Prognostic factors of survival and a new scoring system for liver resection of colorectal liver metastasis
2022-02-12KaiChiChengAdaSzeManYip
Kai-Chi Cheng, Ada Sze-Man Yip
Kai-Chi Cheng, Ada Sze-Man Yip, Department of Surgery, Kwong Wah Hospital, Hong Kong, China
Abstract BACKGROUND Hepatic resection has become the preferred treatment of choice for colorectal liver metastasis (CLM) patients.AIM To identify the prognostic factors and to formulate a new scoring system for management of CLM.METHODS Clinicopathologic and long-term survival data were analyzed to identify the significant predictors of survival by univariate and multivariate analyses with the Cox model.A clinical score was constructed based on the analysis results.RESULTS Three factors of worse overall survival were identified in the multivariate analysis.They were number of liver metastases ≥ 5, size of the largest liver lesion ≥ 4 cm, and the presence of nodal metastasis from the primary tumor.These three factors were chosen as criteria for a clinical risk score for overall survival.The clinical score highly correlated with median overall survival and 5-year survival (P = 0.002).CONCLUSION Priority over surgical resection should be given to the lowest score groups, and alternative oncological treatment should be considered in patients with the highest score.
Key Words: Colorectal cancer; Liver metastasis; Liver resection; Long-term outcome; Overall survival; Disease-free survival; Prognosis; Score
INTRODUCTION
Colorectal cancer (CRC) is the third leading cause of cancer-related death in developed countries[1].About half of the cases will develop liver metastasis, and 25% of them will present synchronously[2].Hepatic resection has become the standard management in selected patients, with a reported 5-year survival rate ranging from 36% to 60% after curative liver resection[2-4].Yet, this is a heterogeneous group of patients with variable prognoses[2].As such, many studies have been directed towards the investigation of factors that might influence the recurrence and survival of patients with colorectal liver metastasis (CLM), with a goal to differentiate patients that would best benefit from surgical resection from those who should be directed to palliative care[5-8].The objectives of the present study were to identify the prognostic factors of survival in patients subjected to resection of CLM and to propose a risk score accordingly, to differentiate these patients.
MATERIALS AND METHODS
Data source and study population
Between June 1999 and June 2020, all resections of CLM in Kwong Wah Hospital were recorded prospectively in the institution’s database and retrospectively analyzed.Patients who underwent palliative resection or ablation treatment only were excluded from analysis.
All patients were followed according to a defined protocol including serum carcinoembryonic antigen level, chest X-ray, and computed tomography scan of the abdomen with contrast or ultrasonography of the liver if the patient was contraindicated for contrast injection.Patients were followed every 3 mo for the first 2 years after the operation and every 6 mo afterwards.Patients were actively called back for follow-up if they missed the appointment.
Patient demographics were extracted, including age at resection of liver metastasis and sex.Information on preoperative factors such as the site of the primary tumor, American Joint Committee on Cancer stage of primary tumor, primary tumor nodal stage, extrahepatic metastasis, disease-free interval from CRC resection to development of metastatic liver disease, carcinoembryonic antigen (CEA) level, and administration of systemic chemotherapy before liver resection was recorded.Regional lymph node metastasis of primary tumor was defined as mesenteric lymph node metastasis found histologically after resection of primary CRC.Synchronous metastases were defined as metastases detected by preoperative screening or during resection of the primary tumor or occurring within 6 mo of the initial diagnosis of CRC[9].
Data on operative details including the extent of liver resection (majorvsminor hepatectomy), concomitant use of ablation and operative approach (laparoscopicvsopen), volume of blood loss, and requirement of blood transfusion were collected; major hepatectomy was defined as a resection of at least three Couinaud liver segments.Perioperative outcomes, including 30-d mortality and complications, were reported.Pathologic details, including number of tumors, size of the largest tumor nodule, and resection margin, were extracted.Positive resection margin was defined as the presence of tumor cells within 1 mm of the transection line.
The primary endpoint was overall survival, which was defined as the time interval between primary surgical treatment of liver metastasis and the date of death or last follow-up.Secondary endpoint was disease-free survival, which was defined as the time interval between primary surgical treatment of liver metastasis and the date of radiological diagnosis of recurrence.
