Laparoscopic surgery for gastric cancer:Current status and future direction
2021-05-19SoHyunKangHyungHoKim
So Hyun Kang,Hyung-Ho Kim,2
1Department of Surgery,Seoul National University Bundang Hospital,Seongnam 13620,Republic of Korea;2 Department of Surgery,Seoul National University College of Medicine,Seoul 03080,Republic of Korea
Abstract Gastric cancer is still a major cause of death worldwide.While laparoscopic gastrectomy (LG) has gained evidence as a standard treatment for early gastric cancer in the distal stomach,there are still concerns regarding its application for gastric cancer in the upper stomach and advanced gastric cancer.Nevertheless,LG has shown to have faster recovery,shorter hospital stay,less pain,and less blood loss in many retrospective and prospective studies.The application of LG has now extended from conventional radical gastrectomy to novel approaches such as function-preserving gastrectomy and sentinel-node navigated surgery.Studies on the use of laparoscopy in treatment for stage IV gastric cancer are rare,but show that there may be some roles of LG in selected cases.With the development of new laparoscopic tools that augment human ability,the future of LG should move on from proving non-inferiority to demonstrating superiority compared to the traditional open gastrectomy.
Keywords:Laparoscopy;stomach neoplasm;minimally invasive surgical procedures
Introduction
Despite the declining incidence over the decade,gastric cancer is still the fifth most commonly diagnosed malignancy and the third leading cause of cancer death worldwide (1,2).Although Korea has the highest incidence of gastric cancer in both men and women (2),early gastric cancer (EGC) takes up to 61% (3) of gastric cancer diagnosed in the country.This high proportion of EGC in Korea is mostly attributed to the active implementation of the national screening program,often performed using endoscopy (4).According to the Korean national survey of gastric cancer in 2014,EGC is reported to have a favorable 5-year survival of nearly 95% (5).
Since the introduction of laparoscopic gastrectomy (LG)for gastric cancer by Kitanoet al(6),it has spread worldwide.Many efforts have been made to standardize the technique and prove its safety.Several randomized control trials (RCTs),starting from East Asia,have been released to analyze both the advantages and oncological safety of LG for different types of gastric cancer.For EGC of the distal stomach,laparoscopic distal gastrectomy has become the standard treatment in many gastric cancer guidelines(7-9).For advanced gastric cancer (AGC),some of the major RCTs have recently been published.This review will summarize the evidences surrounding LG for gastric cancer treatment,focusing on its application in functionpreserving gastrectomy,recent evidences in AGC,possible applications on stage IV gastric cancer,and technological advancements for reduced ports surgery.
Laparoscopic distal gastrectomy (LDG) for EGC
For EGC in the distal 2/3rd of the stomach,the benefits and safety of LDG or laparoscopic-assisted distal gastrectomy (LADG) are well established through various studies,including RCTs.Pivotal studies include the largescale multicenter RCTs held in Japan (JCOG0912) (10,11)and Korea (KLASS-01) (12,13).The KLASS-01 trial is(13),by far,the largest phase III RCT comparing open gastrectomy with LG,with 1,416 patients enrolled from 13 institutions from 15 surgeons,each performing more than 80 gastrectomies per year.This is the first study among many multicenter trials that have been conducted by the Korean Laparoendoscopic Gastrointestinal Surgery Study(KLASS) Group which are arranged inTable 1(12-16).The primary endpoint was 5-year overall survival (OS) with a noninferiority margin of -5% [corresponding hazard ratio (HR) of 1.54].It was published in 2019,showing 5-year OS rates of 94.2% in the laparoscopic group and 93.3% in the open surgery group [log-rank P=0.64,onesided 97.5% confidence interval (97.5% CI),-1.6].In the JCOG0912 trial,920 patients were enrolled from 33 institutions from March 2010 to November 2013.The primary endpoint was relapse-free survival (RFS) after a follow-up of 5 years,and the results were published in 2020(11) with LADG group also fulfilling the noninferiority criteria compared to the open distal gastrectomy (ODG)group (HR=0.84,90% CI,0.56-1.27;P=0.0075).Both trials were designed as non-inferiority trials,and their results were consistent with each other.There is a lack of well-designed large-scale studies for LDG in EGC from Western countries,which is unsurprising due to the rare incidence of EGC compared to East Asia.
