Effect of health locus of control on the quality of life among hemodialysis patients
2021-06-25MahdiMOSHKIJahanshirTAVAKOLIZADEHMohammadVahedianSHAHROODIMahmoudNABIANSANIAtefehDEHNOALIANDepartmentofHealthEducationandHealthPromotionSchoolofHealthSciencesandSocialDeterminantsofHealthResearchCenterDepartmentofPsychiatryS
Mahdi MOSHKI, Jahanshir TAVAKOLIZADEH,Mohammad Vahedian SHAHROODI, Mahmoud NABIANSANI, Atefeh DEHNOALIANDepartment of Health Education and Health Promotion, School of Health Sciences and Social Determinants of Health Research Center; Department of Psychiatry, School of Medicine,Gonabad University of Medical Sciences, Gonabad, Iran; Social Determinants of Health Research Center, Department of Health Education and Health Promotion, School of Health; Clinical Supervisor of Ghaem Hospital, Mashhad University of Medical Sciences, Mashhad, Iran; Department of Nursing, Neyshabur University of Medical Sciences, Neyshabur, Iran
ABSTRACT
Objective: The purpose of this study was to determine the effect of health locus of control on the quality of life on hemodialysis patients.
Materials and Methods: This study is a randomized controlled trial. Participants were 78 dialysis patients among 17–70 years old including 39 cases in the training program and 39 cases in control groups. Kidney disease quality of life-short form and the health locus of control scale-form A were used. Questionnaires were completed before and 8 weeks after the intervention by two groups.
Results: The results of the paired t-test showed that the mean scores of physical component summary, mental component summary, and components of renal disease in the test group increased significantly after the intervention. There was also a significant difference between the test and control groups only about powerful others.
Conclusion: The education based on health locus of control can have a positive effect on the life quality of hemodialysis patients.
Keywords: Hemodialysis, locus of control, quality of life, randomized controlled trial
INTRODUCTION
Chronic kidney disease (CKD) is one of the major public health problems worldwide.[1]It is a progressive and irreversible disorder that eventually leads to uremia.[2]CKD endangers not only physical health but also other aspects of health.[1]Published statistics from the United States National Center for Kidney Disease show that approximately 15% of the population suffers from chronic renal failure,[3]of which 65% are on hemodialysis. A number which is increasing at an alarming percent of approximately 8%–10% annually.[4]According to a systematic review and meta-analysis, the prevalence of renal failure in Iran is 15.14%, and the prevalence of CKD in female patients (18.80%) is 1.7 times higher than male patients (10.83%).[5]These patients, in the absence of a successful kidney transplant, will survive premature death using new therapies like hemodialysis.[6,7]However, they may suffer from cardiovascular, skeletal, endocrine, inflammatory,neoplastic diseases[8]and psychological complications.[9]Recent studies have demonstrated a relationship between psychosocial variables, quality of life, and mortality in renal replacement therapy patients leading to poor adherence to dialysis.[10]
In today’s world, improving the quality of life is of particular importance. The quality of life is the distance between the expectations and the experiences of individuals.Typically, even patients with the same clinical condition report different quality of life. Hence, evaluating patients’quality of life helps the care provider to understand the way patients perceive their health, functional ability, and sense of well-being and to consider the ways to improve the quality of life in patients.[6,7]
It has been discovered that patients’ health can be controlled by beliefs and convictions.[11]Health locus of control consists of personal beliefs based on past experiences in health issues and having external or internal power over them in a way that could affect health.[12,13]Rotter introduces two key aspects of internal and external control.[14]In the external control, a person believes life events depend on the external factors or other powers, while in the internal control, the person thinks life events are under his/her control, and he/she is responsible for them.[15]Put differently, the health belief model focuses on the issue that, generally, people have good reactions to health messages and disease prevention strategies when they feel they are at serious risk (perceived threat); it is just then they perceive the benefit of changing their behavior (perceived benefits), and start to eliminate the barriers to these changes (new and healthy preventive behavior), and become confident whether to adopt a new behavior (perceived self-efficacy). It is in these situations that educational interventions and programs are likely to be effective.[16,17]
Despite much research dealing with the quality of life in dialysis patients, such studies are still few. Our educational program is designed to increase the awareness of patients regarding their health issues as well as to minimize the unfavorable effects on their overall quality of life. Therefore,this study was conducted to investigate the application of health locus of control in the quality of life in hemodialysis patients.
