Multicenter phase II study of apatinib single or combination therapy in HER2-negative breast cancer involving chest wall metastasis
2021-05-19HuipingLiCuizhiGengHongmeiZhaoHanfangJiangGuohongSongJiayangZhangYaxinLiuXinyuGuiJingWangKunLiZhongshengTongFangyuanZhaoJunlanYangGuoliangChenQianyuLiuXuLiang
Huiping Li,Cuizhi Geng,Hongmei Zhao,Hanfang Jiang,Guohong Song,Jiayang Zhang,Yaxin Liu,Xinyu Gui,Jing Wang,Kun Li,Zhongsheng Tong,Fangyuan Zhao,Junlan Yang,Guoliang Chen,Qianyu Liu,Xu Liang
1Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing),Department of Breast Oncology,Peking University Cancer Hospital &Institute,Beijing 100142,China;2Breast Disease Diagnostic and Therapeutic Center,the Fourth Affiliated Hospital of Hebei Medical University,Shijiazhuang 050019,China;3 Department of General Surgery,Peking University Third Hospital,Beijing 100191,China;4Department of Breast Oncology,Key Laboratory of Breast Cancer Prevention and Therapy,National Clinical Research Center for Cancer,Tianjin Medical University Cancer Institute and Hospital,Tianjin 30060,China;5 Department of the Public Health Sciences,University of Chicago,Chicago 60637,USA;6Department of Medical Oncology,Chinese PLA General Hospital,Beijing 100853,China;7Jiangsu Hengrui Medicine Co.Ltd.,Shanghai 200120,China
Abstract Objective:Breast cancer (BC) with chest wall metastasis (CWM) usually shows rich neovascularization.This trial explored the clinical effect of apatinib on human epidermal growth factor receptor 2 (HER2)-negative advanced BC involving CWM.Methods:This trial involved four centers in China and was conducted from September 2016 to March 2020.Patients received apatinib 500 mg/d [either alone or with endocrine therapy if hormone receptor-positive (HR+)]until disease progression or unacceptable toxicity.Progression-free survival (PFS) was the primary endpoint.Results:We evaluated 26 patients for efficacy.The median PFS (mPFS) and median overall survival (mOS) were 4.9 [range:2.0-28.5;95% confidence interval (95% CI):2.1-8.3]months and 18 (range:3-55;95% CI:12.9-23.1)months,respectively.The objective response rate (ORR) was 42.3% (11/26),and the disease-control rate was 76.9% (20/26).In the subgroup analysis,HR+patients compared with HR-negative patients had significantly improved mPFS of 7.0 (95% CI:2.2-11.8) months vs. 2.3 (95% CI:1.2-3.4) months,respectively (P=0.001);and mPFS in patients without or with chest wall radiotherapy was 6.4 (95% CI:1.6-19.5) months vs. 3.0 (95% CI:1.3-4.6) months,respectively (P=0.041).In the multivariate analysis,HR+status was the only independent predictive factor for favorable PFS (P=0.014).Conclusions:Apatinib was highly effective for BC patients with CWM,especially when combined with endocrine therapy.PFS improved significantly in patients with HR+status who did not receive chest wall radiotherapy.However,adverse events were serious and should be carefully monitored from the beginning of apatinib treatment.
Keywords:Apatinib;advanced breast cancer;chest wall metastasis;HER2-negative
Introduction
Tumor metastasis is responsible for most cancer deaths.Chenet al.reported that female breast cancer (BC) was the most commonly diagnosed cancer in Chinese patients in recent years.There were an estimated 27.9×104newly diagnosed BC cases and 6.6×104related deaths,and it was a frequent cause of cancer death in women aged 45-59 years(1).Once diagnosed with BC,25%-50% of patients will eventually develop metastasis (2). The mechanism underlying tumor metastasis is complex and includes many factors,such as molecular biology,genetics,and angiogenesis.Additionally,different molecular subtypes tend to have distinct initial metastatic sites.For instance,human epidermal growth factor receptor 2 (HER2)-positive BC mainly metastasizes to the liver,triple-negative BC (TNBC) to the lung,and hormone receptor-positive(HR+) BC to the bone (Figure 1A).However,regardless of the subtype,the rate of chest wall and lymph node metastasis is higher in all molecular subgroups (Figure 1B)(3,4).Recently,Songet al.(5) reported that neutrophil extracellular traps (NETs) are abundant in breast and colon cancer with liver metastases,and detecting serum NETs can predict liver metastasis of BC at an early stage.This indicates that studying organ specificity of tumor metastasis may allow us to better understand tumor behavior and lead to improved therapeutic approaches.
Angiogenesis plays an important role in tumor formation,invasion,and relapse.Vascular endothelial growth factor (VEGF) and its receptors play an essential role in the angiogenesis signaling pathway,especially VEGF receptor 2 (VEGFR2) (6,7).Bevacizumab inhibits tumor angiogenesis by binding to and inhibiting VEGF.Multiple clinical studies have confirmed that the combination of bevacizumab with chemotherapy can prolong progression-free survival (PFS) in BC patients (8-12).VEGF-tyrosine kinase inhibitors (VEGF-TKIs),such as sunitinib and sorafenib,have been used clinically in metastatic BC patients for their anti-tumor activity in combination with chemotherapy (13).