Although the oncological safety of LG for distal EGC has been established rather recently,LDG displayed superior outcomes in short-term morbidity compared to ODG in various RCTs and systematic reviews.Laparoscopic surgery is known to have less blood loss,less postoperative pain,and faster patient recovery compared to open surgery (17).LADG is also known to have lower systematic inflammatory response compared to ODG (18).In the short-term analysis of the KLASS-01 trial (12),complication rate was lower in the LADG group (13.0%vs.19.9%,P=0.001),especially in wound complications.In the LADG group,the operative time was about 40 min longer(184.7±55.0vs.145.8±49.4 min),but had 75 mL less blood loss and shorter in hospital stay of about one day.Nowadays,the paradigm of LDG is moving from LADG to totally laparoscopic distal gastrectomy (TLDG) (19),in which all transection and anastomoses are being performed intracorporeally.A systematic review comparing TLDG and ODG analyzed 14 studies with a sample size of 1,532 patients (20).TLDG showed similar outcomes with longer operation time,less blood loss,shorter hospital stay,and fewer complications without significant difference in the number of harvested lymph nodes and surgical margins.
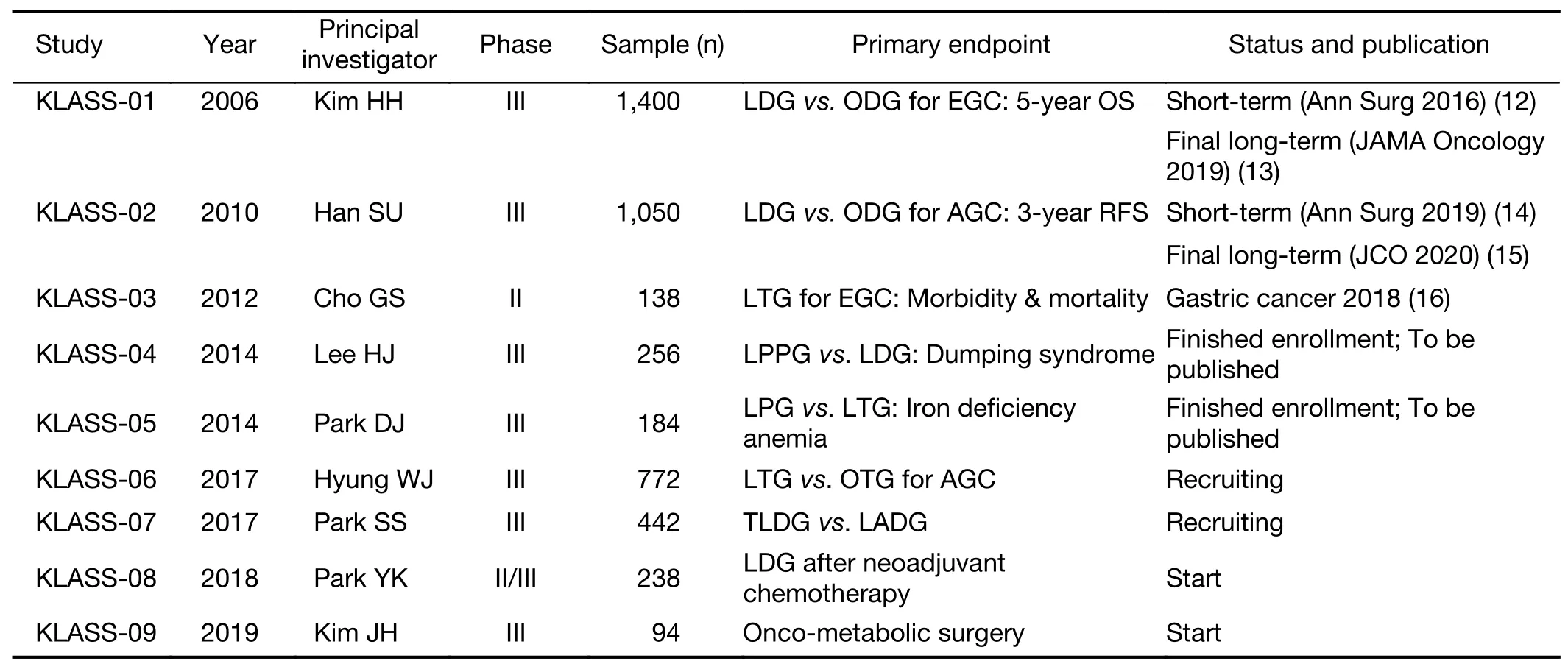
Table 1 Published and ongoing prospective clinical trials from KLASS group
Laparoscopic total gastrectomy (LTG) for EGC
Total gastrectomy is still the standard operation for upper 1/3rd gastric cancer including EGC.Several studies have shown that LTG is feasible and safe (21),but is technically demanding due to the difficulty in the esophagojejunal (EJ)anastomosis,esophagojejunostomy (EJstomy). Several methods of intracorporeal EJstomy have been illustrated in literature,but it can be grouped mainly into using either circular or linear staplers (22).Several studies have been published,which are all retrospective,that compare types of intracorporeal EJ anastomosis.Two literature reviews suggest a relatively higher risk of anastomosis stenosis when a circular stapler is used (23,24).However,there is a wide heterogeneity between the circular EJstomy methods that are being performed,and these results cannot be generalized.A previous study showed that circular EJstomy using an intra-abdominal purse-string suture device (Lap-Jack) had no significant difference in anastomotic complications than linear EJstomy (22).Despite the debate on EJ anastomosis methods,LTG has less short-term morbidity than open total gastrectomy (OTG) (21).The CLASS-02 trial randomized 227 patients with stage I gastric cancer to receive either LTG or OTG (25).The short-term results showed similar overall complication rates (18.1% in the laparoscopic group,17.4% in the open group).So far,evidence seems to suggest that LTG is safe if performed by experienced surgeons.Until well-designed prospective studies on the types of EJ anastomosis method are published,both circular and linear EJstomy are recommended for intracorporeal anastomosis.