MATERIALS AND METHODS
Design
This was a randomized controlled trial.
Participants
This study was conducted in 2017 among 17–70 years old dialysis patients. The patients were selected by the random stratified sampling method. Then, the participants were allocated randomly in the test and control groups,respectively (using the flip the coin method). The sample size was determined based on a previous study[18]and using Altman’s nomogram which possibility of sample fall was estimated at 78 people.
First, the statistics of hemodialysis patients were collected separately by the treatment center, and then the desired number in each hospital was estimated according to the ratio of the patient’s population to the total study population. Because patients were on hemodialysis three times a week (once a day)in each treatment center, patients on even days of the week were selected as the control group and patients on odd days of the week were selected as the test group.
The whole process of randomization and registration of participants was done by researchers.
The inclusion criteria were as follows: having a medical report in the hemodialysis ward, being at the age range of 17–70 years, receiving hemodialysis for at least 6 months,performing hemodialysis at least 2 times a week for 3 h,being willing to participate in the study, not having any visual or hearing deficits, no mental illness, and other diseases affecting the quality of life. The exclusion criteria were as follows: not willing to participate or continue the study,incomplete answers to questions in the questionnaires, and having renal transplantation surgery [Figure 1].
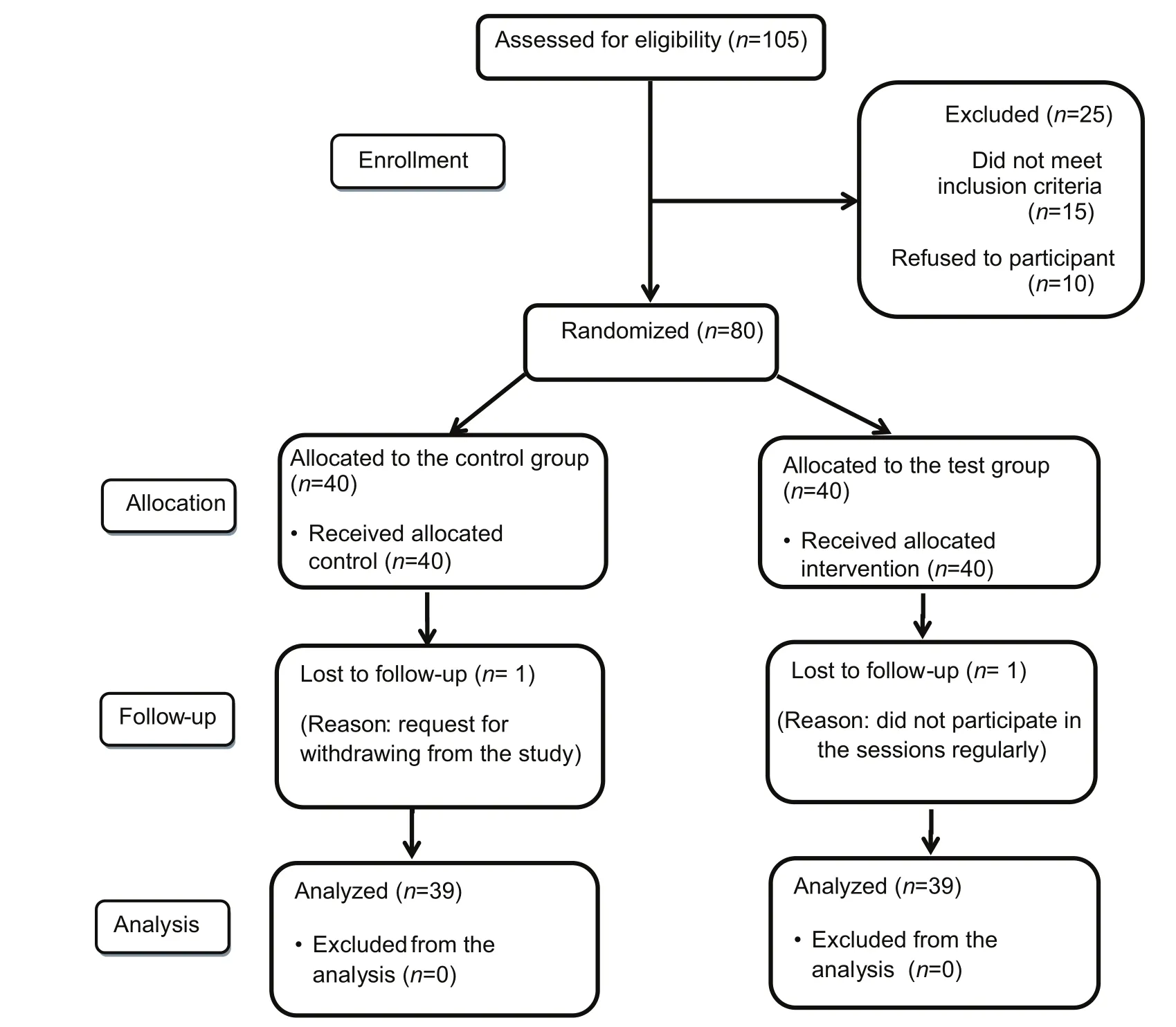
Figure 1: Flow of participants through each stage of this study
Intervention Before intervention
In this section, after selecting the participants, the research questionnaires were distributed among the research units and were collected after completion. By analyzing data at this stage, the most influential constructs on the quality of life were determined before intervention in the research community. Based on these data, a needs assessment was conducted, and the educational content was designed.
Intervention
In this section, participants in the test group were divided into four subgroups of eight and one subgroup of seven.Then, participants were organized a training program based on the needs assessment in the previous stage. The main researcher conducted three 40-min face-to-face sessions for 3 weeks in the test group in the dialysis department.
The sessions were as follows
