tape is when implementation is hindered by excessive complex procedures which result in delay or inaction.In this instance,the red tape may be in the form of regulatory processes and the logistics of learning.

Table 2 Demographics of the participants.

Table 3 Overview of the themes,categories,and subcategories.
3.2.1.Theme one:the model and guidelines for implementation were found to be appropriate
The analysis showed that the participants found the model to be appropriate.Under this theme,four categories emerged that proved that the model is appropriate.These four categories will now be discussed and evidence by means of direct quotations from the transcribed interviews will be provided to affirm the data analysis findings.
Category 1A:model and guidelines for implementation are important because of the need for the nurse anaesthetist.All the participants affirmed the need for nurse anaesthesia in South Africa.The South African medical anaesthesiologist shared the need for anaesthesia mostly by sharing the dire need for service provision,especially in the South African public health sector and South African rural areas.
“I mean there’s a lot of places where surgeons are doing their sedations and that's just horrible because they have no idea and no interest,and they just give something and continue with what they are doing.And there are like,I know about a lot of mortalities that are happening.So in a world like that,I think…filling gaps where the anaesthetist won’t cover.” (Participant 4,specialist anaesthesiologist,10 years experience)
“And … and we see that,particularly with the saving mother’s report,where we have maternal deaths … because the doctors operating also do the anaesthesia and while he’s operating you can’t monitor the patient and so forth…”(Participant 6,specialist anaesthesiologist,3 years experience)
“It’s been important internationally for the nurse anaesthetist to be able to advocate for their skills and what they can…what they can bring and help,help take care of the public.”(Participant 8,nurse anaesthetist,26 years experience)
Category 1B:the model is applicable because it is described as comprehensive.All the participants expressed that the model and the guidelines for implementation are comprehensive.This means that the model and the guidelines for implementation are fitting as they can be applied to the South African context.Participants shared this sentiment by saying:
“But I think that is quite important because in the whole… in the whole the study as a model seems like feasible … it seems like afunctional kind of model.” (Participant 6,specialist anaesthesiologist,3 years experience)
“I think the model is appropriate … for an entry path in any framework.” (Participant 7,specialist anaesthesiologist,3 years experience)
Category 1C:the relationship phase was found to be important and the interdependence between disciplines is imperative.Participants agreed that the relationship phase is very important.Proposed guidelines for the implementation of the relationship phase were also found to be valid.In the relationship phase,the nurse anaesthetist facilitator and the student nurse anaesthetist build a professional relationship through rapport,trust,and open communication.A conducive learning environment is formed by stimulating higher-order learning,ensuring an emotionally and psychologically safe facilitator-student relationship,enabling open communication,and providing support.Many participants reiterated the importance of allowing medical specialist anaesthesiologist to facilitate student nurse anaesthetists in the virgin years of the profession and that this facilitation is handed over to the nurse anaesthetists themselves,as the profession matures.
“So,we find that you know,sometimes students early on…may not even know what they don’t know and as students actually we find as they get towards the end of the program,they don’t give themselves enough credit for the strengths that they have.So,we have to point out to them,‘these are the things that you do well.’”(Participant 1,nurse anaesthetist,18 years experience)
“And the relationship phase -incredibly,incredibly,important!”(Participant 8,nurse anaesthetist,26 years experience)
Category 1D:affirmation that mastery has to be attained by nurse anaesthetists due to the complexity of services rendered.All the participants recognized that mastery needs to be attained and maintained by the nurse anaesthetist due to the complexity of providing anaesthesia services.The guidelines for implementation of mastery are found to be adequate.Nurse anaesthetists must have a well-formed knowledge base to provide anaesthesia services,in conjunction with professional confidence.