Statistical analysis
Continuous variables are summarized as the median with interquartile range (IQR) and categorical variables as frequencies with percentage.Overall and disease-free survival curves were plotted using Kaplan-Meier estimator.Variables affecting longterm survival were determined using the Cox proportional hazards regression model.In order to formulate a risk score, inclusion of variables into multivariable Cox models was based mainly on preoperative factors with clinical relevance, irrespective of thePvalue in the univariate analysis.This type of variable selection was appropriate because the bivariate selection method wrongly rejects potentially important variables when the relationship between an outcome and a risk factor is confounded by any confounder and when this confounder is not properly controlled[10].Data were calculated for hazard ratio (HR).Continuous variables were discretized into categorical variables by clinical relevance.A clinical risk score for overall survival was formulated according to factors identified by the multivariate analysis.Statistical significance was defined asPvalue of the Wald test < 0.05.All the statistical analyses were carried out using SPSS software version 26 (IBM Corp., Chicago, IL, United States).
RESULTS
All 98 patients who underwent resection of CLM during the study period were included in this analytic cohort.Median follow-up period was 36 mo (IQR: 17.00-57.75).There were no missing data or patients lost to follow-up.The clinicopathological data are summarized in Table 1.The study population included 62 males (63.3%) and 36 females (36.7%).The median age of patients at liver resection was 65.5 years (IQR: 59-72).The location of the primary colorectal tumor was mostly in the left colon (n= 40, 40.8%) and rectum (n= 32, 32.7%), and 26 patients (26.5%) had a primary right-sided colon cancer.Regional lymph node metastases were present in 62 patients (63.3%).Fifty-nine patients (60.2%) had synchronous hepatic metastasis.Sixteen patients (16.3%) underwent combined liver and colorectal resection, and eleven (68.8%) of them were performed laparoscopically.Only four patients (4.1%) had a synchronous extrahepatic disease; all of them were pulmonary metastases.Two of the pulmonary metastasis patients underwent curative pulmonary metastasectomy.One patient did not have surgery because he was subsequently diagnosed with a brain metastasis before pulmonary resection.
The median operative time was 270 min (IQR: 177.5-376.0).The median length of hospital stay was 7 d (IQR: 6-11).There was no 30-d postoperative mortality.Eight postoperative complications required interventional radiology.Bile leak (n= 4) was the most common cause, followed by intra-abdominal collection (n= 3), and there was one case of drainage of pleural effusion.There were three postoperative endoscopic retrograde cholangiopancreatographies, indicated for bile leakage, with a common bile duct stent inserted.There was one esophagogastroduodenoscopy performed for coffee-ground aspirate from the nasogastric tube, which only showed gastritis.There were three reoperations.One reoperation was due to adhesive intestinal obstruction and the other two because of intra-abdominal sepsis.
Factors affecting survival
The median overall survival of the entire cohort was 45 mo.The 1-, 3-, and 5-year overall survival rates were 93.6%, 65.8%, and 35.5%, respectively.The overall survival curve is shown in Figure 1A.The median disease-free survival was 19 mo.The 1-, 3-, and 5-year disease-free survival rates were 64.4%, 36.8%, and 27.4%, respectively.The disease-free survival curve is shown in Figure 1B.Univariate analyses of factors affecting overall survival and disease-free survival are shown in Tables 2 and 3,respectively.

