Short-term outcomes of robotic liver resection: An initial singleinstitution experience
2022-02-12ManuelDurJavierBriceAnaPadialFerdinandoMassimilianoAnelliJuanManuelnchezHidalgoMarDoloresAyllRafaelCallejaLozanoCarmenGarcGaitan
Manuel Durán, Javier Briceño, Ana Padial, Ferdinando Massimiliano Anelli, Juan Manuel Sánchez-Hidalgo, María Dolores Ayllón, Rafael Calleja-Lozano, Carmen García-Gaitan
Manuel Durán, Javier Briceño, Ana Padial, Ferdinando Massimiliano Anelli, Juan Manuel Sánchez-Hidalgo, María Dolores Ayllón, Rafael Calleja-Lozano, Unit of Hepatobiliary Surgery and Liver Transplantation, General and Digestive Surgery Department, Reina Sofia University Hospital, Cordoba 14004, Spain
Manuel Durán, Javier Briceño, Ana Padial, Ferdinando Massimiliano Anelli, María Dolores Ayllón, Rafael Calleja-Lozano, GC18 Translational Research in Surgery of Solid Organ Transplantation, Maimonides Biomedical Research Institute, Córdoba 14004, Spain
Juan Manuel Sánchez-Hidalgo, GE09 Research in Peritoneal and Retroperitoneal Oncological Surgery, Maimonides Biomedical Research Institute, Córdoba 14004, Spain
Carmen García-Gaitan, Department of Anesthesiology and Resuscitation, Reina Sofia University Hospital, Cordoba 14004, Spain
Abstract BACKGROUND Liver surgery has traditionally been characterized by the complexity of its procedures and potentially high rates of morbidity and mortality in inexperienced hands.The robotic approach has gradually been introduced in liver surgery and has increased notably in recent years.However, few centers currently perform robotic liver surgery and experiences in robot-assisted surgical procedures continue to be limited compared to the laparoscopic approach.AIM To analyze the outcomes and feasibility of an initial robotic liver program implemented in an experienced laparoscopic hepatobiliary center.METHODS A total of forty consecutive patients underwent robotic liver resection (da Vinci Xi, intuitive.com, United States) between June 2019 and January 2021.Patients were prospectively followed and retrospectively reviewed.Clinicopathological characteristics and perioperative and short-term outcomes were analyzed.Data are expressed as mean and standard deviation.The study was approved by the Institutional Review Board.RESULTS The mean age of patients was 59.55 years, of which 18 (45%) were female.The mean body mass index was 29.41 kg/m².Nine patients (22.5%) were cirrhotic.Patients were divided by type of resection as follows: Ten segmentectomies, three wedge resections, ten left lateral sectionectomies, six bisegmentectomies (two VVI bisegmentectomies and four IVb-V bisegmentectomies), two right anterior sectionectomies, five left hepatectomies and two right hepatectomies.Malignant lesions occurred in twenty-nine (72.5%) of the patients.The mean operative time was 258.11 min and two patients were transfused intraoperatively (5%).Inflow occlusion was used in thirty cases (75%) and the mean total clamping time was 32.62 min.There was a single conversion due to uncontrollable hemorrhage.Major postoperative complications (Clavien-Dindo > IIIb) occurred in three patients (7.5%) and mortality in one (2.5%).No patient required readmission to the hospital.The mean hospital stay was 5.6 d.CONCLUSION Although robotic hepatectomy is a safe and feasible procedure with favorable short-term outcomes, it involves a demanding learning curve that requires a high level of training, skill and dexterity.
Key Words: Robotics; Hepatectomy; Minimally invasive surgery; Liver surgery; Da vinci
INTRODUCTION
Liver surgery has traditionally been characterized by the complexity of its procedures and potentially high rates of morbidity and mortality in inexperienced hands.In recent years, laparoscopic liver surgery has notably increased due to the beneficial outcomes in terms of fewer complications and transfusions, less blood loss and shorter hospital stays compared to open surgery with similar oncologic outcomes[1,2].
