Current aspects of renal dysfunction after liver transplantation
2022-02-12MarianaPachecoLuizAugustoCarneiroAlbuquerqueDanielMazo
Mariana P Pacheco, Luiz Augusto Carneiro-D'Albuquerque, Daniel F Mazo
Mariana P Pacheco, Daniel F Mazo, Division of Clinical Gastroenterology and Hepatology, Department of Gastroenterology, University of São Paulo School of Medicine, Sao Paulo 05403-900, Sao Paulo, Brazil
Luiz Augusto Carneiro-D'Albuquerque, Division of Digestive Organs Transplant, Department of Gastroenterology, University of São Paulo School of Medicine, Sao Paulo 05403-900, Sao Paulo, Brazil
Daniel F Mazo, Division of Gastroenterology, Department of Internal Medicine, School of Medical Sciences of University of Campinas, Campinas 13083-878, Sao Paulo, Brazil
Abstract The development of chronic kidney disease (CKD) after liver transplantation (LT) exerts a severe effect on the survival of patients.The widespread adoption of the model for end-stage liver disease score strongly impacted CKD incidence after the procedure, as several patients are transplanted with previously deteriorated renal function.Due to its multifactorial nature, encompassing pre-transplantation conditions, perioperative events, and nephrotoxic immunosuppressor therapies, the accurate identification of patients under risk of renal disease, and the implementation of preventive approaches, are extremely important.Methods for the evaluation of renal function in this setting range from formulas that estimate the glomerular filtration rate, to non-invasive markers, although no option has yet proved efficient in early detection of kidney injury.Considering the nephrotoxicity of calcineurin inhibitors (CNI) as a factor of utmost importance after LT, early nephroprotective strategies are highly recommended.They are based mainly on delaying the application of CNI during the immediate postoperativeperiod, reducing their dosage, and associating them with other less nephrotoxic drugs, such as mycophenolate mofetil and everolimus.This review provides a critical assessment of the causes of renal dysfunction after LT, the methods of its evaluation, and the interventions aimed at preserving renal function early and belatedly after LT.
Key Words: Liver transplantation; Acute kidney injury; Chronic kidney disease; Calcineurin inhibitor; Mycophenolic acid; Everolimus
INTRODUCTION
Liver transplantation (LT) changed the natural history of cirrhotic patients.It is considered the gold standard treatment for liver diseases on terminal stages, including hepatocellular carcinoma[1,2].Significant advances were achieved in immunosuppression, in the treatment of acute and chronic cellular rejection, in the prevention of infections, and in preoperative preparation, organ preservation, surgical procedure, and anesthesiologic techniques[1].Therefore, short-term mortality, which was due mainly to intraoperative causes, infection, and acute rejection, has considerably decreased[1].On the other hand, long-term mortality has not been altered for the past few years[3].Longer survival rates have, in turn, increased the so-considered late complications of LT, such as diabetes mellitus, cardiovascular diseases, malignance, and renal dysfunction[1,4].
Chronic kidney disease (CKD) develops in the majority of patients who survive the first 6 postoperative months[5,6].The cumulative incidence of post-LT CKD is significantly higher than those following cardiac and lung transplants[5].The presence of CKD post-LT, defined by the Chronic Kidney Foundation as the reduction of the glomerular filtration rate (GFR) to values lower than 60 mL/min/1.73 m² for 3 mo or longer, is a frequent complication and has a negative impact on the graft’s and patient’s survival rates[7].A recent study from the United States assessed 602 liver transplanted patients between 2010 and 2016 and reported a prevalence of CKD in its distinct stages in 41.5% of recipients[8].In addition, renal failure was responsible for 6% of deaths of patients who survived the first 6 post-transplantation months[8].
Prevalence and incidence studies of post-LT renal dysfunction show wide variations, attributable mainly to different criteria used for CKD definition, and to the various follow-up periods evaluated[9].The first consensus of the International Liver Transplantation Society reported that the prevalence of post-LT CKD ranged between 30% and 90%, and terminal CKD that required renal replacement therapy (RRT) was described in 2% to 5% of patients per year[10].According to the Scientific Registry of Transplantation Recipients, the incidence of stage 4 or 5 of CKD after 1, 3, and 5 years of transplantation was 8%, 14%, and 18%, respectively, reaching up to a quarter of recipients within 10 years after the transplant[5,7].An extensive prospective study evaluated the prevalence of CKD through measurement of GFR by iothalamate clearance and the associated mortality in 1211 patients over 25 years[9].The authors reported that after 4 mo of LT, 40% of the patients already had CKD stage ≥ 3, and the risk of death increased when the GFR decreased to values below 30 mL/min/1.73 m2or worse[9].Only 18% of the subjects had normal renal function after 25 years, in opposition to 39% of age-group matched individuals from the general population[9].