Table 1 Clinicopathological data of patients
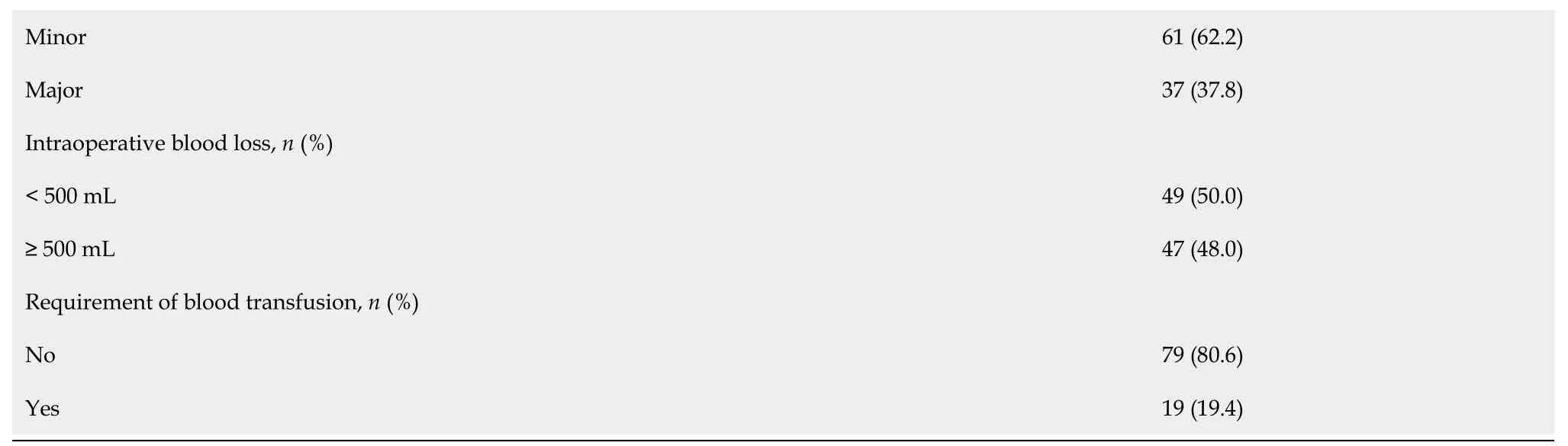
CEA: Carcinoembryonic antigen; IQR: Interquartile range; LN: Lymph node.
On multivariate analysis, the number of liver metastases ≥ 5 [HR: 2.962, 95% confidence interval (CI): 1.174-7.473,P= 0.022], the size of the largest liver lesion ≥ 4 cm (HR: 2.983, 95%CI: 1.343-6.625,P= 0.007), and the presence of nodal metastasis from the primary tumor (HR: 1.955, 95%CI: 1.031-3.707,P= 0.040) were associated with a worse overall survival (Table 4).On the other hand, the number of liver metastases ≥ 5 (HR: 2.753, 95%CI: 1.052-7.205,P= 0.039) and the presence of nodal metastasis (HR: 2.234, 95%CI: 1.219-4.093,P= 0.009) were associated with a worse disease-free survival on multivariate analysis (Table 5).

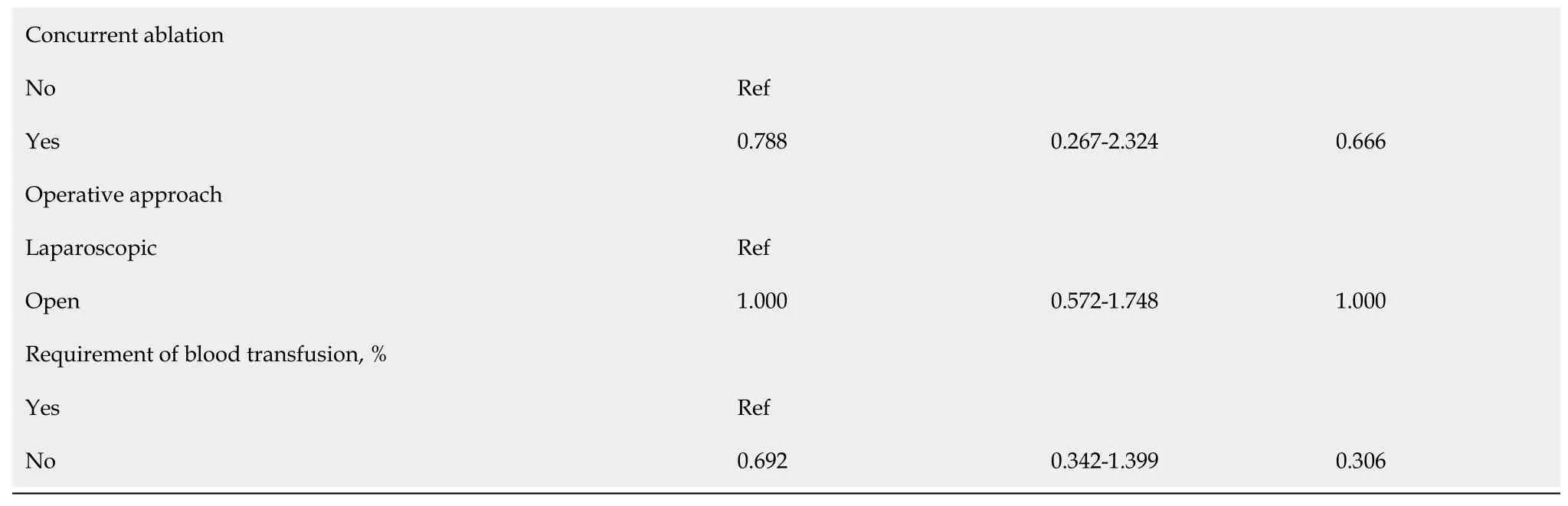
Table 2 Univariate analysis of factors associated with overall survival
Risk score
Three factors-the number of liver metastases ≥ 5, the size of the largest liver lesion ≥ 4 cm, and the presence of nodal metastasis from the primary tumor-were chosen as criteria for a clinical risk score for overall survival.As the HRs of these three factors were similar, for the sake of simplicity, each criterion was assigned 1 point.The total score was compared with overall survival using the log-rank test (Figure 1C).Although the survival of patients with score 0 (5-year survival: 46.8%, median survival of 50 mo) and score 1 was similar (5-year survival: 49.7%, median survival of 49 mo), overall survival clearly separated from those with score 2 (5-year survival: 10.8%, median survival of 33 mo) and score 3 (no 5-year survivors, median survival of 17 mo,P= 0.002).