The number of liver procedures performed laparoscopically remains highly variable, ranging from 10% up to 80% in some centers[3].Complex hepatectomies such as major hepatectomies or in posterosuperior segments are still restricted to expert laparoscopic liver surgeons with considerable experience due to their inherent risk, which make them very technically demanding procedures[4-6].The increase in laparoscopic liver resections (LLR) has been accompanied by the development of parenchymal transection equipment and improved optical systems to compensate for the limitations of this approach and to increase the safety of hepatic resections[7].
The robotic approach is gradually being introduced in liver surgery and could compensate for the inherent difficulties of the laparoscopic approach.However, only some centers have implemented robotic-assisted surgery and the experience continues to be limited compared to laparoscopy[8].In this study, we report an initial experience with our first forty robotic liver resections (RLRs) using the da Vinci Xi SystemÒ(Intuitive Surgical, Inc., Sunnyvale, CA, United States).The aim of this study was to analyze the outcomes and feasibility of an initial robotic liver program implemented in an experienced laparoscopic hepatobiliary center.
MATERIALS AND METHODS
Following Institutional Review Board approval, we performed a retrospective review on our prospective recorded single-institution data between June 2019 and January 2021, including sixty-three patients who underwent a hepatobiliopancreatic procedure as follows: Nineteen distal pancreatectomies, four bilioenteric reconstructions and forty Liver resections.Forty RLRs were performed by a single hepatic surgeon (Dr.Briceño J) and included in the study.The indication of robotic surgery was established when the patient was considered a suitable candidate for minimally invasive surgical approach.All patients gave their informed consent prior to surgery.
Patient preoperative data included age, sex, body mass index (BMI), American society of anesthesiologists (ASA) classification, comorbidities, previous abdominal surgery and presence of chronic liver disease.
Intraoperative parameters included operative time, blood transfusion, use of inflow occlusion and duration and conversion rate.Operative time was defined as the time from the first incision to closure.Intraoperative complications were defined as an event requiring major deviation from the planned procedure.
The anatomical location of the lesions and surgical resection were defined according to the Brisbane terminology[9].The difficulty of the liver resections was graded according to the IWATE scoring system as revised in the Morioka consensus conference whereby a score of 0-3 is graded as low difficulty, 4-6 as intermediate difficulty, 7-9 as advanced difficulty and 10-12 as expert difficulty[10].
Postoperative variables were postoperative complications, length of stay, readmission within 30 d and mortality.Postoperative complications were recorded using the Clavien-Dindo classification up to 90 d after surgery[11].Complications were considered major when Clavien-Dindo > III.
The characteristics, diagnosis, number and size of the lesions were determined by pathological reports.Resection margins were defined as R0 resection when tumor distance from the margin was greater than 1 mm, as R1 resection when tumor distance from the margin was less than 1 mm and as R2 resection upon presence of macroscopic tumor at the margin.
Statistics demographic data and clinical outcomes were analyzed.The descriptive analysis included mean and standard deviation in continuous variables, while categorical and ordinal variables were reported as counts with proportions.AP-value of less than 0.05 was considered statistically significant.Statistical analyses were performed using SPSS Statistics version 22.0 (IBM, Armonk, NY, United States).
Surgical technique
After anesthesia, patients are placed in the French position and in the reverse Trendelenburg position (15°) with a slight left tilt (5°).The assistant is located between the patient’s legs and the robot is located at the left shoulder.The trocars are placed according to the following surgical requirements: The transection plane, the segments involved and the position of the endostapler.For a right hepatic lobe procedure, a 12 mm camera port is introduced in the right paraumbilical area and the main working ports (first and third robotic arm ports on the left and right, respectively) are placed in the left and right upper quadrant area.The fourth robotic trocar is placed near the left anterior axillary line.For a left hepatic lobe procedure or a left hepatectomy, trocar placement is similar to that described previously; however, the camera port is placed at the umbilicus to visualize the target anatomy.Once the robotic trocars are placed, the da Vinci Xi robotic system (Intuitive.com, United States) is docked.An AirSeal port (SurgiQuest Inc., Milford, CT, United States) is used for bedside assistance.An intracorporeal pringle maneuver using Huang’s loop is applied and used when deemed appropriate (Figure 1).