When the whole spectrum of renal dysfunction after LT is evaluated, few studies exhibit data of its occurrence in the early stages after the procedure.A Spanish study with 230 patients revealed that 30.8%, 28.8%, and 26.4% of patients had stage 3 CKD after 12, 24, and 30 mo of transplantation, respectively[11].It is interesting to highlight that, despite a mild reduction in GFR (60-89 mL/min/1.73 m2) is not considered CKD, this same Spanish study observed that a significant percentage of patients had this GFR range (46.2%, 41.9%, and 46.2% within 12, 24, and 30 mo after the transplant, respectively), even with normal GFR prior to LT[11].In the American cohort, this mild reduction in GFR occurred in 21.7% of patients who had controlled blood pressure, and in 24.9% of patients with uncontrolled blood pressure within 1 year after LT[8].
Renal dysfunction etiologies in LT are multifactorial and are related to the period of its occurrence.Therefore, the main factors leading to renal dysfunction can be grouped into pre-LT, intraoperative, and post-LT periods (Table 1).Though efforts have been made to reduce or avoid such predisposing factors of renal dysfunction, many of them are not modifiable, such as, for instance, pre-existing conditions.

Table 1 Main causes of kidney dysfunction in liver transplantation according to the period of its occurrence
CAUSES OF RENAL DYSFUNCTION IN LT
Pre-transplantation
Acute kidney injury (AKI) is a common and increasing clinical event in subjects with cirrhosis[12].It is estimated to occur in 20% to 57% of hospitalized subjects with decompensated liver disease, with a significant impact on survival[12-14].AKI in this setting is an underestimated problem because the main assessed parameter is the serum creatinine (Scr).Scr overestimates GFR for several reasons, such as muscle mass, frequently reduced in patients with cirrhosis[15].In advanced liver disease, the presence of AKI is common, often secondary to infection, hypovolemia, use of vasodilators, and other nephrotoxic drugs, such as non-steroidal anti-inflammatory agents and contrasts.Nonetheless, particularly in those with advanced decompensated liver disease, one of the main causes of loss of renal function is the circulatory dysfunction induced by portal hypertension[16].Activation of the renin-angiotensinaldosterone system (RAAS) leads to kidney vasoconstriction, which may be reverted with the resolution of the portal hypertension, as seen in cases of hepatorenal syndrome (HRS)[16].The understanding of the pathophysiology of HRS-AKI has evolved and currently encompasses, in addition to circulatory dysfunction, systemic inflammation, microvascular dysfunction, and direct tubular damage[17-19].The combination of albumin and terlipressin can restore renal function in 40% to 73% of patients with HRS-AKI[20-23].Moreover, response to terlipressin and albumin was associated with a reduction in the need for RRT after LT and reduced the risk of CKD at 1 year after LT, as recently reported by Pianoet al[24].However, LT remains the definitive treatment for this condition.On the other hand, renal vasoconstriction for extended periods, associated with the intrinsic kidney damage caused by the surgical procedure, may lead to organic and less reversible renal injury, which explains why some patients with HRS develop worse renal function after LT[16].Indeed, nonrecovery of renal function is associated with the duration of pre-LT dialysis in HRS patients[25].In addition, renal recovery and patient survival post-LT are better in those with HRS than in those with acute tubular necrosis[26].
It is noteworthy that AKI is an increasingly recognized risk factor for CKD development and progression[27].A recent Spanish study reported that in a cohort of patients with cirrhosis who survive an episode of AKI, 25% of them developed CKD, and this passage from AKI to CKD was associated with an increased risk of AKI, complications of cirrhosis, and hospital re-admissions[28].According to Francoz[29] (2020), cirrhosis, in addition to being a risk factor for AKI, would also be a predisposing condition for the development of CKD, with an impact on those needing LT.
Some renal parenchymal chronic diseases relatively specific to cirrhosis, such as immune complex glomerulonephritis (seen in hepatitis B and C) or immunoglobulin A nephropathy (seen in cirrhosis due to alcohol), are increasingly found in candidates for LT[16].However, non-specific causes of CKD, mainly secondary to metabolic syndrome, are also increasingly seen in this population[30].Special attention must be paid to subjects with non-alcoholic steatohepatitis (NASH)/metabolic dysfunctionassociated fatty liver disease (MAFLD), which represents a growing LT indication worldwide[31-33].These patients have additional risk factors for renal injury, such as diabetes, hypertension, and obesity, which in turn are associated to some degree with kidney injury in the pre-LT period[34].In addition, it has already been demonstrated that NASH is an independent predictor of stage 3 renal injury post-LT[35].