Apatinib is another oral TKI that selectively targets VEGFR-2 to inhibit tumor angiogenesis (14),and apatinib has reported activity in BC (15,16).However,BC with chest wall metastasis (CWM) has a rich blood supply because of the high expression of angiogenic factors.Previous study found that microvessel density (MVD)assessment was associated with poorer prognosis in luminal A subtype (17).In general,CWM is usually associated with increased tumor MVD,the appearance of skin lesions,and dermal lymphatic invasion.Previously conducted research reported that lymphangitic BC is pathologically characterized by high vascularity,skin lymphatic vessel infiltration,and increased MVD because of the high expression of angiogenic factors.This study also assessed the potential of circulating endothelial cells,circulating endothelial progenitors,and circulating pericyte progenitors as surrogate biomarkers of the response to angiogenesis inhibitor treatment (18).Another study reported that the vascular and connective tissue structures of tumors develop a tissue columns (centrally located single microvessels embedded in connective tissue and smooth muscle actin-expressing myofibroblasts surrounded by basement membrane).Although the size of these tissue columns was fairly uniform in different organs,they found significantly larger tissue columns in the skin compared with other organs (19).Whether apatinib is also effective for BC with CWM remains unknown (20,21).Precise treatment usually refers to therapy using molecular markers.Therefore,in current clinical trial designs,organ specificity is typically not the main consideration.Nevertheless,in our clinical practice,we found that the type of organ metastasis differed among molecular subtypes.Patients with CWM may have increased VEGFR expression and rich neovascularization,which are possibly associated with a better response to angiogenesis inhibitors.We found that bevacizumab rapidly shrank metastases in the chest wall,especially tumors with a rich blood supply(22).Therefore,we designed this clinical trial based on organ characteristics to evaluate the efficacy of apatinib in HER2-negative advanced breast cancer (ABC) with CWM.To our knowledge,this article is one of the few focusing on the characteristics of organ metastasis.
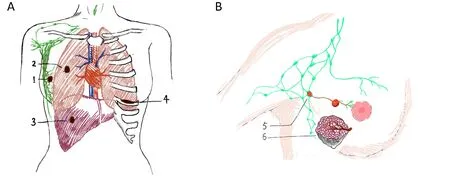
Figure 1 Breast cancer organ specificity of metastasis.(A) Primary tumor and main metastasis organs;(B) lymph node and chest wall metastasis.1,primary tumor in breast;2,lung metastasis;3,liver metastasis;4,bone metastasis;5,lymph node metastasis;6,chest wall metastasis.
Materials and methods
Inclusion criteria
We enrolled patients ≥18 years of age with HER2-negative ABC and CWM (with or without other metastasis sites)confirmed by histology or cytological examination who underwent a first-line chemotherapy regimen or could not tolerate standard first-line treatment.Patients had an Eastern Cooperative Oncology Group performance status of 0 or 1 and at least one measurable disease according to the Response Evaluation Criteria in Solid Tumors version 1.1.Patients also had adequate hematologic,hepatic,renal,and cardiac function,and all patients provided informed consent.
Patients were excluded for the following reasons:radiotherapy within 4 weeks before enrollment;brain metastasis;other carcinomas within 5 years;uncontrolled hypertension despite antihypertensive therapy;myocardial ischemia (≥grade 2),myocardial infarction,or arrhythmia(≥grade 2;QTcF >470 ms);grade III-IV cardiac insufficiency according to the New York Heart Association standard or left ventricular ejection fraction <50%;gastrointestinal disorder or other factors (dysphagia,chronic diarrhea,or intestinal obstruction) that may interfere with drug absorption.
This study was approved by the Ethics Committee of Beijing Cancer Hospital (No.2016YJZ19-GZ01) and is registered at ClinicalTrials.gov (No.NCT02878057).
Drug administration
All patients received apatinib 500 mg/d as the starting dose followed by once per day every 4 weeks as one cycle.Apatinib was continued until disease progression,death,consent withdrawal,or unacceptable adverse events after a 50% dose reduction.In addition to apatinib,HR+patients also received endocrine therapy.Apatinib was partially supplied by Jiangsu HengRui Medicine Co.Ltd.,Shanghai,China.
The dose of apatinib was reduced to 250 mg/d when patients experienced the following:grade 3/4 hypertension,nausea,vomiting,proteinuria,and diarrhea;grade 4 hematologic adverse events;or other grade 3/4 nonhematologic adverse events.
Experimental design
This phase II,open-label,single-arm study involved four centers in China.PFS was the primary endpoint and was defined as the time from the beginning of enrollment to tumor progression or death from any cause,whichever occurred first.Secondary endpoints were the objective response rate (ORR),which included complete response(CR) and partial response (PR) rates,overall survival (OS),disease-control rate (DCR),safety,and tolerability.OS was the duration from the date of enrollment to death from any cause or the last visit.DCR included CR,PR,and stable disease (SD) for at least 8 weeks.Patients were evaluated by computed tomography (CT) or magnetic resonance imaging (MRI) at baseline and every 2 cycles (q 8 weeks)until disease progression.Follow-up was performed every 2 months until death or the end of the study.Adverse events were recorded in accordance with the US National Cancer Institute Common Terminology Criteria for Adverse Events,version 4.03.
Statistical analysis
SPSS software (Version 17.0;SPSS Inc.,Chicago,IL,USA) was used for all statistical analyses.Median PFS(mPFS) was analyzed using the Kaplan-Meier method.Adverse events data were collected from all patients who received even a single dose of apatinib.
PFS and OS for patients who received at least 8 weeks of apatinib treatment were analyzed using the Kaplan-Meier method (unless progression occurred during the 8 weeks of treatment).Univariate and multivariate analyses were performed using log-rank tests and Cox regression models,and P<0.05 was considered statistically significant.