A robotic vessel sealer and bipolar cautery are the main instruments employed for parenchymal transection using the crush-clamp technique.An intraoperative robotic ultrasound device is employed to confirm the location of the tumor and to check the surgical transection line.For anatomic liver resection, indocyanine green may be injected intravenously to visualize hepatic perfusion and the demarcation line by negative staining (Figure 2).Finally, the specimen is removed from the abdominal cavity by means of an extraction bag.

Figure 1 Huang’s loop is applied and used when deemed appropriate.
RESULTS
Forty patients underwent RLR for benign or malignant tumors.Overall, the mean age was 59.6 (± 11.8), of which 18 (45%) were female.The mean BMI was 29.4 (± 4.7).Seventeen patients (42.5%) underwent a previous surgery (laparoscopic or “open”).A total of 72.5% (n= 29) of all lesions were malignant (primary lesionsn= 23, metastatic lesionsn= 6).Five lesions (12.5%) were located in the postero-superior segments (IVa, VII and VIII).The patients’ characteristics are summarized in Table 1.
Perioperative outcomes
The type of liver resection, simultaneous combined procedures and outcomes are summarized in Table 2.Nine patients (22.5%) were cirrhotic and another 22.5% had moderate to severe hepatic steatosis.Seven (17.5%) major hepatectomies were performed, of which five were left hepatectomies and two right hepatectomies.Additionally, thirty-three (82.5%) minor hepatectomies were performed: Ten segmentectomies, three wedge resections, ten left lateral sectionectomies, six bisegmentectomies (two V-VI bisegmentectomies, four IVb-V bisegmentectomies), two right posterior sectionectomies and two right anterior sectionectomies.Two patients underwent a simultaneous resection of the primary tumor and the metastatic liver lesions.Of these, one underwent a distal pancreatectomy with splenectomy and anatomic right hepatectomy and the other underwent a low anterior resection with hepatic wedge resection.Only one patient was converted to the “open” approach due to hemorrhage.Based on the IWATE criteria, 3/40 operations were categorized as low difficulty, 19/40 as intermediate, 13/40 as advanced and 5/40 as expert (see Figure 3).
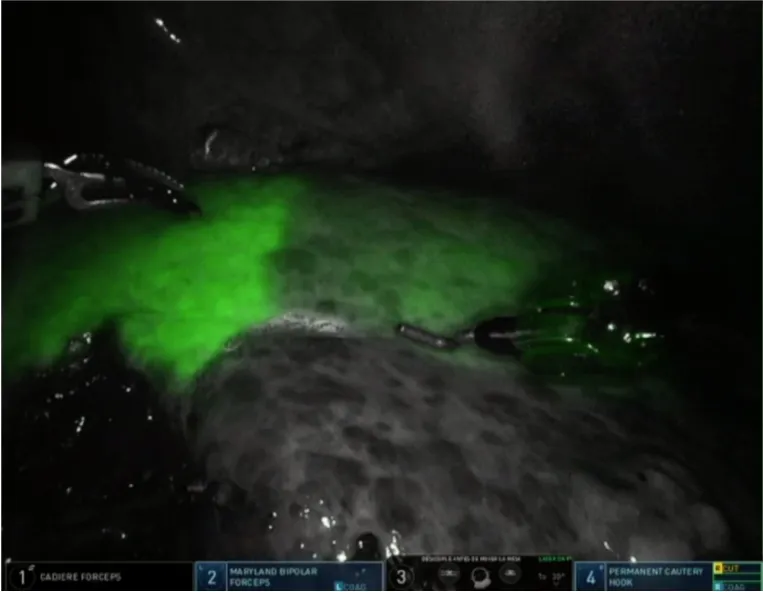
Figure 2 Demarcation line by indole cyanide green negative staining of anatomic segment 3 resections.
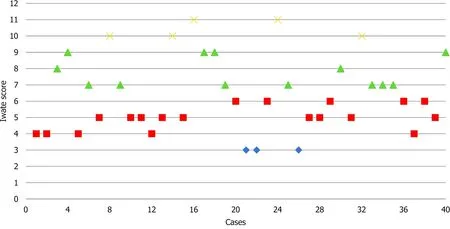
Figure 3 Consecutive case series and degree of difficulty according to the IWATE score.