Finally, the model for end-stage liver disease (MELD) score itself, used for the allocation of organs, which includes Scr in its estimation, favors candidates with renal function impairment for LT.Therefore, its widespread use may increase the number of patients who require RRT and simultaneous liver and kidney transplants, impacting the long-term renal function of the recipients[16,36].The risk of post-LT end-stage renal disease, which is related to post-LT mortality, was 15% higher in the MELD era, as shown by Sharmaet alin 2011[37].Interestingly, the proportion of MELD sodium score attributable to creatinine ≥ 50% was associated with advanced renal dysfunctionat 1 year post-LT in a recent United States retrospective study using the United Network for Organ Sharing (UNOS) database[38].
Altogether, these factors in the pre-LT period contribute to the increased finding of renal dysfunction after LT.
Perioperative
The development of renal injury in the perioperative period leads to extended hospitalization, increases the risk of acute rejection and infection, and impacts global mortality[39].Renal dysfunction during this period has a reported incidence of 11% to 94%, depending upon the definition and the assessment method applied[40], with acute tubular necrosis as the most frequent etiology[6,16].Risk factors for perioperative AKI include sepsis, nephrotoxic drugs, impairment of renal perfusion associated with hemodynamic instability during surgery, and the harmful effect of the ischemia-reperfusion injury[6,41].
High perioperative aminotransferase aspartate peak is independently correlated with the risk of renal injury after LT[6,42].The use of blood transfusion in the intraoperative period, especially above 10 units, increased the risk of renal dysfunction when combined with diuresis lower than 100 mL/h[43].The excessive use of blood products may be related to large blood losses and, consequently, hypotension, but could also induce a pro-inflammatory state that impairs oxygen supply to tissues and increases the concentration of free hemoglobin and iron, both nephrotoxic[44].
In addition, the lack of grafts forces surgeons to use more marginal grafts (of older patients, with steatosis, and organ donors with circulatory causes of death), which is directly related to reperfusion-ischemia injury[45].This may result in more renal dysfunction posteriorly[46].Predictive models for renal dysfunction have already been assessed, but none of the candidates was capable of adequately predicting the outcome within a time frame suitable for appropriate intervention[40].
Post-transplantation
Up to 1 year: The most common histopathological findings in subjects with CKD 1 year after the LT included calcineurin inhibitors (CNI) toxicity, diabetic nephropathy, and thrombotic microangiopathy[7].
Early nephrotoxicity by CNI is in most part functional, and a dose-dependent mechanism.CNI induce vasoconstriction of afferent and efferent arterioles, with reduction of renal perfusion and of the ultrafiltration coefficient and, consequently, reduction of the glomerular filtration[10,47].Therefore, early renal alteration may be reversible with the reduction of the CNI dose[5].The accurate vasoconstriction mechanism is still unclear, but it is known that there is a disequilibrium of vasoactive substances that lead to the increase of vasoconstrictors, for instance, endothelin, angiotensin II, and thromboxane, and the decrease in the generation of vasodilators, such as prostaglandins and nitric oxide[10,48] (Figure 1).
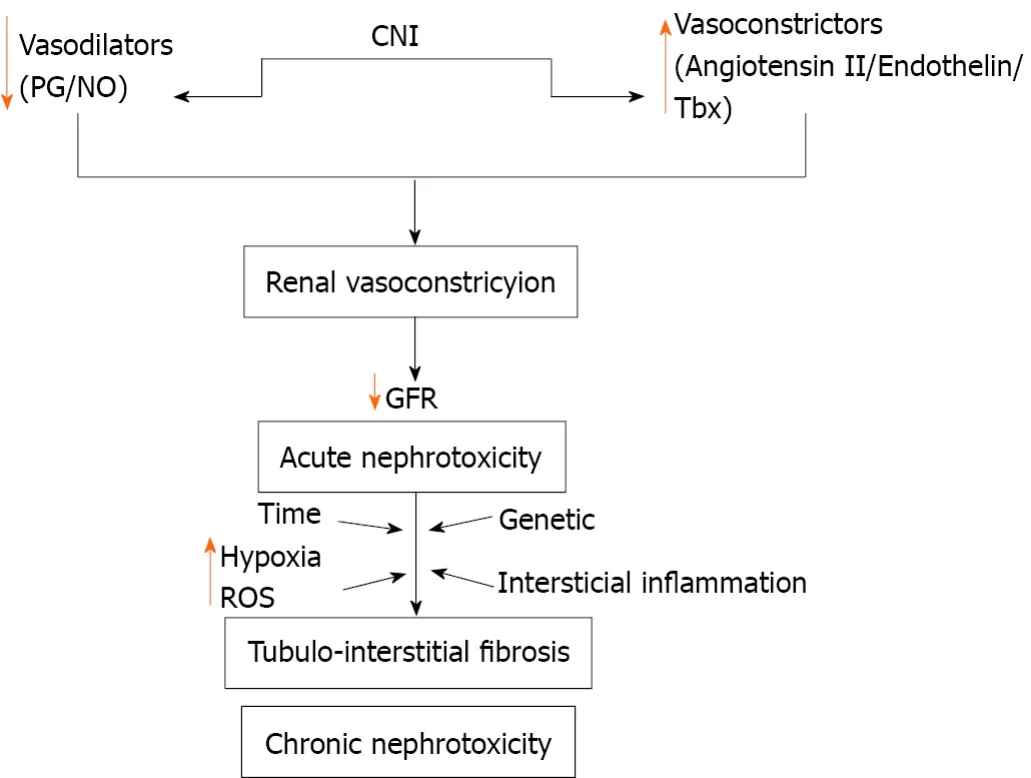
Figure 1 Calcineurin inhibitors nephrotoxicity mechanism.C