Laparoscopic function-preserving gastrectomy for EGC
With the high survival rate in EGC,the attention is now shifting towards less radical surgery,preserving gastric function to attain a higher quality of life (QOL) through the development of function-preserving gastrectomy.Postgastrectomy symptoms such as dumping syndrome,anemia,malnutrition,diarrhea,and postprandial discomfort all interfere with patient QOL.Since the successful spread of LG,minimally invasive surgery has been adapted to function-preserving gastrectomy (26) which includes laparoscopic pylorus-preserving gastrectomy (LPPG)(27,28),laparoscopic proximal gastrectomy (LPG) (29,30),vagus-preserving distal gastrectomy (VPDG) (31),and sentinel lymph node navigation surgeries (32).For EGC at the middle third of the stomach,LPPG was shown to be safe,with better nutritional advantages and less dumping syndrome,but had a higher rate of delayed gastric emptying compared to LDG (7.8%vs.1.7%,P=0.015)(27).The KLASS-04 trial is an RCT comparing LPPG and LDG,and results are to be released soon.For EGC at the proximal third of the stomach,LPG may be performed.Compared to the standard LTG,LPG shows better nutritional change and less postoperative anemia without increasing short-term complications (30). Various anastomotic methods to prevent gastric reflux after proximal gastrectomy have been proposed,such as the double-tract reconstruction (29) and double-flap reconstruction (33).Still,there are not enough studies to determine the best type of reconstruction.
The sentinel node navigation concept has long been investigated on gastric cancer.A prospective multicenter trial held in Japan performed sentinel node mapping using standard dual tracer technique on 397 cT1 or cT2 gastric cancer patients (34).Results showed sentinel node detection rate of 97.5%,and the accuracy of metastatic status based on sentinel node evaluation was 99.0%(383/387).The SENORITA trial is an RCT that used this sentinel node concept to compare the oncological safety of laparoscopic stomach-preserving gastrectomy and sentinel basin dissection to conventional LG (35).A total of 580 patients were randomized.Though long-term results are yet to be published,short-term results show that laparoscopic stomach-preserving gastrectomy with sentinel node navigation is potentially safe with a comparable complication rate to LG.The dual-tracer technique improves the sensitivity and specificity of sentinel node detection compared with when used alone (36).However,recent development in near-infrared technology may allow the use of fluorescent dye alone to be sufficient (37).
LG for AGC
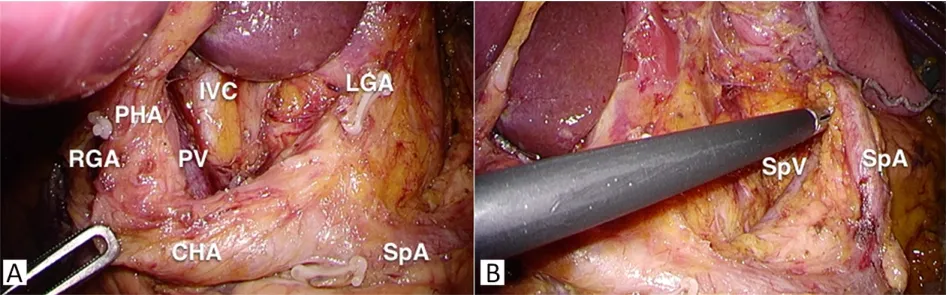
Figure 1 View of suprapancreatic D2 lymph node dissection in laparoscopic gastrectomy. (A) Complete lymph node 12a dissection;(B) Complete lymph node 11p dissection.RGA,right gastric artery;PHA,proper hepatic artery;PV,portal vein;IVC,inferior vena cava;CHA,common hepatic artery;LGA,left gastric artery;SpA,splenic artery;SpV,splenic vein.