Eight patients developed complications and are summarized in Tables 2 and 3.Major complications (Clavien-Dindo > III) occurred in three patients (7.5%).Postoperative complications included ascites (1), ileus (1), acute renal injury (1) and bile leak (2), for which one patient required endoscopic retrograde cholangiopancreatography.One cirrhotic patient who underwent a right hepatectomy developed post-hepatectomy liver failure, ascites, acute kidney injury and lower gastrointestinal bleeding with no findings at colonoscopy.
The mean operative duration was 247.6 (± 119.2) min.Inflow occlusion was used in 30 cases (75%) and mean total clamping time was 32.6 (± 26.6) min.Two patients were transfused intraoperatively (5%) and vasopressors were used intraoperatively in fourteen cases (35%).The overall mean length of stay was 5.6 (± 6.1) d, while for minor hepatectomies was 4.4 (± 3.6) d and for major hepatectomies was 14 (± 12.6) d.
The pathologic findings are summarized in Table 4.The mean number of lesions was 1.2 (± 0.7), the mean size was 60.6 (± 40.5) and R0 resection was performed in twenty-seven (93%) of malignant cases.Of the forty operations, the most common diagnoses were as follows: Sixteen (40%) hepatocellular carcinoma, six (15%) intrahepatic cholangiocarcinoma, five (12.5%) colorectal metastases and four (10%) giant hemangiomas.
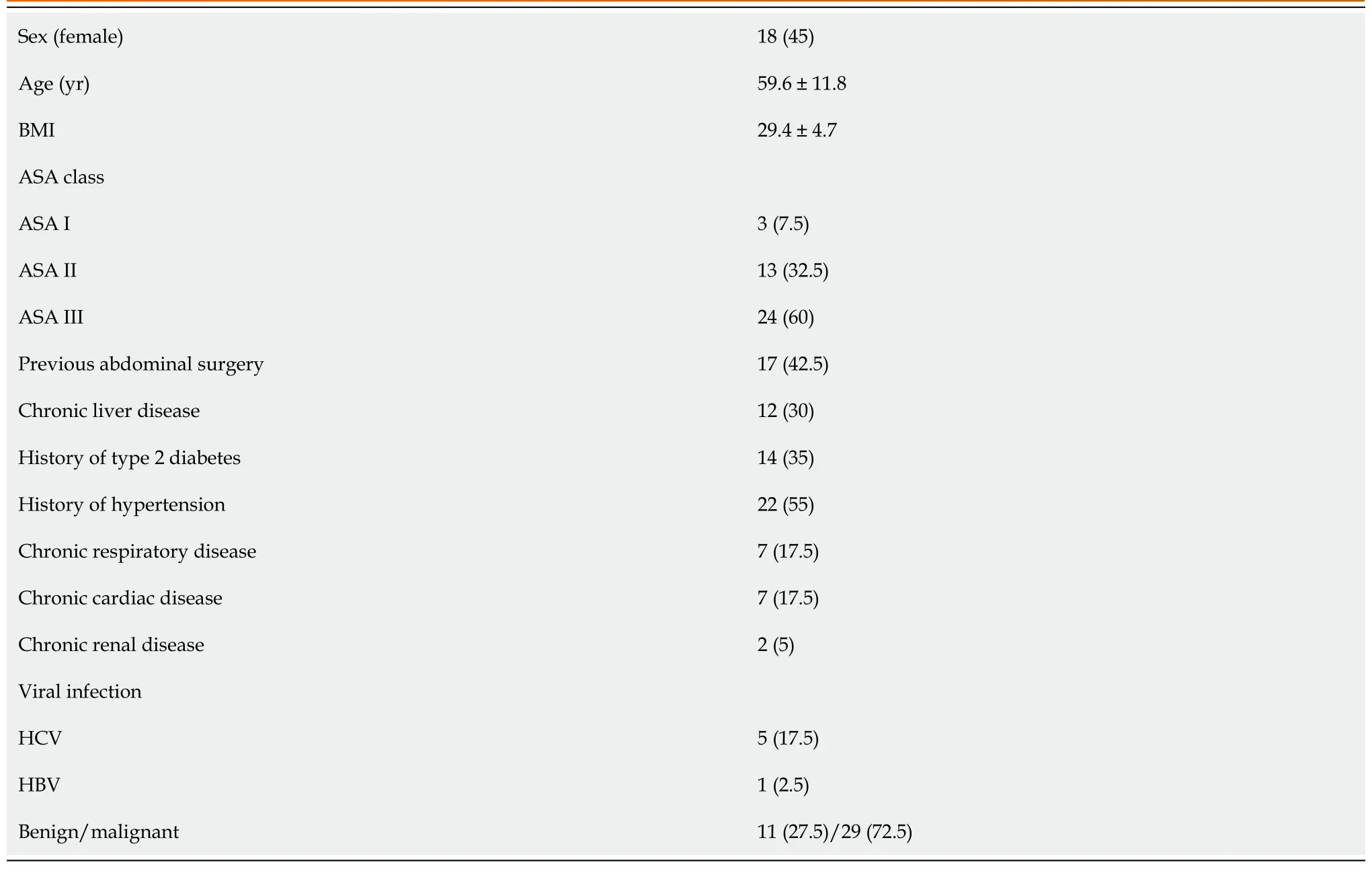
Table 1 Patient demographics and chronic preoperative conditions, n (%)

Table 2 Type of liver resection

Table 3 Perioperative and postoperative outcomes

Table 4 Pathologic examination
DISCUSSION
The minimally invasive approach in liver surgery has revolutionized the management of patients with liver tumors due to its demonstrated superiority over open surgery in terms of hospital stay, morbidity and blood loss[12,13].
Despite the exponential increase in laparoscopic liver surgery in recent years, the development of this surgical procedure has been a real challenge and even today the majority of hepatectomies performed by laparoscopy are the least complex, while major LLRs are still performed in few expert centers.A recent meta-analysis has demonstrated similar outcomes between laparoscopic and robotic major hepatec-tomies[14].Most procedures were performed in specialized centers by liver surgeons with great previous expertise on minimally invasive surgery, demonstrating a severe complication rate of 6.7% and 3.6%, respectively, and almost zero risk of death.