Results
Baseline patient characteristics
Thirty patients were enrolled in this trial between September 2016 and July 2019,and the last follow-up date was March 30,2020.Patient baseline characteristics are listed inTable 1.The median age was 49.5 (range:35-69)years,and 20 (66.7%) patients were HR+.Other than CWM,the most common metastasis sites were lymph nodes,lung,bone,and liver;17 (56.7%) patients had more than two metastatic sites,and approximately half (16/30;53.3%) of patients had ≥three lines of metastatic disease.Twenty (66.7%) patients were pre-treated multiple times with endocrine therapy (Table 1).All patients underwent prior chemotherapy regimens before enrollment,and the median follow-up duration was 18 (range:3-55) months.
There were 13 cases with CWM only,and one case could not be evaluated for efficacy.Seventeen cases showed chest wall and other metastasis sites,including the lymph node,bone,liver,and lung,and three cases could not be evaluated for efficacy.In the evaluable 26 cases,there was no significant difference in the mPFS between patients with CWM only (4.9 months) or simultaneously with other metastasis sites (4.3 months) (P=0.258).
Efficacy
After a median follow-up of 18 months,four patients discontinued apatinib therapy because of adverse events(grade 2 hypertension in two and grade 2 nausea in two).Because these patients were treated for less than 8 weeks,they were evaluated for safety but not efficacy.The response of 26 (86.7%) patients was assessed.The mPFS and mOS were 4.9 months [range:2.0-28.5 months;95%confidence interval (95% CI):2.1-8.3]and 18 months(range:3-55 months;95% CI:12.9-23.1),respectively(Table 2,Figure 2A,B).For the efficacy-evaluated patients,the ORR (0 CR,11 PR) was 42.3% (11/26),and the DCR(0 CR,11 PR,9 SD) was 76.9% (20/26) (Table 2).In patients reaching PR,SD and PD,the mPFS was 14.4,2.0 and 2.3 months,respectively (P<0.001);the mOS was not evaluated,7 and 20 months,respectively (P=0.029) (Table 2,Figure 2C,D).In the subgroup