First session: Patients attended a session aimed at raising awareness about kidney disease. The educational content of this session included a definition of kidney disease,hemodialysis and its complications, and ways to reduce these complications. All of these topics were explained in general,and then they were discussed in more detail.
Second session: This session was held to develop a proper attitude about the quality of life, factors affecting the quality of life and the ways to improve it, and the effective role of nutrition and physical activity in preventing complications. At this meeting, was provided information about patients’ numbers and statistics and also cultural,sports, and economic achievements, and honors of dialysis patients at national and international levels were discussed.
The third session: In this session, was conducted a detailed discussion to raise the awareness of patients about self-care and ways to improve it and its impact on the quality of life.Then, daily text messages were sent for 1 month after the sessions were completed.
It should be noted that the control group received routine care (just a pamphlet about hemodialysis) without any face-to-face educational intervention.
After intervention
Eight weeks after the completion of the training program,the same questionnaires were distributed and completed in both groups (test and control).
Measures Demographic questionnaire
The first part of the questionnaire included seven demographic questions about age, sex, level of education, occupation,hemodialysis duration, household income level, and smoking.
Kidney disease quality of life short-form questionnaire(version 1.3)
This questionnaire is a specific tool for assessing the quality of life in hemodialysis patients. The general part of the questionnaire consists of 36 questions in three sections: (1)physical component summary (PCS) (includes four areas of general health, physical functioning, pain, and limitations caused by physical problems); (2) mental component summary (MCS) (includes four areas of social functioning,emotional functioning, emotional well-being, and fatigue/energy); and (3) the section related to the quality of life in kidney disease has 11 dimensions, including symptoms,problems, the impact of renal disease on the daily living,the burden of the kidney disease, occupational status,cognitive functioning, the quality of social interaction, sexual functioning, sleep, social support, health-care staff support,and patient satisfaction. Each question is scored from 0 to 100.