Certain aspects associated with the laparoscopic approach, such as unstable cameras, rigid instruments with reduced degrees of freedom, human hand tremors, poor surgeon ergonomics and the difficulty of suturing in hard-to-reach locations constitute a serious limitation for performing complex hepatectomies[15].Robotic systems have compensated for the limitations inherent in the laparoscopic approach as they use stable, 3D high-definition cameras that eliminate hand tremors and provide 7 degrees of freedom, thus increasing manual dexterity and facilitating liver resections.Moreover, it has been shown that robotic platforms reduce physical workload and are less strenuous for surgeons, so they may reduce musculoskeletal strain and disorders[16,17].
In this study, we present our initial experience in robotic liver surgery.Comparing our experience with those reported by other specialized centers, some have performed a greater number of RLRs, but the study interval is greater[18-25].In our series, forty RLRs were performed in 18 mo and included major hepatectomies and cirrhotic patients.Most of the patients were overweight, middle-aged men, the majority of whom were ASA class III and had several comorbidities.Resections were mainly performed for malignant lesions, with hepatocellular carcinoma, intrahepatic cholangiocarcinoma and colorectal metastases being the most common diagnoses.Two patients underwent a simultaneous resection of the primary tumor (distal pancreatectomy and low anterior resection) and liver metastasis.
Resections for liver metastases were only performed in the absence of peritoneal carcinomatosis or unresectable extrahepatic disease.All patients with malignant disease except two had negative margins after the resection.Of the total number of patients, eleven (27.5%) had benign indications for liver resections.Benign lesions were resected because of severe symptoms caused by tumor size, radiological features of malignancy or diagnostic uncertainty despite preoperative biopsies and underwent anatomic resection.