A comprehensive study using the UNOS database evaluated 1720 patients with pre-LT renal dysfunction and demonstrated that the most important independent predictor of recovery of renal function, defined as creatinine < 1.5 mg/dL and survival rate greater than 29 d, was the absence of liver graft dysfunction[49].Induction with anti-thymocyte globulin, decreasing the use of CNI, was also considered a protective factor[49].Interestingly, the authors showed that the need for RRT for up to 8 wk was not a contributing factor to CKD evolution[49].In Taiwan, Linet al[50] (2012) reported that the Scr in the 4thwk after LT was a good predictive variable for CKD over 5 years, which implies that the aggressive management of early kidney injury may avoid the development of CKD.Yeet al[51] (2020) described that the estimated GFR at 1 year after LT, beyond the stage at which postoperative complications may occur and with greater immunosuppression stabilization, had a good correlation with the estimated GFR in 5 years.
After 1 year:Unquestionably, the main mechanism of CKD evolution is CNI nephrotoxicity.It is estimated that in about 50% of patients who develop renal dysfunction in the postoperative period, CNI nephrotoxicity is the root cause[6].Gonwaet al[52] (2001) evaluated 843 liver-transplanted patients for up to 13 years, and the presumed etiologies of end-stage renal disease that occurred in 45 patients were CNI toxicity (73.3%), progression of subjacent renal disease (11.1%), focal segmental glomerulosclerosis (6.66%), non-recovered HRS (6.66%), and acute tubular necrosis/toxicity of amphotericin (2.22%).In the longer term, diabetes mellitus and high blood pressure worsen renal damage even further[16].As standard immunosuppressive therapy is based upon CNI [tacrolimus (FK) and cyclosporine] monotherapy or is associated with other agents (for instance, mycophenolate)[53], handling such complications is one of the core challenges of physicians who manage liver-transplanted patients.
The chronic renal damage that CNI causes is characterized by the development of irreversible structural injury and may culminate in terminal stages of kidney disease[10].Upon histology evaluation, obliterative arteriopathy, glomerular ischemic collapse, tubular vacuolization, and focal areas of tubular atrophy and interstitial fibrosis may occur[10].The development of chronic nephropathy induced by CNI is also influenced by genetic variability[54].The factors responsible for chronic injury by CNI are complex and not completely understood, and involve interstitial inflammation and renal vasoconstriction, with activation of the RAAS in a relevant manner (Figure 1).Consequently, there is an imbalance between vasodilator and vasoconstrictor factors, leading to renal damage[10].Another possible mechanism generated by CNI nephrotoxicity is the direct injury of tubular epithelial cells, derived from the blocking of mitochondrial permeability and inhibition of prolyl isomerase, the enzyme responsible for the interconversion of the cis- and trans-isomers of peptide bonds, which can speed up or slow down protein cleavage[55].
The previously mentioned study from Yeet al[51] (2020) also evaluated several predictive factors of the evolution to CKD in post-LT patients under the FK regimen[51].The authors reported that the GFR found 1 or 2 years after LT showed a good correlation with the one found after 5 years, and demonstrated that those subjects with GFR < 60 mL/min/1.73 m² are those who will probably develop an irreversible renal injury in the following years.It is important to highlight that while statistical significance was not found in the annual reduction of the GFR between FK-using and FK-free groups, the serum concentration of FK influenced the progression to CKD within 1 and 2 years, with receiver operating characteristic curves of 0.73 and 0.78, respectively[51].
The development of post-LT metabolic syndrome is frequent[56].In addition to lingering pre-LT risk factors, there is an increase in post-LT risks due to immunosuppression with corticosteroids and CNI[57].Moreover, it is expected that metabolic syndrome components after LT will continue to rise due to the increase of NASH/MAFLD as an indication for LT[31-33,58].VanWagneret al[8] (2020) reported that hypertension was observed in up to 92% of patients and diabetes in 53%, adding risk to the development of CKD in such patients.Moreover, there is the possibility of an evolution to advanced liver fibrosis/cirrhosis, which adds renal dysfunction components of cirrhotic patients to those associated with immunosuppression.