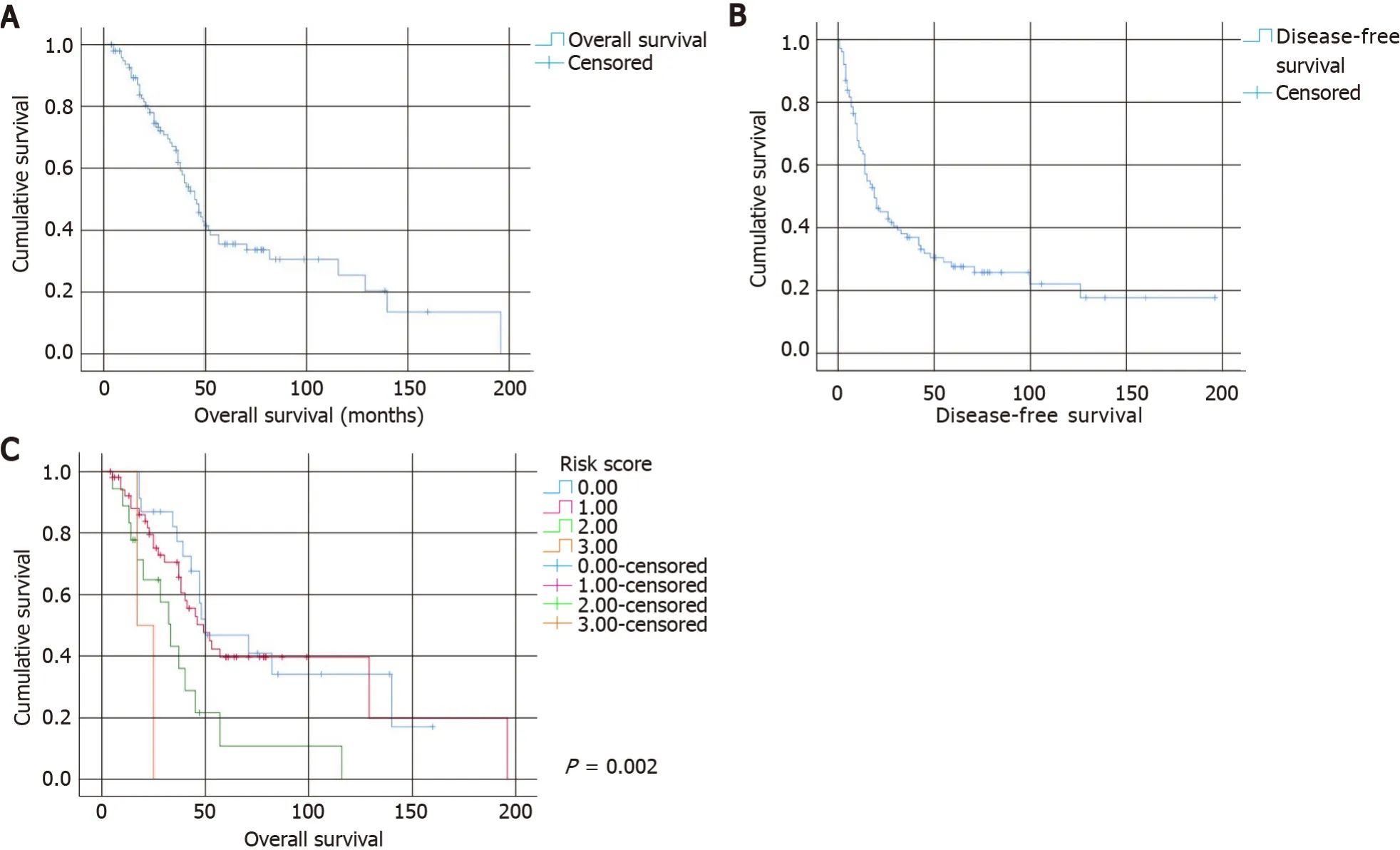
Figure 1 Kaplan-Meier curves.
DISCUSSION
The management of CLM has seen a marked change over the last decade, owing to the advancement of surgical techniques and perioperative treatments[3].The achievement of curative resection of liver metastasis has transformed the 5-year survival from 11% to a range of 36%-60%[2-4].The current study demonstrated a 5-year overall survival rate of 35.5%, slightly lower than the reported survival rate.This is probably due to the extended duration of the study period, which could be traced back to as early as 1999, in which management of CLM was less aggressive.
Many studies have investigated the prognostic factors of survival after resection of CLM.The most frequently cited prognostic factors are the number and the largest size of CLM, regional lymph node metastasis of the primary tumor, and preoperative CEA level[2].Other proposed factors included disease-free interval from the treatment of primary CRC, location of primary CRC, and surgical resection margin[4,11,12].The present study confirmed that a larger number of liver metastases, a larger size of the liver tumor, and the presence of regional lymph node metastasis of the primary tumor were associated with a poorer long-term survival.Among them, the number of liver lesions and the size of the largest liver tumor had the highest HRs (2.962 and 2.983, respectively).