This questionnaire has already been used in various studies with its validity and reliability evaluated and verified.[19-21]
Multidimensional health locus of control scale-form A
It used the multidimensional health locus of control scale-form A (MHLC-form A) to measure health beliefs. Wallstonetal.designed this scale in 1978 to determine patients’ beliefs about health. MHLC-form C includes three subscales titled as internal locus of control (Internal Health Locus of Control [IHLC]),external health locus of control of others (Powerful Other Health Locus of Control [PHLC]), and health locus of control of outside chance (Chance Health Locus of Control [CHLC]). IHLC determines the degree to which a person believes internal factors and behaviors account for the health. PHLC examines the degree to which a person believes health is determined by other people, and CHLC assesses the degree to which a person believes health depends on chance, luck, fortune, or fate. It is a 6-point Likert scale (1 = disagreed, 6 = very much agreed). The total score is the sum score of the items in each subgroup. None of the items needs reversing before adding up. All the subgroups are independent of each other. In MHLC,no specific score is known as the cutoff point, and the mean and median are used to measure the Z-Score. The reliability and validity of the Persian version of the questionnaire were confirmed by Moshkietal.[22]
Ethical considerations
It should be emphasized that all participants were briefed about the study and its objectives and willingly signed written informed consent forms before participating in the study. They were ensured about the confidentiality of their information and the questionnaires were filled out anonymously. Moreover,they were free to quit whenever they wished to do so.
Data analysis