“And mastery I think you know…I like the idea of…of…gaining uh … mastery of skills and or knowledge or … higher level and it was being able to apply the knowledge and I … that hit home for me… ”(Participant 1,nurse anaesthetist,18 years experience)
“… Where you know there will be teaching done regularly,that there will be continuous assessment of the individual for competency and things like…and whether they’ll be able to achieve the skills.” (Participant 6,specialist anaesthesiologist,3 years experience)
3.2.2.Theme two:anticipated limitations to the South African nurse anaesthetist
By evaluating a practice model for nurse anaesthesia,the participants foresaw limitations to the introduction of nurse anaesthetist in South Africa.These limitations can be categorized into two categories.First,the South African nurse anaesthetist needs to identify complex patients and limitations on the setting and refer to higher level of care indeed to be appropriate.Secondly,the nurse anaesthetist in South Africa may experience some limitations due to red tape,which is further explained below.
Category 2A:the need to identify complex patients and limitations on the setting and refer to higher level of care.A responsible nurse anaesthetist ought to know their professional limitations.The medical specialist anaesthesiologists expressed the complexity of the service rendered by referring to the American Society of Anesthesiologist’s Physical Status Classification System (ASA).Some participants expressed that nurse anaesthetists should be limited to ASA I and ASA II patients.
“Cause you … I expect nurse anaesthetist would be more straightforward cases.” (Participant 4,specialist anaesthesiologist,10 years experience)
“Yeah,so I think that will be like a big thing for them to also selfmanaged and maybe say,‘well this is outside of my scope of practice,I need to refer this patient’,or whatever the case might be,but I think that needs to be a big thing.” (Participant 5,specialist anaesthesiologist,5 years experience)
Category 2B:limitations due to red tape.The second category is divided into two subcategories:‘regulatory red tape’ and ‘logistics for learning’.During interviews,participants expressed possible barriers that may prevent the nurse anaesthetist model for practice in South Africa from being implemented or may hinder the guidelines for implementation of the model.
Subcategory one:regulatory red tape.Participants foresaw that the current South African nurse,medical,and/or governmental regulatory structure is not fertile soil for this practice model due to no fault of the model or the guidelines for the implementation itself.
“And,and the bureaucracy around it is also going to be a problem…” (Participant 7,Participant 7,specialist anaesthesiologist,3 years experience)
“Those,I think is the biggest challenges is the politics and the government recognition … recognition and support for our education.” (Participant 8,nurse anaesthetist,26 years experience)
Subcategory two:logistics for learning.Facilitating student nurse anaesthetists may also not be as easy as was foreseen by not only the South African medical specialist anaesthesia experts but also the international panel of nurse anaesthetists.
“And you have some general things,but when it comes down to really looking at your audience,the setting,what you have for resources,those are the pieces I think is always a … a challenge in terms of the flexibility.” (Participant 1,nurse anaesthetist,18 years experience)
“Actual theoretical … where you sit and have a theory … our programs completely fell apart because no one had time to do that kind of stuff.So,I think that is a big problem is who is going to train them?” (Participant 4,specialist anaesthesiologist,10 years experience)
4.Discussion
One-third of the global burden of diseases could be addressed by surgical care,which encompasses surgery,obstetrics,trauma,and anaesthesia [35].South Africa does not have any non-physician anaesthesia providers [2-5].To better healthcare accessibility,boundaries of responsibility and authority need to be shifted[36,37].The model thus provides fertile soil to inform and outline the education (curriculum) and practice (scope of practice) and research for nurse anaesthesia practice in South Africa.
Support structures such as those provided by facilitators and lecturers are vital for nursing students’ learning process [38].The relationship with a facilitator is of cardinal importance in nursing practice as it facilitates the development of clinical reasoning[39].In the nurse anaesthetist model for practice in South Africa,the relationship between the nurse anaesthetist facilitator and the student nurse anaesthetist is emphasized.A strong relationship is the foundation for the student nurse anaesthetist to reach mastery of the scope of practice and ultimately practice independently.
In the nurse anaesthetist model for practice in South Africa,mastery,and thereby the skills and ability to deal with the complexity of anaesthesia services,is key.Anaesthesia risks can either be related to the patient or the practitioner [40,41].Complexity of anaesthesia as described by anaesthesia complications and emergencies is well recorded in literature [42-45].Provision of anaesthetic services requires practitioners to have command of the subject and to have comprehensive knowledge.This mastery of the scope of practice is fostered in the working phase and evaluated in the termination phase of the model.