analysis,HR+patients(apatinib combined with endocrine therapy) had significantly improved survival compared with TNBC(apatinib monotherapy) patients;the mPFS was 7.0 (95%CI:2.2-11.8) monthsvs.2.3 (95% CI:1.2-3.4) months,respectively (P=0.001).In patients withoutvs.with chest wall radiotherapy,the mPFS was 6.4 (95% CI:1.6-19.5)monthsvs.3.0 (95% CI:1.3-4.6) months (P=0.041),respectively (Table 3,Figure 3A,B).No lymph node metastasis occurred after surgery,and the site and number of metastases showed superior PFS benefit but without statistical significance (P=0.112 and 0.258,respectively)(Table 3,Figure 3C,D).In the multivariate analysis,the following factors were included:molecular subtype,lymph node metastasis after surgery,disease-free survival (DFS),endocrine therapy prior to enrollment,radiation therapy prior to enrollment,site and number of metastases,and line of disease prior to enrollment.HR+was the only independent predictive factor for PFS (P=0.014),and chest wall radiation therapy was not associated with substantiallyimproved PFS (P=0.057).Longer OS was associated with HR+status and CWM only (P=0.042 and P=0.031,respectively) (Table 3).Tumors in the chest wall clearly shrank with apatinib therapy,with 9 of 11 patients reaching PR in two cycles and another 2 patients reaching PR in four cycles (Figure 4,5).
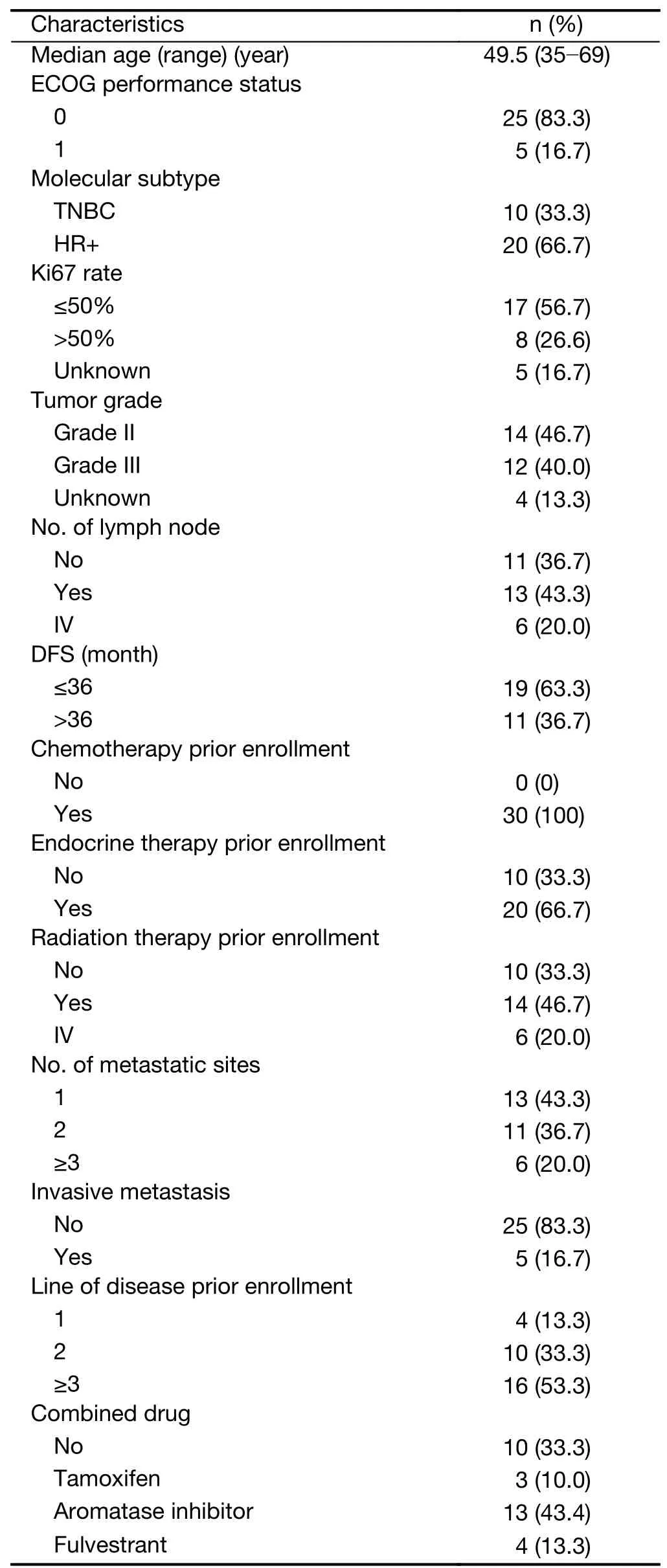
Table 1 Patient characteristics at baseline of enrollment (N=30)
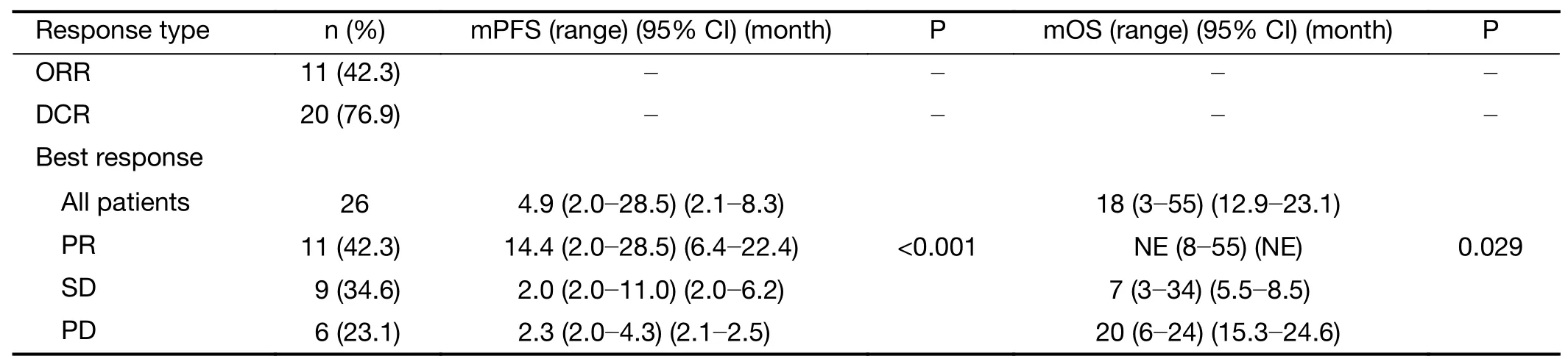
Table 2 Best response in evaluated patients (N=26)
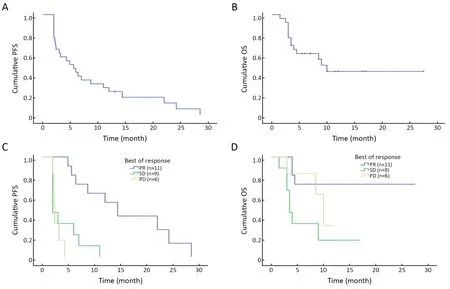
Figure 2 Kaplan-Meier survival curves showed efficacy of apatinib-treated patients.(A) PFS [mPFS=4.9 (range,2.0-28.5;95% CI,2.1-8.3)months];(B) OS [mOS=18 (range,3-55;95% CI,12.9-23.1) months];(C,D) PFS and OS benefit related to different response (PFS,P<0.001;OS,P=0.029).PFS,progression-free survival;mPFS,median PFS;95% CI,95% confidence interval;OS,overall survival;mOS,median OS;PR,partial response;SD,stable disease;PD,progression disease.