Data were analyzed by SPSS 16.0 (SPSS Inc., Chicago, IL) using descriptive (mean, frequency, and relative frequency) as well as analytical statistical tests (t-test, Chi-square, Pearson correlation coefficient, and pairedt-test). The significance level was considered to be <0.05.
RESULTS
A total of 78 hemodialysis patients (n= 39 in each group) in the age range of 17–70 years were evaluated. Fifty-seven persons were male and 21 were female. The mean age of the patients in the test and control groups was 45.72 ± 15.15 and 45.28 ± 13.98 years,respectively. About 84.6% reported <100 months of disease duration. Other demographic factors are presented in Table 1.
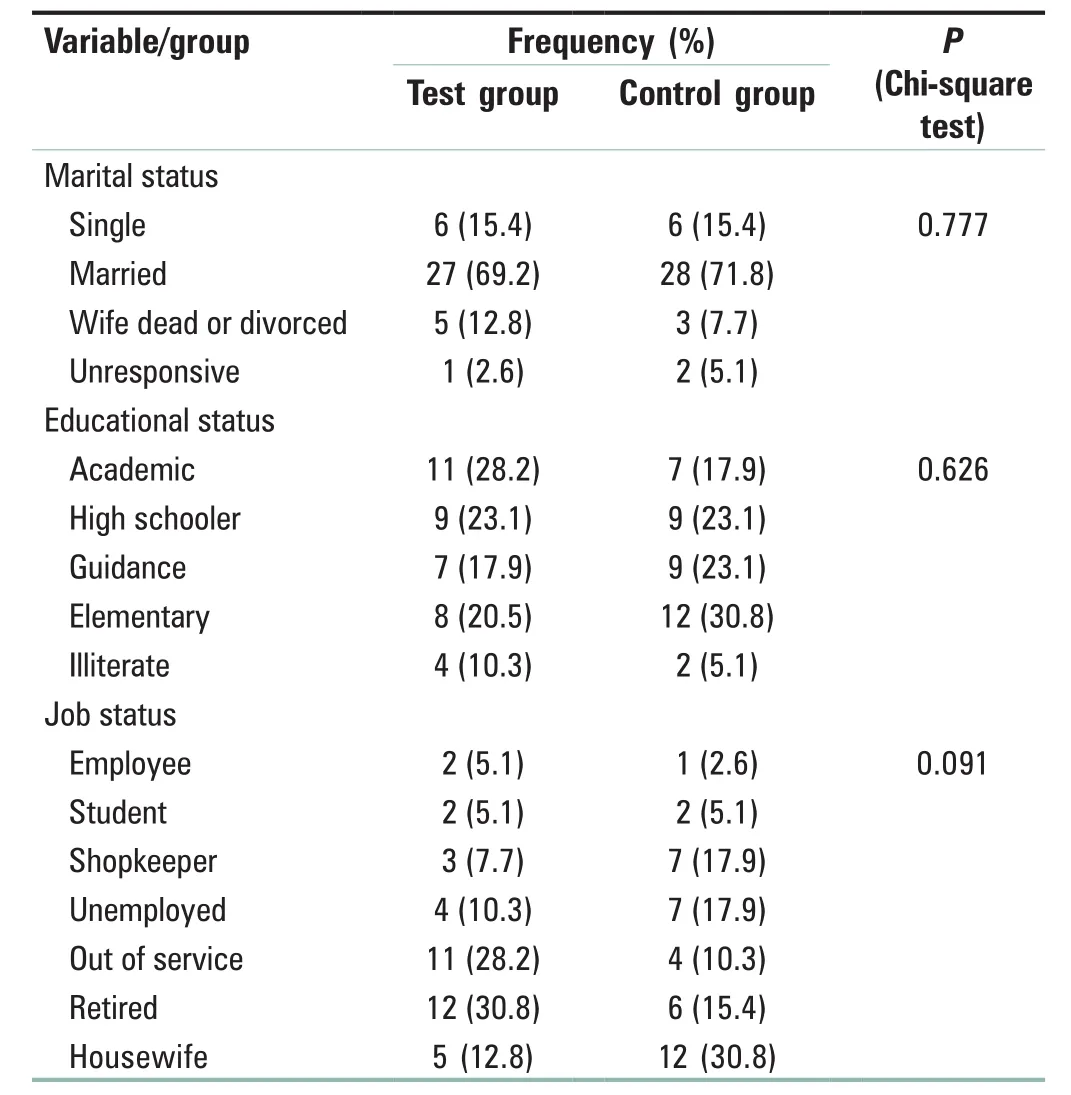
Table 1: Demographic factors in participants (n=78)
The results of the pairedt-test showed that the mean scores of PCS, MCS, and components of renal disease in the test group increased significantly after the intervention (P< 0.05) [Table 2].

Table 2: The mean scores comparison of the quality of life constructs and the total score in both test and control groups before and after the intervention
The results showed a significant difference between the test and control groups only about powerful others (P< 0.001),and no significant change was noted in terms of other preventive behaviors [Table 3].

Table 3: The mean comparison of health locus of control components in both groups before and after the intervention
The Pearson correlation coefficient indicated that, after the intervention, the dimensions of the role limitation induced by the emotional problems, emotional well-being, burden of disease, symptoms, problems, social support, and health-care staff support were directly related to the internal factors;however, the burden of the disease and cognitive functioning showed an inverse relation with the chance [Table 4].