METHODS OF ASSESSMENT OF RENAL FUNCTION
Due to the multifactorial nature of CKD in the post-LT period, the ability to accurately identify patients under risk and the development of preventive strategies are crucial[59].The discovery of a more sensitive biomarker would make it feasible to quickly detect renal damage factors and implement early therapeutic interventions.To assess renal function after LT, the GFR measurement is the most used laboratory tool[60].For such, the most commonly used test in clinical practice is the dosage of Scr, which supplies information about GFR and is widely available and inexpensive[7,60].Nevertheless, besides considerations concerning analytical aspects of the test, there are individual characteristics that may interfere with the results.Reference Scr values are influenced by non-renal factors, such as body weight, muscle mass, race, age, gender, and protein intake[61].In this way, Scr values differ among children and adult women and men[61].Scr is also considered a late renal dysfunction marker, requiring a reduction above 50% of glomerular ultrafiltration before an increase in Scr is observed[60].Accuracy can be improved through measurement of 24 h creatinine clearance, but it also brings limitations: Higher costs, the need to store urine for 24 h (subject to errors in sample collection and incomplete bladder emptying), and the effect of tubular secretion of creatinine[61].As it is a small molecule and does not bind to serum proteins, creatinine is freely filtrated by glomeruli; however, about 10% to 20% of the creatinine excreted in urine comes from its secretion by the proximal tubular cell.Tubular secretion is the main determinant of the overestimation of renal function when creatinine clearance is used[62].This secretion by the tubular cell is variable in the same individual and increases with the reduction of the glomerular filtration[60-62].
Equations specifically developed for the estimation of creatinine clearance, such as Cockcroft-Gault[63] or the Modification of Diet in Renal Disease (MDRD)[64], have been widely used in clinical practice[60].MDRD-4 (simplified MDRD) is the equation usually employed to compute GFR because it is considered to be as accurate as MDRD-6, the original equation[65].Indeed, there are undeniable advantages to its use, but despite its generalized use in clinical practice, the measurement of GFR through formulae is not accurate, particularly in patients with uncommon biotypes or diet alterations, in the presence of rapid deterioration of renal function, or when the GFR values are above 60 mL/min/1.73 m²[62].
The 2012 joint guideline of the American Society of Transplantation along with the American Association for the Study of Liver Diseases (AASLD) recommended the use of the MDRD equation in any of its four variations as superior to the use of the isolated Scr and of the 24 h creatinine clearance[66].Nevertheless, in 2016 the American Society of Transplantation developed a document that specifically endorsed the use of MDRD-4 and CKD-epidemiology-creatinine[67] as the formula that yields the most accurate results of GFR in this population[68] (Table 2).The 2019 British guideline for post-LT management advised that close monitoring of renal dysfunction after LT is necessary, but did not cite which method to use in the evaluation[69].
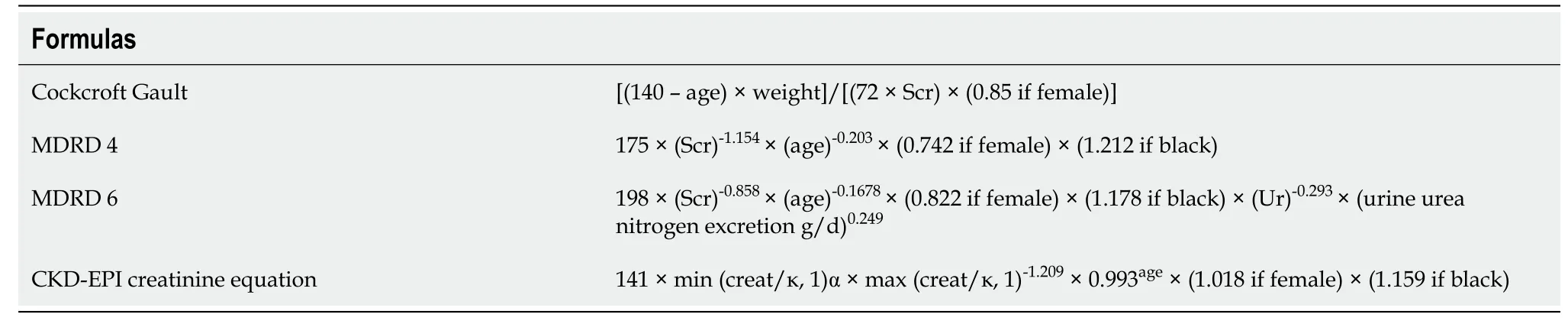
Table 2 Main formulas for measurement of glomerular filtration rate
Due to the antiproteinuric effect of CNI, proteinuria may be absent even in advanced stages of CKD[66].The AASLD guideline recommends its measurement in isolated samples at least once per year[66].
Cystatin-C is placed as an alternative glomerular filtration marker because, as it can be completely eliminated in the circulation, its serum concentration could properly reflect the GFR[70].Unlike creatinine, it is not influenced by muscle mass, diet, or the presence of infection or malignance[60,70].However, other factors, such as age, male gender, weight, height, tobacco use, steroid use, and thyroid disease, are independently associated with elevated cystatin-C levels, suggesting low specificity in detecting renal impairment[60].The 2016 guideline of the American Society of Transplantation states that among all blood-based estimates of GFR, the cystatin-C equations are the most accurate in post-LT patients[68].