Our study also identified that the largest tumor size 4 cm was the optimal cutoff value for prognostic purposes.Fonget al[5] and Nordlingeret al[6] were among the earliest groups of investigators to produce a clinical risk score, which utilized the size of the largest tumor > 5 cm as one of the criteria.This cutoff value has been used in subsequent studies as well[13,14].Yet, this cutoff value was not universal; other size parameters (i.e., 2 cm, 3 cm, or 4 cm) have been adopted as well[4,15,16].Hence, size parameter of liver metastasis is a generally accepted risk factor, and our study isconsistent with previous studies.

aP < 0.05.CEA: Carcinoembryonic antigen; CI: Confidence interval; HR: Hazard ratio; LN: Lymph node; Ref: Reference.
The current study evaluated that number of liver metastases 5 was the cutoff value that predicted a negative survival.The number of liver metastases is another frequently reported prognostic factor[2,5,6,13,14,16-18].Again, there was not a universally accepted cutoff value for the number of liver metastases.However, a Japanese group of researchers analyzed 727 patients who had undergone CLM resections and reported that 4-5 was the most reliable cutoff value (HR: 2.35)[19].Some studies also demonstrated that solitary liver metastasis had a significantly better prognosis than multiple metastases[16,18,20].The present study echoed the past studies and was able to demonstrate the prognostic significance of the number of liver metastases.