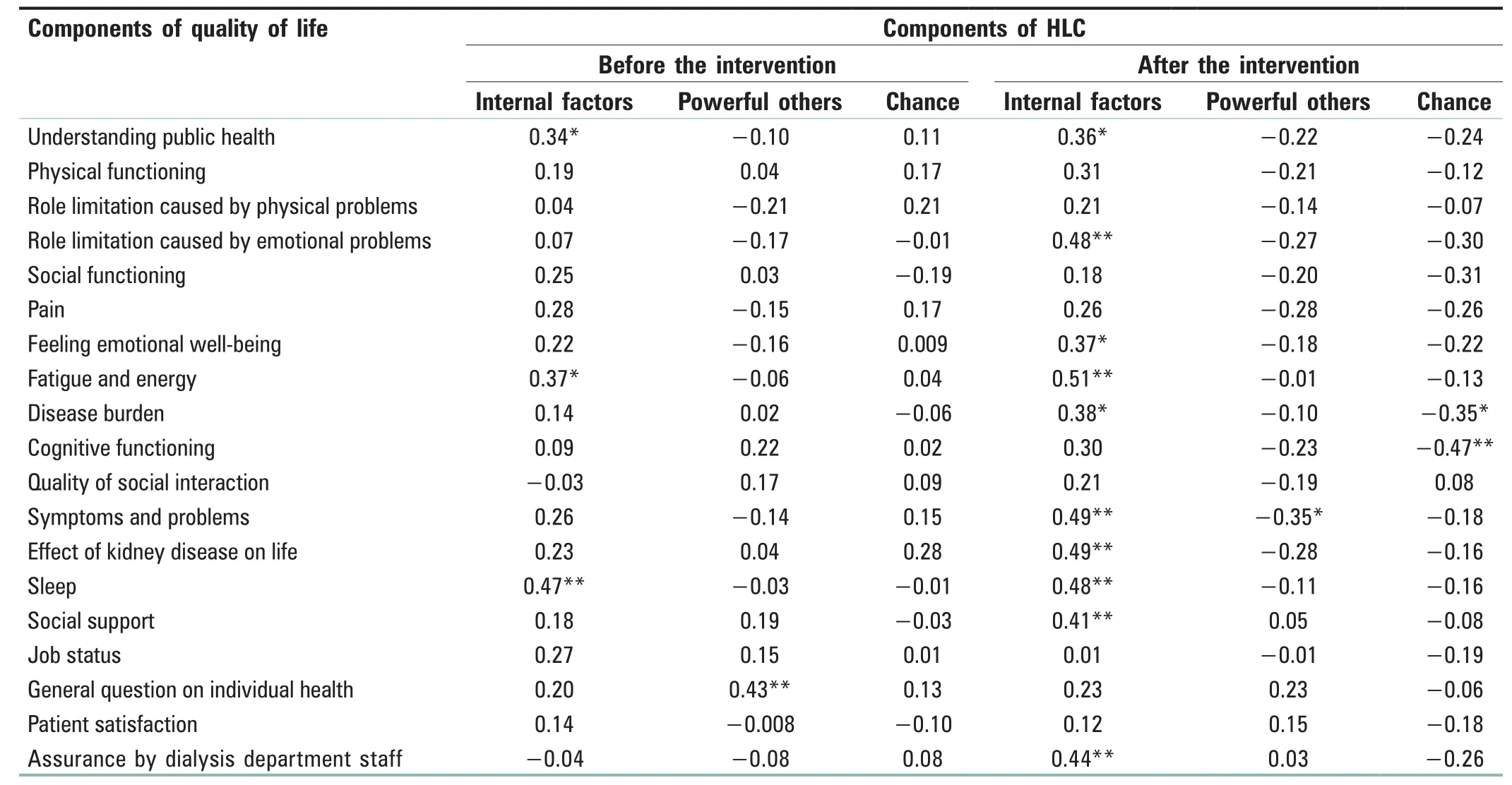
Table 4: The relationship between components of health locus of control and quality of life dimensions in the test group before and after the intervention
DISCUSSION
The results showed that health locus of control can significantly improve the quality of life in hemodialysis patients. In the present study, after the intervention, the mean score of the overall quality of life in the test group improved from 60.24 to 69.37, which keeps the patients in a good quality of life. By comparing the mean scores of these components, it was found that the highest effect of training on the physical component was 15 points higher than the average, and then the mean kidney disease component summary scores created with 8 points increased. These results are consistent with the studies performed by Mustataetal.,[23]Moghimi Dehkordietal.,[24]Nonoyamaetal.,[25]Ghadamet al.,[26]and Bakarmanetal.[4]
Parsons concluded that exercise training did not play a role in improving the quality of life among hemodialysis patients.[27]Perhaps, the reason for this difference is that patients in the Parsons study had a 4-month dialysis experience, which may have had a significant effect on the outcome. Barzegaretal.in their study entitled as Relationship Between Duration of Dialysis and Quality of Life in Hemodialysis Patients found that the mean quality of life in patients on hemodialysis for >3 years was somewhat lower than the patients with longer duration of dialysis therapy; however, this relation was not significant.[28]According to Gerasimoulaetal., the elapsed time from hemodialysis could reduce the patients’quality of life.[29]
In this study, the comparison of the mean components of the health locus of control (internal factors, powerful others, and chance scores) showed a significant difference before and after the intervention in the test group only in the dimension of powerful others. However, there were no significant differences in terms of other components in both groups before and after the intervention. In other words,education influenced powerful others, significantly reduced the degree of individuals’ beliefs about the effect of others on their health or illness, and highlighted the role of internal factors. However, incorrect chance-associated beliefs should not be underestimated. The present study revealed that after educating patients, they related their health status mostly to their actions and behaviors and not to chance. Normanetal. showed that the higher the score of the internal health locus of control, the more health-related behaviors such as exercise and dietary compliance are likely to occur; on the other hand, if the chance locus of control and powerful others get higher scores, the incidence of health behaviors would be lower.[30]Hatamlooetal. held that people with an internal health locus of control believe that they have control over their health; therefore, they will enhance their health behaviors and show a greater tendency toward having good eating habits and doing medical examinations.[31]Therefore,the internal health locus of control directly affects the quality of life of hemodialysis patients, and education can increase the awareness of these individuals about health determinants,empower them, and create positive health beliefs in them to strengthen their internal health locus of control and promote their health behaviors.