Renal clearance of inulin is the gold standard of GFR measurement, but the necessity of performing a test in standardized conditions, with continuous intravenous injection of the marker, its elevated cost, and peculiar aspects of laboratory dosage limit its use in clinical practice, restricting it to research settings[71].The use of renal and plasma clearance of radioactive isotopes, such as51Cr-ethylenediamine tetraacetic acid (EDTA), is growing in clinical practice, as they are safer and simpler methods -and were sufficiently accurate - to measure GFR[71].Despite the ongoing discussion about the underestimation of renal clearance of51Cr-EDTA in comparison to renal clearance of inulin, the determination of GFR by51Cr-EDTA and by inulin had comparable results in kidney-transplanted patients[72].The authors have shown elevated correlation coefficients between both methods (0.9516)[72].Only a few studies used51Cr-EDTA clearance measurement to evaluate GFR in children and adults post-LT[73-76].
Neutrophil gelatinase-associated lipocalin (NGAL), a protein expressed in the renal tubular cells, has been gaining attention as an early marker of AKI, including the immediate post-LT period, though there is still considerable variation among studies[77].In a Japanese study, Tsuchimotoet al[78] (2014) reported that NGAL was the best urinary marker in comparison to 5 other assessed candidates [liver-type fatty acid binding protein, monocyte chemoattractant protein-1, interleukin (IL)-18, cystatin-C, and osteopontin], with its values in the 1stand 7thpostoperative days being helpful to predict AKI by FK in liver-transplanted patients.In 2019, Limaet al[79] evaluated the urine and plasma NGAL elevation pattern in the LT perioperative period of 100 patients and showed that these measurements were able to predict AKI diagnosis earlier in this setting.Urinary NGAL levels evaluated just after the LT procedure could accurately predict AKI development in 27 subjects in the United Kingdom, as Robertsonet al[80] reported in 2019.NGAL could also be useful in the context of chronic renal injury, not only to predict its progressions but also to monitor the response to treatment aimed at protecting renal function[60,81,82].However, changes in urinary NGAL are not specific to CKD, and more studies are required to further explore its potential in the context of LT[83].The utility of NGAL and other urinary and serum biomarkers for the prediction of AKI in patients undergoing LT has yet to be defined because AKI pathogenesis in this context is complex[84].Moreover, optimal cut-off values and source of confounding factors must be addressed prior to routine clinical use in LT[60,77].
The use of imaging tests for kidney evaluation, under several clinical situations, is a well-established method.In adults, the ultrasound exam finding of a more echogenic renal cortex as compared to liver echogenicity clearly suggests renal disease[85-87].It is a very sensitive marker of renal parenchymal disease and correlates well with some glomerular and tubular-interstitial injuries[87].Recent studies displayed the role of magnetic resonance imaging (MRI) in evaluating hypoxia and fibrosis of the renal parenchyma through 2 techniques (blood oxygen level-dependent MRI and diffusionweighted MRI).Both provided information on the progression of kidney disease[88].The standardization of acquisition and processing protocols is required, as current methodological differences exist across studies and pose difficulties in comparing the results[88].In addition, kidney evaluation data in liver-transplanted patients are awaited, as the non-invasive assessment of renal changes by magnetic resonance diffusion imaging has so far been evaluated only after lung transplantation[89].
Acoustic radiation force impulse (ARFI) is a recently developed noninvasive technique.It is safe and convenient to assess the elasticity of tissues[90].The technique is capable of identifying the parenchymal elasticity by measuring the speed of the shear wave, and it is integrated into conventional ultrasound devices[91].It has been used mainly in the determination of hepatic fibrosis and cirrhosis in chronic viral hepatitis and displays a good correlation with the degree of liver fibrosis[92,93].In recent years, the ARFI technique has also been applied to other organs, such as the muscles[94], prostate[95], and breast[96].Fibrosis is the core process of the progression of CKD and this method has also been evaluated in this scenario.Despite the inability to predict pathological alterations, ARFI results were significantly correlated with GFR and the stage of CKD in several studies[97].However, kidney hemodynamical alterations may affect the renal parenchymatic elasticity during CKD progression[97].In a pilot study, Bobet al[98] (2015) reported that ARFI measurements diminished with the decrease in GFR, suggesting a cutoff at 2.26 m/s or less as a predictor of stage 4 or 5 CKD.Structurally, the finalviaof post-LT CKD culminates in kidney fibrosis and, similar to what happens in other organs such as the liver, the collagen deposition may culminate in an increase in tissue stiffness.Therefore, elastography techniques could play a role in this setting.