Our study failed to show that the preoperative CEA level had a significant impact on long-term survival.Half of the published data referred to preoperative CEA level as a poor prognostic factor[2].One of the possible explanations is that the sample size of the current study was too small to detect a significant result for this factor.
Concerning the surgical approach, past studies suggested that laparoscopic surgery was a favorable alternative to open surgery in selected CLM patients[21,22].The OSLO-COMET randomized controlled trial, which compared laparoscopic and open parenchyma-sparing liver resection for CLM, concluded that laparoscopic surgery was associated with significantly less postoperative complications[23,24].Although the evidence of the benefit of laparoscopic surgery on long-term survival is limited, there was a meta-analysis published in 2020 that aimed to evaluate the long-term oncologic outcome of laparoscopic and open liver surgery for CLM patients[25].The study included 13 propensity-score matched studies and two randomized controlled trials, with a total of 3148 patients.The study concluded that laparoscopic surgery had a restricted mean survival time 8.6 mo longer at 10 years (P< 0.0001) and 30.0 mo longer at 15 years (P< 0.0001) than the open surgery group.The current study concurred with previous findings of similar survival between laparoscopic and open liver resections.Further research on this subject using a case-matched cohort study would be helpful.
Elderly patients are bound to have less physiological reserve and suffer from more medical comorbidity than younger patients.These factors will cause older patients to be more prone to surgical risks and mortality from other non-cancer related causes.Yet, from our study, liver surgery in elderly patients appeared to be safe, with a comparable outcome to younger patients, and these patients should not be denied surgery due to the sole reason of advanced age[26,27].As a result of this argument, age should not be used as a criterion in formulating management of CLM.
The first large-scale clinical scoring system was the Nordlinger score, which incorporated preoperative and postoperative factors[6].Then, Fonget al[5] developed a frequently cited clinical score system in 1999.Recently, the Tumor Burden Score was developed based on the concept of the “Metro-Ticket” paradigm and utilized a continuum of liver tumor size and number.This score was developed and validated in studies where most patients received modern neoadjuvant chemotherapy[7].It is a growing recognition that KRAS and BRAF mutation statuses are important prognostic biochemical markers[28].Brudviket al[8] and Beamishet al[29] created a clinical scoring system specifically examining the impact of KRAS mutational status on survival of CLM patients.Many studies had been conducted to validate these clinical prediction scores[30-32].A recent study examined the validity of previous clinical risk scoring systems in the contemporary era where chemotherapeutic treatment for CLM patients had significant improvement.It was shown that previous systems were still relevant in modern clinical use[29].
Despite the emergence of numerous clinical scoring systems in keeping with the development of oncological treatment for CLM, the most frequently cited scoring system was still the Fong score due to its incorporation of clinical criteria available for all patients (size, number, nodal status, preoperative CEA level, and disease-freeinterval)[5].This was also applicable to our clinical scoring system, which was basically a simplified version of the Fong score.Apart from its simplicity, the factors of the current scoring system are easily available and are available before resection of the liver tumor (except in cases of synchronous resection).This is of vital importance when clinicians are formulating the cancer-specific treatment for patients.The distinct difference in overall survival between the higher and lower score groups means that we can identify two groups of patients who are the most and the least likely to benefit from surgical treatment.A more reserved attitude should be given to the group of patients with the highest score (score = 3), in which there were no 5-year survivors, and the median survival was 17 mo, which was similar to patients without liver resection (15.5-21.3 mo)[33,34].With the advancement in chemotherapeutic and radiological treatment, this group of patients may achieve a comparable life expectancy without the need to sustain surgical risks and discomforts.The lowest score groups (score = 0 or 1) are clearly the group of patients that can enjoy the benefit of extension of overall survival as a result of surgical treatment.Grey area existed for the average score (score = 2) group.In this group, additional factors, such as patient premorbid status, should be taken into consideration (Table 6).

Table 3 Univariate analysis of factors associated with disease-free survival

Table 4 Multivariate analysis of factors associated with overall survival

Table 5 Multivariate analysis of factors associated with disease-free survival

Table 6 Risk score

aP < 0.05.CEA: Carcinoembryonic antigen; CI: Confidence interval; HR: Hazard ratio; LN: Lymph node; Ref: Reference.