Besides, after the intervention, the study participants believed that their quality of life in most aspects is dependent on internal factors, such that the behaviors and ways of dealing with a person are responsible for improving the quality of life. This finding is inconsistent with Rutter’s view stating that externally focused people are more likely to suffer mental disorders.[32]However, it is in line with the results by Wallston who believed that the axis of health control is the degree to which a person believes that his/her health is influenced by internal or external factors.[12]
The results of this study provide a better understanding of the dimensions of the health control center in hemodialysis patients and it seems that medical staff should be aware of the role of this psychological phenomenon in creating self-control and self-management of patients and in order to increase the internal source of health control and more responsibility, they should take interventions.
The limitations of the study are the reluctance to participate in the study due to illness and lethargy, inaccuracy in completing the questionnaire due to a large number of questions, and the loss of patients during follow-up. To facilitate accountability and increase confidence replies,shorter tools for measuring the quality of life and health locus of control in renal patients should be developed. It is also recommended that future studies are conducted with a larger sample size so that the impact of the intervention on other dimensions of the health locus of control can also be considered.
CONCLUSION
The results of the present study indicate that the application of the health locus of control can lead to the adoption of self-care behaviors in hemodialysis patients and improve their quality of life through exerting a positive impact on internal health locus of control of patients and adjusting the effects of powerful others and chance locus of control. Therefore, it is suggested to design and implement educational programs based on health locus of control to improve the quality of life among hemodialysis patients.
Financial support and sponsorship
Nil.
Con flicts of interest
There are no conflicts of interest.
杂志排行

Journal of Integrative Nursing的其它文章
- The impacts of resilience on the association between illness uncertainty and sleep quality among patients with type 2 diabetes mellitus
- Scienti fic publications in nursing journals from East Asia:A survey of literature
- Mediating effect of undergraduate nursing students’professional commitment on positive psychological capital and learning burnout
- Correlation between psychological factors and the expression of galanin and 5-hydroxytryptamine in different subtypes of gastroesophageal re flux disease
- A nursing study on five-animal frolics in improving anxiety and depression of inpatients
- Teaching traditional Chinese medicine classics to clinical nurses: Taking Treatise on Cold Damage for example