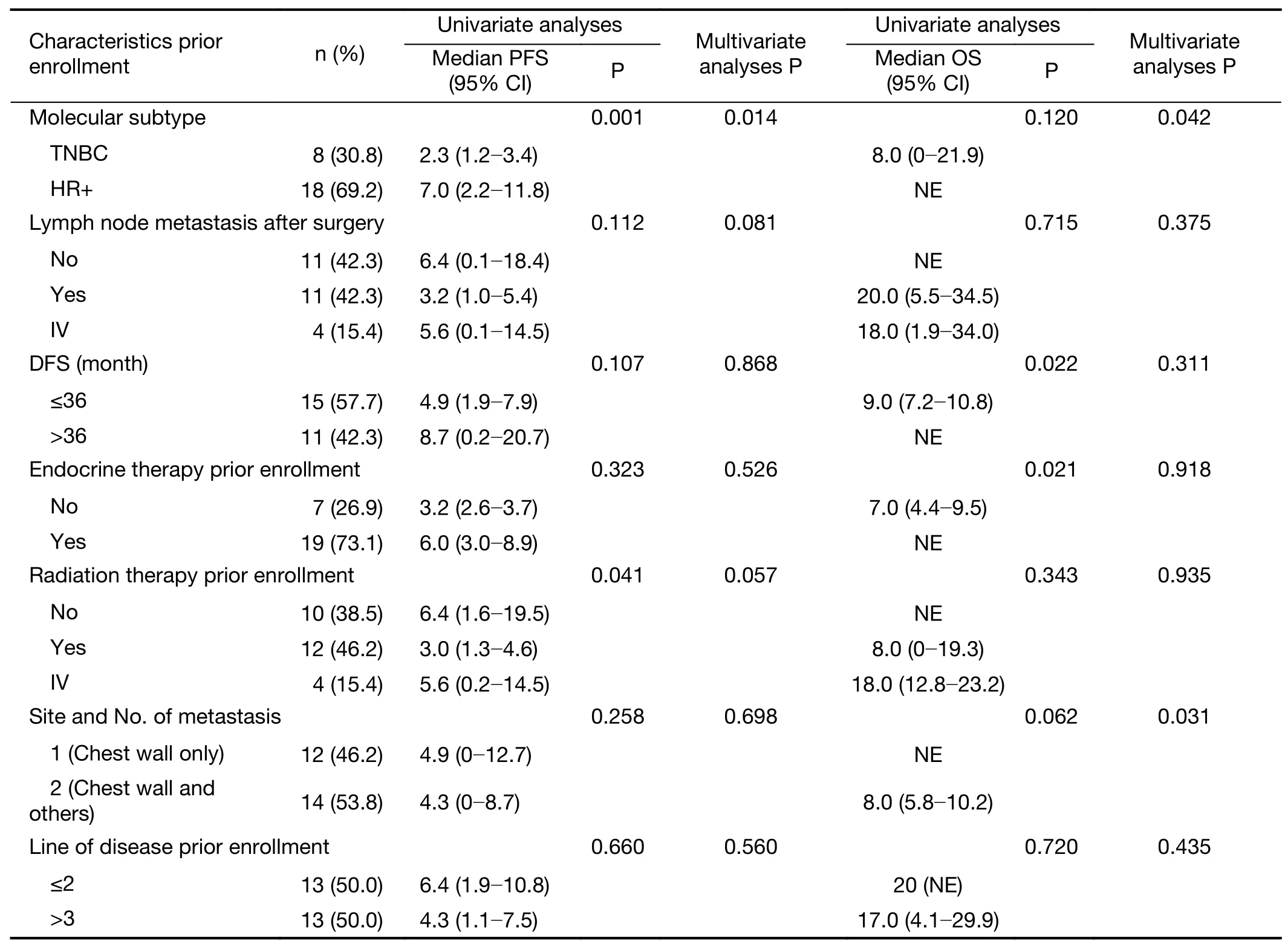
Table 3 Univariate and multivariate analyses of evaluable efficacy PFS patients (N=26)
Safety
Because of adverse events,the apatinib dose was reduced from 500 mg to 250 mg for most patients (18/30,60.0%),and some patients received 500 mg and 250 mg every other day (10/30,33.3%).
The drug-related adverse event rates were 50.0% for grade 1,66.7% for grade 2,and 40.0% for grade 3 (Table 4).Grade 4 and fatal adverse events were observed,although most adverse events were mild (grade 1-2) and manageable.The most common adverse events for all grades were hypertension (50.0%;grade 3,6.7%),proteinuria (33.3%;grade 3,20.0%),nausea (13.3%;grade 3,0),fatigue (13.3%;grade 3,3.3%),and increased bilirubin concentration (10.0%;grade 3,6.7%).Other adverse events are listed inTable 4.Two patients exhibited a large ulcer in their chest wall;one experienced serious bleeding,and the other patient’s entire chest wall was necrotic and exposed.Four patients discontinued the treatment due to adverse events (grade 2 hypertension in two and grade 2 nausea in two).
Discussion

Figure 3 Cumulative PFS of apatinib-treated patients in different sub-group.(A) HR status (P=0.001);(B) Radiation therapy after surgery in chest wall (P=0.041);(C) Lymph node metastasis after surgery (P=0.112);(D) Site and number of metastasis (P=0.258).PFS,progressionfree survival;HR,hormonal receptor;IV,primary metastasis.
Effective screening programs and novel therapeutic strategies are attributed to a continuous downtrend in cancer mortality.In an analysis of age-standardized cancer incidence and mortality rates,breast cancer ranks first for incidence,with 36.1 new cases per 100,000 population,but the mortality figures reflected a better chance of survival,with 8.8 deaths per 100,000 population,ranking the sixth after lung,stomach,liver,esophagus and colorectal cancer (23).
Sustained angiogenesis plays an important role in promoting tumor development and metastasis.Compared with traditional treatments,anti-angiogenic medications improve the efficacy of chemotherapy in multiple ways(24).MVD is considered a critical prognostic factor influencing survival (25).The efficacy of bevacizumab,the first monoclonal antibody targeting VEGF,is controversial in BC treatment.The first multicenter phase 3 clinical trial(462 patients) to examine the efficacy of bevacizumab with chemotherapy in pre-treated ABC was published in 2005.Patients were randomly assigned to treatment with capecitabine alone or in combination with bevacizumab(11).According to the primary endpoint of PFS,there was no significant difference between the two groups (4.86 monthsvs.4.17 months,respectively;hazard ratio:0.98;95% CI:0.77-1.25).The subsequent AVADO (2010) trial of bevacizumab combined with docetaxel showed that PFS was statistically significantly different between the control group and the bevacizumab combination group,but the authors found no difference for OS (8).Regarding oral VEGFR-TKIs,monotherapy with sunitinib or sorafenib in ABC patients resulted in an mPFS of 2.5-3.6 months (26-29).