STRATEGIES FOR PREVENTING POST-TRANSPLANTATION CHRONIC RENAL DISEASE
Patients developing CKD, besides having limitations regarding the use of immunosuppressing drugs, exhibit an increased risk of hospitalization, infectious complications, and graft dysfunction.Moreover, they have a 2 to 4 times greater risk of death[5,99].Thus, preventive strategies to preserve kidney function after LT are paramount.The management of comorbidities and other general factors leading to CKD must be remembered.Therefore, it is possible to extrapolate non-transplanted CKD orientations to these patients[100].It is advisable to, at least once per year, measure or calculate GFRviaformulae, besides performing albuminuria or proteinuria tests and, if necessary, referring the patient to a nephrologist (Table 3).

Table 3 Referral to specialized kidney care services
Regarding arterial hypertension, the pressure target should be below 140/90 mmHg in the absence of proteinuria, and below 130/80 mmHg when it is present[66,68].These objectives must be reached with a combination of lifestyle changes and pharmacological options.The choice of the anti-hypertensive must be based upon safety and drug interaction[69].Dihydropyridine calcium channel blockers, such as amlodipine, are considered first-choice agents, as they reduce systemic vascular resistance and improve renal blood flow, thus blocking CNI’s vasoconstrictor action[68,69].Drugs that block the RAAS, such as angiotensin converting enzyme inhibitors and angiotensin receptor blockers, must be avoided in the immediate postoperative period because, in this period, the activity of plasmatic renin is decreased and their use may worsen the hyperkalemia observed with FK use[69].After this period, these drugs are of choice for patients with diabetes, significant proteinuria, and CKD[66,68,69].Beta blockers are safe, but diuretics must be employed with caution, as they may further affect renal function[69].Cardiovascular complications are frequent non-graft-related causes of mortality after LT, and it has already been shown that the mean GFR is inversely proportional to the time of the first cardiovascular event[6,101].In these cases, immunosuppression based on everolimus, with the withdrawal or reduction of FK, improved both renal function and the risk of major cardiac events in comparison to standard therapy, as shown by Salibaet al[101].
Post-LT diabetes treatment must target an Hb1AC below 7.0%[66].Though there is no consensus about which is the best antidiabetic, it is advisable to decrease or interrupt corticosteroids as soon as possible[66,69].When corticosteroids are administered at higher doses, the use of insulin is safer and more efficient[66].
Dietary interventions may help to slow down CKD’s progress.Salt intake should be restricted to less than 2 g of sodium per day to better control blood pressure and proteinuria[69,102].Other interventions with less evidence would be to avoid high protein intake (less than 1.3 g/kg/d) in subjects at risk of CKD and to further reduce it to 0.8 g/kg/d in those with GFR < 30 mL/min/1.73 m²[102].Post-LT weight gain is also associated with the development of metabolic syndrome, cardiovascular events, and renal dysfunction[103,104].Therefore, weight gain should be avoided.Charltonet al[105] (2017) demonstrated that the introduction of everolimus as an attempt to reduce the FK dosage decreased the weight gain of patients within 1-2 years after LT.
Liver-transplanted patients are particularly vulnerable to hemodynamic insults and present an increased risk of developing AKI after exposure to nephrotoxins, such as non-steroidal anti-inflammatory drugs, amphotericin B, aminoglycosides, and contrast agents.Whenever possible, therapy with CNI before and after exposure to potential nephrotoxins should be reduced or suspended, and a temporary switch to other nonnephrotoxic immunosuppressors should be considered, due to rejection risks, in addition to other nephroprotective measures established for other patients[100].
CNI-induced nephrotoxicity contributes to the worsening of renal function in both the short and long term; the greatest challenge is the choice of a strategy that minimizes renal dysfunction without simultaneously affecting the survival rate of the liver graft.In the immediate postoperative stage (< 1 mo), a strategy to spare the renal function has been the administration of short-term induction therapy (mono- or polyclonal antibodies), with delayed introduction of CNI[6,69].Several clinical trials have shown that in individuals with preoperative renal dysfunction, this approach resulted in a better renal outcome, as it avoided the vasoconstrictor risks of CNI in synergy with other perioperative risk factors associated with AKI[6,69,106].Basiliximab and daclizumab, which have a selective target upon activated T-cells blocking CD25, the IL-2 receptor, are the most used.The use of belatacept has also been studied, in addition to other standard strategies of induction, but the study had to be terminated due to a higher mortality rate of the belatacept group[107].
Early usage of mycophenolate mofetil (MMF) has also been assessed in subjects without preoperative kidney dysfunction, with an improvement of GFR without disadvantages in terms of graft rejection[108].Thus, reduced FK doses in combination with MMF are capable of protecting renal function more efficiently than isolated FK use[109].