Major obstacles in the widespread of LG for AGC are the following:highly technically demanding D2 lymphadenectomy (Figure 1),bulky tumor,total omentectomy,high vasculature,and possibility of tumor invasion to adjacent organs.For locally AGC,prolonging disease-free survival (DFS) should be the primary concern.According to the 15-year long-term analysis of the Dutch D1D2 trial (38),D2 lymph node dissection is associated with lower locoregional recurrence and cancer-specific deaths.Retrospective studies and short-term analyses of prospective trials suggest that LDG for AGC may have possible benefits such as faster recovery,less pain,and lower immediate postoperative complications (39,14).Until now,two large-scale RCTs on the long-term safety of LDG for AGC have been published.The CLASS 01 trial(40) from China was the first multicenter RCT to report its long-term outcomes.In this study,1,056 patients with clinical AGC were randomized to LDG or ODG.The 3-year DFS was 76.5% in the LDG group and 77.8% in the ODG group with an absolute difference of -1.3% and a one-sided 97.5% CI of -6.5%,not crossing the noninferiority margin of -10%.The KLASS-02 trial (15)held in Korea analyzing 1,050 patients with clinical AGC also showed similar results.The 3-year RFS was 80.3% in the LDG group and 81.3% in the ODG group.After adjusting for surgeon stratification,because the surgeon factor was a stratification factor during randomization,the HR was 1.035 (95% CI,0.762-1.406;P=0.039) which was within the upper limit of 1.43 for noninferiority.Although both studies included pathological stage I patients (Table 2)(15,40,41),there was no statistical difference in subgroup analyses by stage.One major limitation in both studies is the larger than expected proportion of EGC patients.In the CLASS-01 trial,22.4% of the LDG group and 25.4%of the ODG group were EGC.In the KLASS-02 trial,27.8% of LDG group and 25.9% of ODG group were EGC.Also,there were also a substantial number of patients who were lost for follow-up,which may have affected the survival calculations at the 3-year period.The final results of the JLSSG-0901 phase III trial from Japan is yet to be published (42),but the results of the phase II study prove its short-term technical safety (41).
LTG for AGC
While LDG for AGC is slowly gaining evidence,there are even fewer studies regarding LTG for AGC,most of them being retrospective and conjoined with other types of LG.Our 15-year analysis of patients who received LG for AGC included 432 patients who received LTG (43).Mean operation time was 251.6±69.8 min,and estimated blood loss was 141.9±171.5 mL.The mean number of retrieved lymph nodes was 70.1±28.9.A case-controlled study by Boet al.(44) reviewed 117 cases of LTG matched with OTG for pT2 and pT3 patients.Operation time was significantly longer by 50 min,but there was significantly less blood loss in LTG group (196.9±88.4vs.358.2±158.7 mL,P=0.024).Postoperative hospital stay was shorter in the LTG group,and there was also less use of analgesic injection in theLTG group.Early complication rate was also lower in the LTG group (11.1%vs.16.3%,P=0.045) specifically having less pulmonary problems and wound infection.The 5-year OS rates were 49.3% and 46.5% in the LTG group and OTG group,respectively,with no statistical difference.Answering the need for a well-designed prospective RCT,the KLASS-06 trial is the first RCT to compare LTG and OTG in patients with AGC that can be curatively treated through total gastrectomy.This trial started in April 2018 and is now ongoing with the primary endpoint being 3-year RFS.Current evidences suggest that LG for AGC is possible,but is still recommended for experienced surgeons,and careful patient selection must be done.