The South African nurse anaesthetist should be able to recognize their limitations and limitations on the setting and refer when applicable.Responsible practitioners need to exhibit recognition of their cognitive errors,such as provider bias and heuristic reasoning,to ensure that patients are effectively treated [46].Complex patients with multiple variables contributing to their unwellness are best served when referred to specialized clinics[47].Timely referral to higher or more specialized care facilities can improve a patient’s long-term outcome[48].Nurse anaesthetists working in rural areas may be supported by regular visits from medical specialist anaesthesiologists to handle difficult cases together and to further the skills and confidence of the nurse anaesthetists.Barriers to referral can be a practitioner’s perception of the scope of care needed,medical paternalism,lack of an institutional referral policy,poor human resource capacity,and lack of awareness about the existence of specialized care providers [49].
Relevant South African regulatory authorities should adapt to the times and develop programs to upgrade nursing professionals[50].In the last years post-apartheid,many quality-improvement programs have been initiated but not many produced the required level of quality service delivery[51].In South Africa,policy implementations have been slow due to provider ambivalence,challenges with infrastructure,and a shortage of human resources[52].The principal healthcare challenges in Africa are inadequate human resources,inadequate budgetary allocation to health,and poor leadership and management [53].In South Africa,it is the responsibility of the nurse and health leaders to reform the country’s health policy,thereby facilitating nurse anaesthetist practice.By investing in infrastructure,and the development of collaborative frameworks between nursing and midwifery and higher educational councils,better education can be facilitated.Southern Africa’s education and training system for the health sector has not grown adequately to meet health needs and health system requirements [54].
5.Limitations
One limitation of this study is that the concept selection is derived from the current nurse anaesthesia framework as described in step one:concept analysis.It is often difficult to gain legislative information,especially in developing countries.Some countries do not have a nursing council or association website that could be found,while some websites are poorly maintained or have unverified domain names due to using free website hosting services.Many countries’ anaesthesia associations’ websites are not published in English.Moreover,published research articles on the status of nurse anaesthesia in some countries may be limited due to the sheer deficiency of anaesthesia providers in that country.That said,the data gathered was not sufficient enough to cover conditions of nurse anesthesiologists in vaious countries or regions.Despite this limitation of the study,the research question was sufficiently answered by fulfilling the research purpose and objectives.
6.Conclusion
The evaluation by national and international anaesthesia experts warrants the model appropriate and therefore able to inform and outline the education (curriculum) and practice (scope of practice)for nurse anaesthesia practice in South Africa.Challenges on regulatory red tape and nurse anaesthetist trainting should be taken into account for facilitation to mastery of scope of practice.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Funding
Nothing to declare.
CRediT authorship contribution statement
JD Holtzhausen:Conceptualization,Methodology,Formal analysis,Writing -original draft,Writing -review &editing,Data curation,Investigation.Charlene Downing:Conceptualization,Formal analysis,Writing -review &editing,Data curation,Supervision.Marie Poggenpoel:Conceptualization,Formal analysis,Writing -review &editing,Data curation,Supervision.Gugu Ndawo:Conceptualization,Formal analysis,Writing -review &editing,Data curation,Supervision.
Declaration of competing interest
The authors have declared no conflict of interest.
Acknowledgments
Simonˊe van der Walt assisted with language editing of this manuscript.Mareza Christensen graphically designed the model as per the authors instruction.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2022.06.009.
杂志排行

International Journal of Nursing Sciences的其它文章
- Effects of white noise on procedural pain-related cortical response and pain score in neonates:A randomized controlled trial
- Preventive strategies for feeding intolerance among patients withsevere traumatic brain injury:A cross-sectional survey
- Effects of multidisciplinary exercise management on patients after percutaneous coronary intervention:A randomized controlled study
- Implementation strategies to improve evidence-based practice for post-stroke dysphagia identification and management:A before-andafter study
- Development and validation of a rapid psychosocial well-being screening tool in patients with metastatic breast cancer
- The relationship between acceptance of illness and quality of life among men who have sex with men living with human immunodeficiency virus:A cross-sectional study