Apatinib is a selective inhibitor of VEGFR-2,and the drug has been widely used in the treatment of various tumors since its development,including gastric cancer,non-small-cell lung cancer,and BC (15,16,30-33).Our study aimed to assess the activity and safety of apatinib in multiple pre-treated HER2-negative ABC patients with CWM.To our knowledge,this is the first trial evaluating apatinib therapy specifically for CWM.We observed that the mPFS and mOS of the 26 evaluated patients were 4.9 months and 18.0 months,respectively.Additionally,the ORR was 42.3%,and the DCR was 76.9%.This trial showed better effects of apatinib compared with previousreports.Two previous studies evaluated apatinib in ABC(15,16) and 38 non-TNBC patients with advanced disease who were previously treated with anthracycline,taxanes,and capecitabine.Using apatinib alone achieved an mPFS and mOS of 4.0 months and 10.3 months,respectively,an ORR of 16.7%,and a DCR of 66.7% (15).In 56 patients with TNBC,the mPFS and OS were 3.3 months and 10.6 months,respectively;the ORR was 10.7% (16).In addition,results from an observational study investigating the antitumor activity and safety of apatinib combined with chemotherapy in 85 heavily and repeatedly treated ABC patients in clinical practice revealed an mPFS and mOS of 4.4 months and 11.3 months,respectively (32).A subgroup analysis of the patients with TNBC revealed an mPFS and mOS of 5.2 months and 11.4 months compared with an mPFS and mOS in the non-TNBC group of 4.3 months and 11.3 months,respectively.
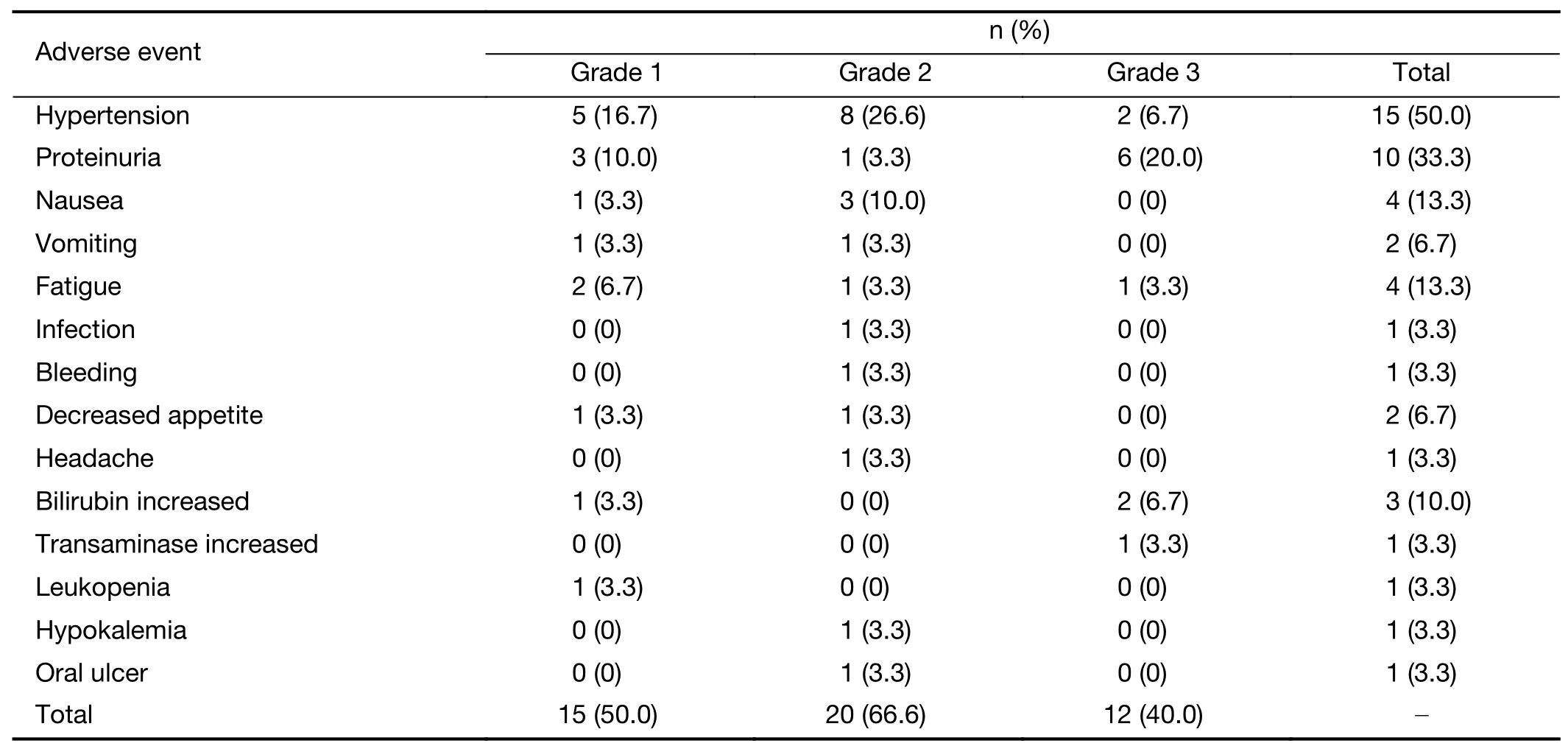
Table 4 Adverse events in all patients graded based on CTCAE 4.0 (N=30)
The reason for the improved response in this study may be that all enrolled patients had CWM,with almost half(46.2%) having only CWM.Figure 4shows the huge chest wall masses in the patient’s chest wall.Although the metastatic masses were large,they had a rich blood supply.Some patients also showed metastasis to other sites,and similar effects as those for CWM were observed.Therefore,it is implied that even if this type of tumor metastasizes to other parts of the body,the blood supply may be relatively abundant.After initiating apatinib for its anti-VEGFR effects,the tumors shrank quickly.Furthermore,among 11 patients,9 achieved PR in the second cycle (Figure 4),and 2 reached PR in the fourth cycle (Figure 5),indicating that patients with CWM were more likely to obtain benefit from apatinib treatment.