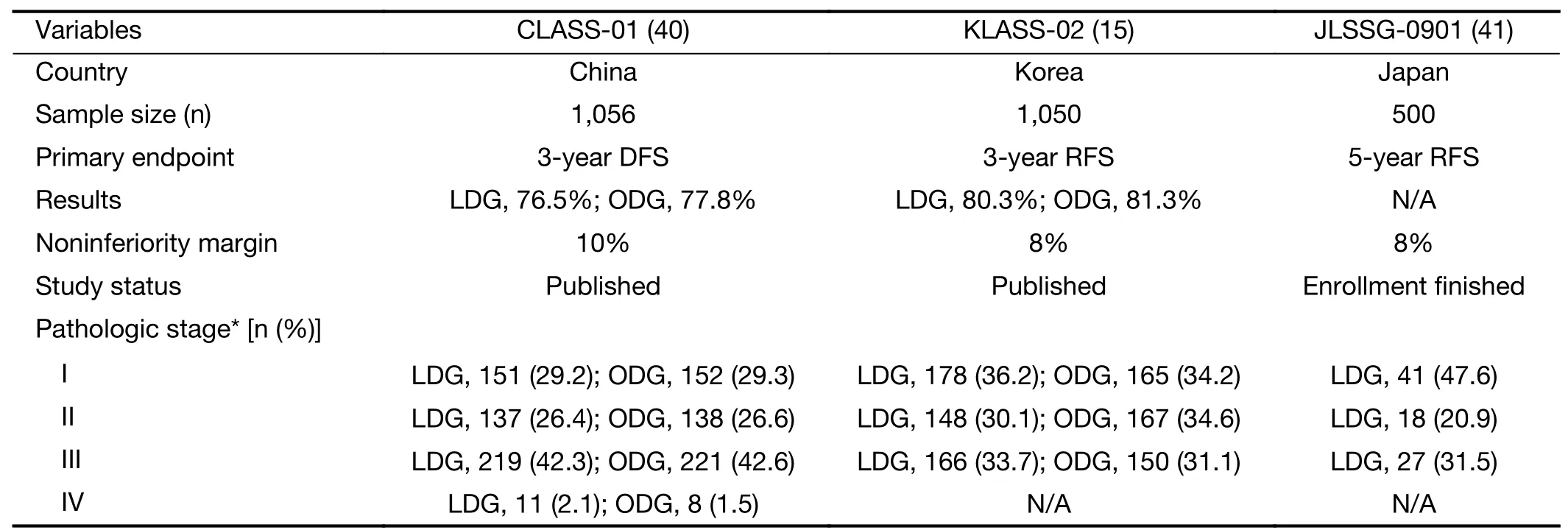
Table 2 Large-scaled randomized clinical studies from East Asia comparing LDG and ODG for AGC
Laparoscopic surgery for stage IV gastric cancer
Studies on the role of laparoscopic surgery for stage IV gastric cancer are rare.In the subgroup analysis of the previously mentioned CLASS 01 trial (40),although there was no statistical difference,3-year DFS was much lower in the laparoscopic group for stage IV gastric cancer(laparoscopy 20.8%,open 58.3%,P=0.060).In the 15-year analysis of LG in our institution (43),63 patients revealed to have pathologic stage IV gastric cancer received LG.The 5-year OS was 25.0%.Although the REGATTA trial(45),which compared chemotherapy alone and gastrectomy followed by chemotherapy for patients with a single site of metastasis,did not show survival benefit of gastrectomy,there are growing evidences that gastrectomy along with maximal metastasectomy may provide some survival benefit(46,47).LG with maximal metastasectomy may be a treatment option for narrowly selected patients.We analyzed 117 consecutive patients with pathologically proven stage IV gastric cancer who underwent either open or laparoscopic radical gastrectomy with concurrent metastasectomy (48).Thirty-six patients in the laparoscopic group were matched to the open group in 1:1 ratio using propensity score matching.There was no significant difference in complication rates,and the 5-year OS was 23.4% in the laparoscopic group and 25.0% in the open group (HR=0.960;95% CI,0.560-1.640;P=0.882).Most of the cases were peritoneal metastasis (61.1%),in which the affected peritoneum was resected,followed by distant lymph node metastasis (31.9%),and distant organ metastasis (7.0%).Although the proper role of LG,even maximal metastasectomy itself,in stage IV gastric cancer is yet to be confirmed,the result of the study suggest that LG and metastasectomy is feasible in selected cases.