aP < 0.05.CEA: Carcinoembryonic antigen; CI: Confidence interval; HR: Hazard ratio; LN: Lymph node; Ref: Reference.
aP < 0.05.CEA: Carcinoembryonic antigen; CI: Confidence interval; HR: Hazard ratio; LN: Lymph node; Ref: Reference.
Several limitations should be considered when interpreting the results of the current study.The retrospective design may limit its conclusions on associations over time.Second, it is a single-center study involving only a small study population with data recorded over 21 years.Perioperative management, including chemotherapy, changes over time, and consequently survival, may be influenced.
CONCLUSION
Nodal metastasis from the primary tumor, number of liver metastasis, and size of the largest liver tumor have a significant negative impact on overall survival of the patient after resection of CLM.In clinical practice, laparoscopic surgery should be an available option for a selected group of patients due to its potential benefits.When formulating cancer-specific treatment for patients with CLM, we proposed using a simplified clinical scoring system consisting of three significant prognostic factors.Priority over surgical resection should be given to the lowest score groups, and alternative oncological treatment should be considered in the group of patients with the highest score.
ARTICLE HIGHLIGHTS
Research background
Colorectal cancer is the third leading cause of cancer-related death in developed countries.About half of the cases will develop liver metastasis.Hepatic resection has become the standard management in selected patients, with a reported 5-year survival rate ranging from 36% to 60% after curative liver resection.
Research motivation
Patients with colorectal liver metastasis (CLM) are a heterogeneous group, with variable prognoses even after liver resection.As such, many studies have investigated factors that might influence the recurrence and survival of this group of patients, with a hope to differentiate patients that would best benefit from surgical resection from those who should be directed to palliative care.
Research objectives
The objectives of the present study were to identify the prognostic factors of survival in patients subjected to resection of CLM and to propose a risk score accordingly, to differentiate these patients.
Research methods
Between June 1999 and June 2020, all resections of CLM at Kwong Wah Hospital were recorded prospectively in the institution’s database and retrospectively analyzed.Variables affecting long-term survival were determined using the Cox proportional hazards regression model.A clinical risk score for overall survival was formulated according to factors identified by multivariate analysis.
Research results
On multivariate analysis, the number of liver metastases ≥ 5 [hazard ratio (HR): 2.962, 95% confidence interval (CI): 1.174-7.473, P = 0.022], the size of the largest liver lesion ≥ 4 cm (HR: 2.983, 95%CI: 1.343-6.625, P = 0.007), and the presence of nodal metastasis from the primary tumor (HR: 1.955, 95%CI: 1.031-3.707,P= 0.040) were associated with a worse overall survival.These three factors were chosen as criteria for a clinical risk score for overall survival, and the total risk score was compared with overall survival using the log-rank test.Lower total risk score groups had a significantly improved overall survival than the higher total risk score group.
Research conclusions
The newly proposed clinical risk score consisting of three significant prognostic factors (nodal metastasis from the primary tumor, number of liver metastases, and size of the largest liver tumor) is simple and easy to use.Priority over surgical resection should be given to the lowest score groups, and alternative oncological treatment should be considered in the group of patients with the highest score.
Research perspectives
Small study population (98 patients) and retrospective design limit the conclusions on associations over time.Future study with an expanded study population may allow weighting assignment to each component of the clinical risk score for a more accuracy in prognosis prediction.An external validation study is needed for the actual application of this clinical score in clinical use.
杂志排行

World Journal of Hepatology的其它文章
- Hepatitis C virus: A critical approach to who really needs treatment
- Current aspects of renal dysfunction after liver transplantation
- Hepatitis C: Problems to extinction and residual hepatic and extrahepatic lesions after sustained virological response
- Metabolic and nutritional triggers associated with increased risk of liver complications in SARS-CoV-2
- Recent updates on progressive familial intrahepatic cholestasis types 1, 2 and 3: Outcome and therapeutic strategies
- Targets of immunotherapy for hepatocellular carcinoma: An update