Regarding the type of resection performed, left lateral sectionectomy (25%) and segmentectomy (25%) were the most frequently performed resections.To study the complexity of the RLRs performed, we employed the IWATE score.The effectiveness of the IWATE score as an indicator of operative difficulty in LLR has been demonstrated and several groups have previously considered that its usefulness in laparoscopic liver surgery could be extrapolated to the robotic approach[26,27].In this study, 45% of the procedures were classified as advanced and expert.These percentages are similar to those of Labadieet al[26] (43%) and lower than the data reported by Sucandyet al[27] (68.6%).As can be seen in Figure 3 showing the cases performed to date and their degree of difficulty, the 45% of RLRs performed were classified as advanced and expert.In our experience, this is due to two reasons: The advantages of the robotic approach for surgeons and the extensive background of our group in laparoscopic liver surgery, which has provided the surgeons an understanding of the specific features and difficulties of this minimally invasive approach.In the coming years, the IWATE score will likely have to be adapted to robotic-assisted liver surgery, as this approach allows accessing posterior superior segments but shows difficulties associated with the resection of various lesions in different quadrants.RLR may favor the operative feasibility of highly difficult resections reducing the conversion rate and increasing safety.However, it does not translate directly into a postoperative course more favorable than pure laparoscopy, as we are still comparing two minimally invasive approaches[28].
Although the overall complication rate was 20%, major complications (Clavien-Dindo > III) occurred in three patients (7.5%).The postoperative complication rate in our study (20%) is similar to that published in a recent metanalysis by Guanet al[29] (19.2%), which included 435 RLRs.Reported conversion rates range from 0%-6%[18,19,21,22,30].The only conversion to the “open” approach in our series (2.5%) occurred in a cirrhotic patient due to hemorrhage from a right inferior hepatic vein during a segment VI resection which required a cava vein venorrhaphy.The only death in our series occurred in a patient with a previous history of autoimmune vasculopathy who underwent a segment VI segmentectomy.The patient developed pancolonic ischemia at postoperative day 7 requiring intervention and died 18 d after being admitted to the Intensive care unit due to massive intestinal ischemia.
The main limitations to the present study are its single-arm design, the relatively small sample size and the retrospective nature of the analysis despite prospective recording.The lack of financial costs and quality of life analysis prevent a deeper investigation.
CONCLUSION
The results reported in this initial case series reflect perioperative outcomes similar to those published previously which support the safety and feasibility of this approach in liver surgery.Previous experience in minimally invasive liver surgery is necessary to overcome the initial difficulties of the robotic approach and perform complex liver procedures in a short period of time.
ARTICLE HIGHLIGHTS
Research perspectives
Future work is required to clarify the role of the robotic approach in complex hepatectomies.
Research conclusions
The implementation of a liver robotic surgery program is safe and feasible with favorable short-term outcomes.
Research results
Forty consecutive patients underwent robotic liver resection between June 2019 and January 2021.Liver resection included: Ten segmentectomies, three wedge resections, ten left lateral sectionectomies, six bisegmentectomies (two V-VI bisegmentectomies and four IVb-V bisegmentectomies), two right anterior sectionectomies, five left hepatectomies and two right hepatectomies.
Research methods
In this study patients were prospectively followed and retrospectively reviewed.The study was conducted according to STROBE statements.
Research objectives
The authors aimed to analyze the outcomes and feasibility of an initial robotic liver surgery program implemented in an experienced laparoscopic hepatobiliary center.
Research motivation
A robotic liver surgery program has been implemented in our center which has significant previous experience in minimally invasive surgery.
Research background
In recent years, minimal invasive liver surgery has notably increased due to its perioperative and postoperative favorable outcomes.
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis C virus: A critical approach to who really needs treatment
- Current aspects of renal dysfunction after liver transplantation
- Hepatitis C: Problems to extinction and residual hepatic and extrahepatic lesions after sustained virological response
- Metabolic and nutritional triggers associated with increased risk of liver complications in SARS-CoV-2
- Recent updates on progressive familial intrahepatic cholestasis types 1, 2 and 3: Outcome and therapeutic strategies
- Targets of immunotherapy for hepatocellular carcinoma: An update