In this study,in HR+patients treated with apatinib combined with endocrine therapy,the mPFS was 7.0 (95%CI:2.2-11.8) months,which is almost 3-4 months longer than in previous reports (15,16,32).This degree of improvement may have resulted from the combination of apatinib and endocrine therapy,which differed from the treatment in previous studies in which apatinib was administered in combination with chemotherapy.Previous treatments focused more on TNBC,and apatinib was mainly combined with chemotherapy in several important clinical studies (8,9).There is evidence of crosstalk between estrogen receptors and VEGFRs.For example,anin vitrostudy found that estrogen mainly enhances the angiogenic cascade that is essential for tumor growth by releasing VEGF (34).Therefore,anti-estrogen therapy in estrogenreceptor-positive BC may potentially modify VEGF production.However,with acquired drug resistance in BC and endometrial cancer,it is clear that selective estrogen receptor-modulator (SERM) (tamoxifen and raloxifene)-stimulated tumors induce angiogenic growth (35).A previous study found that TAMR-MCF-7 cells showed increased expression of VEGF,leading to enhanced angiogenesis (36).Compared with control MCF-7 cells,the angiogenic potential is increased in TAMR-MCF-7 cells via the upregulation of VEGF expression.Regulating the VEGF pathway may also involve estrogen receptors(37,38).Another study in animal models using the targetspecific agents tamoxifen (SERM) and brivanib alaninate(VEGFR-2 inhibitor) found that the combination of these drugs showed enhanced anti-tumor activity compared with either tamoxifen or brivanib alaninate as a single agent (39).Previous study also showed that annexin A2 (ANXA2)overexpression regulates plasmin generation and suspected promotes neoangiogenesis in TNBC.Blocking of ANXA2 significantly inhibited neoangiogenesis and resulted in inhibition of tumor growth (40).
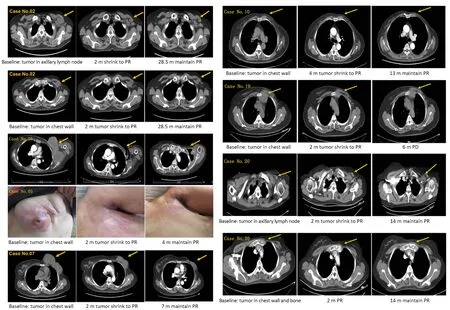
Figure 4 Examples of effective cases:each one showed in base line and tumor shrink to PR and maintain PR,case No.19 showed PD.m,month;PR,partial response;PD,progression disease.
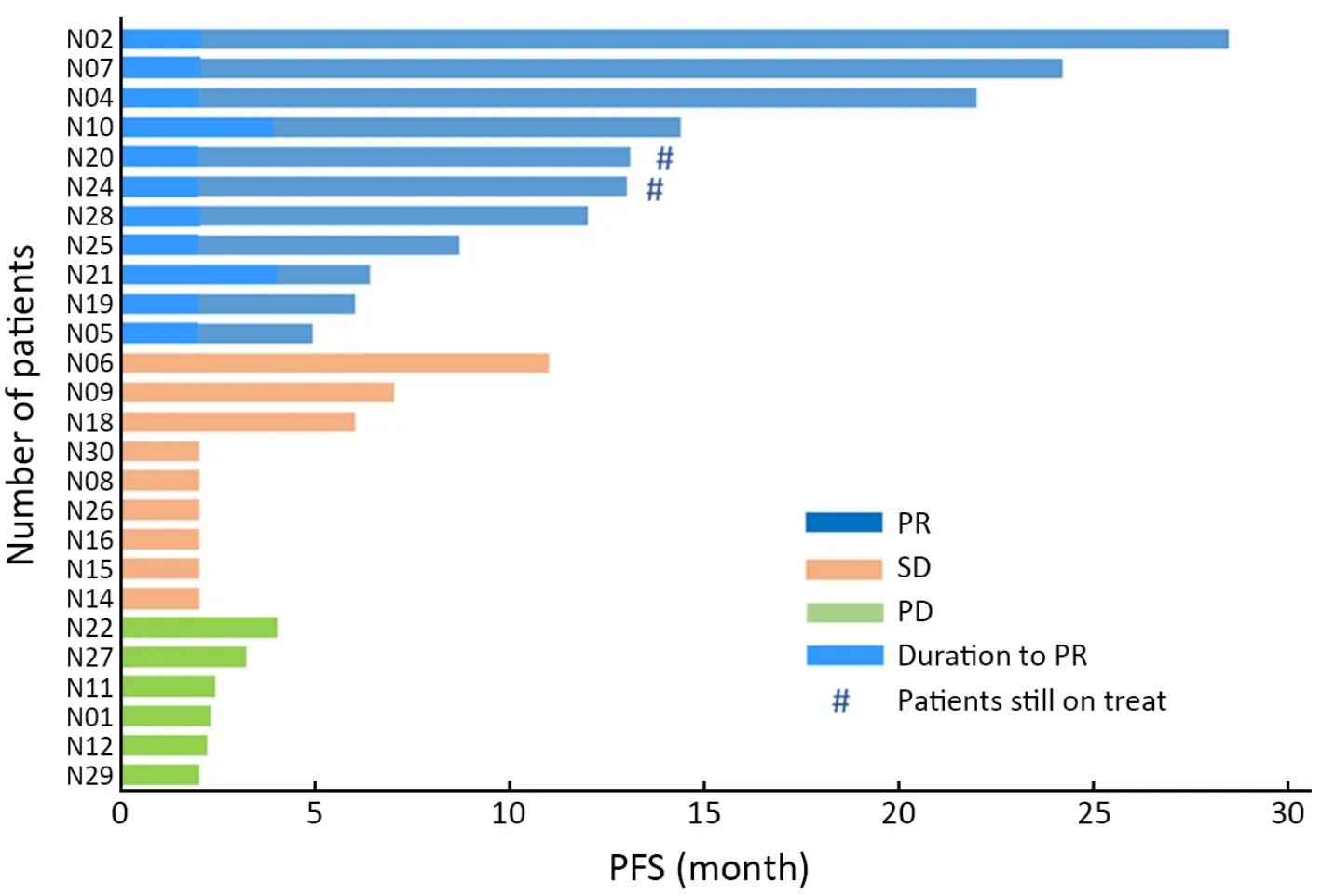
Figure 5 PFS of different response and duration reached to PR.PFS,progression-free survival;PR,partial response;SD,stable disease;PD,progression disease.