The peritoneum is one of the most frequent site of metastasis in gastric cancer,and studies have shown that intraperitoneal chemotherapy may be an effective and safe treatment for peritoneal metastasis (49).The use of heated intraperitoneal chemotherapy (HIPEC) after cytoreductive surgery is known to increase the median survival of these patients from 7.9 months to 15 months (50).HIPEC can be safely reproduced through laparoscopy as a neoadjuvant intraperitoneal chemotherapy (51),achieving a significant reduction in peritoneal cancer index score (52).Pressurized intraperitoneal aerosol chemotherapy (PIPAC) is a novel technique that delivers cytotoxic drugs into the abdominal cavity as an aerosol (53) in a laparoscopic setting.The aerosol form combined with positive capno-pneumoperitoneum generates an artificial pressure gradient that allows deeper drug penetration and better distribution into target peritoneal tissues.Since PIPAC was reported in 2011,PIPAC has been explored using different cytotoxic drugs in various cancers with peritoneal metastasis (53-55).Currently,several studies are being performed to determine the safety of PIPAC according to each drug,and it will take some time before a full large-scale phase III trial can be performed.However,this may be just a start of the development of many more applications of laparoscopy for stage IV gastric cancer.
Future of LG
Technology is evolving at an extremely high speed as new machines,devices,and other surgical materials are being developed and introduced to the market. Various laparoscopic devices and instruments such as the singleincision glove ports,intra-abdominal organ retractors,and articulating laparoscopic graspers have been developed,allowing more freedom of movement in performing LG.This progress allowed the development of more minimally invasive techniques such as reduced-ports LG and singleport laparoscopic gastrectomy (SLG).Since the first report of single-port distal gastrectomy in 2011 by Omoriet al(56),reports of SLG for other types of gastrectomy have been published (57-59).An RCT by Omoriet al.(60)randomized 101 patients to receive either conventional LG(multi-port) or SLG.Postoperative pain was significantly lower in the SLG group,and analgesics were administered significantly less in the SLG group.While many evidences show that SLG is feasible and safe,it is still a technically demanding procedure even to surgeons who have passed the learning curve for LG.Although many advancements have made reduced-ports LG or SLG become technically feasible today,more innovative devices and techniques are still needed in order to shorten its learning curve and allow the technique to become generalized to the public.
With the introduction of the robotic system in the form of the DaVinci surgical platform,some surgeons may have predicted the early demise of the laparoscopic era to come within few years.However,the current robotic system is mainly a master-slave system,lacking tactile sense that is crucial for safe and precise operation.Many retrospective studies on the feasibility of robotic gastrectomy to patients with EGC have been published,but only few prospective studies have been reported.One prospective single-arm study by Uyamaet al.(61) showed that robotic gastrectomy may reduce morbidity rate when compared to a historical control cohort.On the other hand,a multi-center prospective comparative study conducted by Kimet al.(62)that compared 223 robotic gastrectomy cases with matched 211 LG cases resulted in no benefit of robotic gastrectomy over LG.Operation time was longer for robot gastrectomy and had significantly higher costs.Robotic gastrectomy has yet to prove its cost-effectiveness over LG,allowing LG to maintain its role being as the major treatment option for EGC.
The focus of research on laparoscopic surgery for gastric cancer should now move on from proving its noninferiority to demonstrating its superiority as treatment for gastric cancer.Unlike how it started,laparoscopic surgery is not just about reducing the size of the incision.It is now about using technology to augment human capabilities in performing the operation the best way possible.High resolution cameras can magnify tissues beyond human sight,allowing the visualization of small vessels,lymphatics,and never tissues (63).Flexible cameras and intraabdominal organ retractors show areas that can be difficult to see during open resection (64).Laparoscopy using cameras with near-infrared radiation imaging can use augmented reality to guide the operator in lymph node dissection and obtaining sufficient tumor margin (37)through the injection of fluorescent dye.Minimally invasive surgery may even allow the surgeons to prolong the prime of their career not only through magnified vision,but also by reducing postural risk (65).
Conclusions
LG is now a widely accepted procedure for gastric cancer treatment.However,it is still early to generalize its safety to more complex cases such as AGC and LTG.Innovations in surgical tools show that there is still potential for the field of LG to expand.
Acknowledgements
None.
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
杂志排行
Chinese Journal of Cancer Research的其它文章
- Landscape of cell heterogeneity and evolutionary trajectory in ulcerative colitis-associated colon cancer revealed by single-cell RNA sequencing
- Combined detection and subclass characteristics analysis of CTCs and CTECs by SE-iFISH in ovarian cancer
- Multicenter phase II study of apatinib single or combination therapy in HER2-negative breast cancer involving chest wall metastasis
- Effect of preoperative nutrition therapy type and duration on short-time outcomes in gastric cancer patient with gastric outlet obstruction
- Novel therapies targeting hypoxia mechanism to treat pancreatic cancer
- Clinical challenges in neoadjuvant immunotherapy for non-small cell lung cancer