The use of the mammalian target of rapamycin inhibitors (mTor-I) everolimus has also been demonstrated to be a protective renal strategy[110].Everolimus was capable of promoting an early decrease of FK dosage with similar efficiency and safety, and with preservation of renal function[111,112].A continued effect was observed after 1, 2, and 3 years of LT[112].In these studies, in which everolimus was introduced 4 wk after LT, thrombosis of the hepatic artery and impaired wound healing were not observed[111,112].In the PROTECT randomized trial, it was shown that the monotherapy with everolimus displayed better results regarding GFR within 12 mo after LT, with similar mortality, graft rejection, and therapeutic failure rates[111].In addition, maintenance of the GFR benefit in the extension of the study of 24 and 36 mo was observed[113,114].However, infections, leukopenia, dyslipidemia, and treatment discontinuation were higher in the everolimus group[111].
The use of sirolimus, another mTor-I, was also evaluated as a nephroprotective option after LT.A large randomized prospective trial assessed the conversion of CNI to sirolimus in 607 liver-transplanted patients, and a higher rate of acute rejection and discontinuations was observed in the sirolimus group, with no gains regarding the GFR[115].Also, the early use of sirolimus inde novoLT in a phase II trial did not exhibit nephroprotection and showed higher graft loss rates, mortality, and sepsis as compared to the use of tacrolimus at standard doses alone[116].The FDA added a black box warning for the use of sirolimus and belatacept in LT recipients[68].
Therefore, strategies for the primary preservation of long-term renal function are based upon precocious post-operative CNI reduction in combination with nonnephrotoxic immunosuppressing drugs, such as MMF or everolimus, and the use of induction therapy in selected patients[6,66,68,69].
Despite the evidence that early MMF and mTor-I usage minimizes renal dysfunction, this strategy does not seem to be as effective when performed after 1 year from the LT[68].The significant reduction of the CNI dose (below 50% of the original dosage) with the addition of MMF resulted in an improvement of GFR without negatively affecting the graft’s survival rate, and it did not increase the incidence of adverse events, even when it was implemented after 1 year of LT, but with a weaker effect[117-120].Complete withdrawal of CNI increased the risk of rejection and graft loss, without adding gains to the GFR[120,121].Unfortunately, these studies demonstrated that once the renal function is markedly affected (GFR < 60 mL/min/1.73 m²), changing to a kidney preservation approach is less efficient to improve GFR, possibly due to irreversible kidney structural damage[6].Regarding everolimus, the studies revealed no increase in the rate of liver rejection, but they also reported little to no improvement in the GFR (about 4 mL/min)[122-125], with a discontinuity rate above 10% and the development of proteinuria in some recipients[125].Therefore, there is little evidence that the substitution of CNI for mTor-I after 1 year has some benefit for the improvement of renal function[68].Indeed, early rather than late conversion of CNI to everolimus after LT was shown to be a safe approach to preserve long-term renal function, as recently reported by Salibaet al[126] (2020) in the EVEROLIVER Registry.
To minimize the use of CNI, new drugs are currently being tested, such as CFZ533, an IgG1 anti-CD40 antibody, which blocks the signaling pathways implicated in rejection; however, the majority of such studies were in renal transplantation[127,128].Finally, for those patients who develop end-stage renal disease with a need for dialysis, there is a benefit from renal transplantation from either living or deceased donors, with a mortality reduction of 44% to 60% in comparison to those patients who stay in RRT[66,129,130].
CONCLUSION
Post-LT renal dysfunction is a frequent and severe problem, impacting patients’ morbimortality.Its etiology is multifactorial, with pre-, intra-, and post-LT factors.Its incidence is increasing, mainly after the changes in organ allocation by MELD score.Early diagnosis is paramount, but the most conventional methods of estimating GFR have limitations, and there is currently no accurate, non-invasive marker ready to use in clinical practice.Taking into consideration that CNI’s toxicity is an important post-LT cause of renal dysfunction, strategies to minimize its use, such as induction therapy followed by a reduction in CNI levels, and the introduction of less nephrotoxic drugs, such as MMF and everolimus, are still the best options to preserve renal function.Also, aggressive treatment of other comorbidities that can negatively impact GFR is important.Nonetheless, once the renal function is significantly compromised, the adoption of a nephroprotective immunosuppression approach is less efficient.New immunosuppressing drugs that do not lead to GFR impairment and do not increase liver rejection rates are eagerly awaited.
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis C virus: A critical approach to who really needs treatment
- Hepatitis C: Problems to extinction and residual hepatic and extrahepatic lesions after sustained virological response
- Metabolic and nutritional triggers associated with increased risk of liver complications in SARS-CoV-2
- Recent updates on progressive familial intrahepatic cholestasis types 1, 2 and 3: Outcome and therapeutic strategies
- Targets of immunotherapy for hepatocellular carcinoma: An update
- Redefining non-alcoholic fatty liver disease to metabolic associated fatty liver disease: Is this plausible?