Patients with HR+status showed improved survival with endocrine therapy,which can induce endocrine resistance and increase VEGF and VEGFR expression;therefore,inhibiting both HRs and VEGFRs may potentially improve therapeutic outcomes.This finding also indicates that for HR+patients,inhibiting both HRs and VEGFRs provide more benefit than inhibiting VEGFRs alone.The outcomes of the current trial indicated that VEGF-TKIs combined with endocrine therapy have potential antitumor activity,and this approach may be a new favorable option for HR+resistant patients.
This study also found that the benefit of apatinib therapy differed significantly between patients with and without chest wall radiation before enrollment (3.0 monthsvs.6.4 months,respectively;P=0.041).Due to the relatively low oxygen conditions in cancer,angiogenesis is a key event for the maintenance and growth of cancer cells.Although nonvascular-derived growth factors (such as fibroblast growth factor) are also involved in angiogenesis,fibrosis-related proteins (such as galectin-3,Smad 2/3,and transforming growth factor type beta 1) are upregulated after radiotherapy and support histopathological changes leading to vascular disease (41).In addition,postoperative complications in irradiated patients can be explained by the increase in endothelial dysfunction caused by lectin-like oxidized low-density lipoprotein 1 in patients who have previously been irradiated (36,37).These results emphasize that increased fibrosis of the blood vessel wall after radiotherapy may influence the effect of apatinib.Lymphangiogenesis may be related to the VEGFC/VEGFR3 pathway,whereas apatinib acts mainly as a VEGFR-2 inhibitor (42,43).According to our results,VEGF-TKIs combined with endocrine therapy in patients without chest wall radiation and with lymph node metastasis from the primary tumor have potential antitumor activity.
In this trial,the most frequent adverse events for all grades were hypertension (50.0%),proteinuria (33.3%),and nausea (13.3%),with similar rates to those reported previously,especially in ABC (15,16,44).Most adverse events were mild at grade 1-2,grade 3 adverse events occurred in 40.0% of the patients,and no grade 4 adverse events were observed.No treatment-associated mortality occurred during the combined treatment.In this study,60.0% (18/30) of the patients had a dose reduction from 500 mg to 250 mg during treatment because of toxicities,and 13.3% (4/30) of the patients discontinued the treatment due to adverse events.One hypothesis describing the mechanism for the hypertension observed in our patients is that the inhibitory effect of arterial endothelial cells on VEGFR may lead to a decrease in the release of nitric oxide,which acts on arterial smooth muscle cells to cause vasodilation (45).In addition to reducing the apatinib dose,angiotensin receptor blockers,such as valsartan,can also be used to control hypertension.Patients can also recover quickly from proteinuria,and symptoms can be well tolerated after interrupting or reducing the dose.
The limitation of this study is that the sample size was relatively small.This limitation may be more reflected in the subgroup analysis,but because HR+patients had significantly longer mPFS,it might also imply that the combination of angiogenesis inhibitors plus endocrine therapy provides a highly effective treatment.In addition,some patients withdrew from the study even with stage 2 hypertension.To address this limitation,further clinical trials are needed with larger sample sizes.Additionally,the adverse events related to apatinib therapy require careful management from the beginning of treatment.Among the adverse events,special attention should be paid to managing hypertension and the risk of local huge ulcers and bleeding caused by rapid tumor shrinkage.
Conclusions
Apatinib showed excellent efficacy in pre-treated BC with CWM,with significantly improved PFS in HR+patients and patients with no chest wall radiotherapy and longer OS for patients who achieved PR.HR+patients showed better outcomes when treated with apatinib combined with endocrine therapy,which may be a new option for VEGFR inhibitor treatment.However,adverse events can be serious and should be well managed from the beginning of apatinib treatment.
Acknowledgements
None.
Footnote
Conflicts of Interest:The authors have no conflicts of interest to declare.
杂志排行
Chinese Journal of Cancer Research的其它文章
- Recent updates and current issues of sentinel node navigation surgery for early gastric cancer
- Current status and challenges in sentinel node navigation surgery for early gastric cancer
- Screening for gastric cancer in China:Advances,challenges and visions
- Current status and future perspectives on neoadjuvant therapy in gastric cancer
- Current status of lymph node dissection in gastric cancer
- Clinical challenges in neoadjuvant immunotherapy for non-small cell lung cancer