Presentation and surgical management of xanthogranulomatous cholecystitis
2021-05-19MximosFrountzsDimitriosShizsEfstthiLitsouKonstntinosEonomopoulosChristinNikolouKonstntinosApostolouKonstntinosToutouzsEvnglosFlkours
Mximos Frountzs ,Dimitrios Shizs ,Efstthi Litsou ,Konstntinos P Eonomopoulos ,Christin Nikolou ,Konstntinos G Apostolou ,Konstntinos G Toutouzs ,Evnglos Flkours
a First Propaedeutic Department of Surgery, Hippocration General Hospital, National and Kapodistrian University of Athens, School of Medicine, 114 Vas.Sofias Ave. 11527, Athens, Greece
b Laboratory of Experimental Surgery and Surgical Research, National and Kapodistrian University of Athens, School of Medicine, 15B Ag. Thoma Str. 11527,Athens, Greece
c First Department of Surgery, Laikon General Hospital, National and Kapodistrian University of Athens, School of Medicine, 17 Ag. Thoma Str. 11527, Athens,Greece
d Society of Junior Doctors, Surgery Workgroup, 75 Mikras Asias Str. 11527, Athens, Greece
e Department of Surgery, Duke University Medical Center, 2301 Erwin Rd, Durham, NC 27707, USA
Keywords:Xanthogranulomatous cholecystitis Surgical management Pathology Postoperative complications
ABSTRACT Background: Xanthogranulomatous cholecystitis (XGC) is a rare benign chronic inflammatory disease of the gallbladder that often presents as cholecystitis and most of the times requires surgical management.In addition,distinguishing XGC from gallbladder cancer preoperatively is still a challenge.The aim of the present systematic review was to outline the clinical presentation and surgical approach of XGC.Data sources: The present systematic review was designed using the PRISMA and AMSTAR guidelines.We searched MEDLINE,Scopus,Clinicaltrials.gov,EMBASE,Cochrane Central Register of Controlled Trials(CENTRAL) and Google Scholar databases from inception until June 2020.Results: The laparoscopic cholecystectomy rate (34%) was almost equal to the open cholecystectomy rate (47%) for XGC.An important conversion rate (35%) was observed as well.The XGC cases treated by surgery were associated with low mortality (0.3%),limited intraoperative blood loss (58-270 mL),low complication rates (2%–6%),along with extended operative time (82.6–120 minutes for laparoscopic and 59.6–240 minutes for open cholecystectomy) and hospital stay (3–9 days after laparoscopic and 8.3–18 days after open cholecystectomy).Intraoperative findings during cholecystectomies for XGC included empyema or Mirizzi syndrome.In addition,complex surgical procedures,like wedge hepatic resections and bile duct excision were required during operations for XGC.Conclusions: XGC seemed to be a rare,benign inflammatory disease that presents similar features as gallbladder cancer.The mortality and complication rates of XGC were low,despite the complex surgical procedures that might be required in some cases.
Introduction
Xanthogranulomatous cholecystitis (XGC) is a rare,benign,chronic inflammatory process of the gallbladder.It has been classified as an uncommon variant of chronic cholecystitis [1].The prevalence of XGC depends on the geographic location,ranging from 1.3% to 1.9% in Western societies like Europe and USA,while in India the reported prevalence reaches 9% [2].The clinical presentation is similar to acute cholecystitis with nausea,vomiting,right upper quadrant pain and positive Murphy’s sign.However,an indolent chronic course with symptoms of weight loss and anorexia could be possible.Laboratory findings are similar to those of acute cholecystitis,but ultrasound may show subjective signs like intramural hypoechoic nodules or bands in the gallbladder wall and a diffusely thickened gallbladder wall [3].CT and MRI show diffuse gallbladder wall thickening,intramural nodules and discontinuous enhancement of the mucosal line.Moreover,pericholecystic infiltration,transient hepatic attenuation difference at the gallbladder bed of the liver and luminal surface enhancement with contrast are some findings of radiological procedures [4].
Complications occur in approximately 30% of the patients with XGC,and most common complications are gallbladder perforation,bile duct obstruction,liver abscesses,and fistulas to the liver,duodenum or stomach [5].The treatment of XGC often requires open cholecystectomy due to the extensive fibrotic and inflammatory nature of the disease.However,laparoscopic approach should be initially attempted,as the conversion rate varies from 10%to 80% [6].Nevertheless,most complications,such as bile duct injury and bile fistula,are reported in laparoscopic operations [7].Despite the unique histopathological characteristics of XGC,distinguishing XGC from other clinical entities such as gallbladder carcinoma (GBC) is difficult,because the clinical presentation and radiologic features of this disease are non-specific [8].
The aim of the present systematic review was to summarize the surgical outcomes and postoperative complications after open and laparoscopic cholecystectomy for XGC;the secondary aim was to collect existing evidence on radiological and perioperative features that could suggest the diagnosis of XGC preoperatively.
Search strategies and selective criteria
The present study was designed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)and A Measurement Tool to Assess systematic Reviews (AMSTAR)guidelines [ 9,10 ].
Information sources and search methods
We searched MEDLINE,Scopus,Clinicaltrials.gov,EMBASE,Cochrane Central Register of Controlled Trials (CENTRAL) and Google Scholar databases.The date of our last search was June 20th,2020.“Snow-balling”was also performed by searching the references of articles that were retrieved in full-text to minimize the possibility of missing articles eligible for our study.The search strategy included the keywords“xanthogranulomatous”,“cholecystitis”in combination with Boolean operators (AND,OR,NOT).The stages of article selection are depicted in the PRISMA flow diagram(Fig.1).
The studies were selected in three consecutive stages.Firstly,after checking for duplicate publications,the titles and abstracts of all electronic articles were screened to evaluate their eligibility.Secondly,the articles that were presumed to meet the criteria were retrieved as full texts.In the third stage,we selected all observational studies (both prospective and retrospective) that met the inclusion criteria.Two authors (Frountzas M and Liatsou E)performed the electronic search of articles and tabulated data on duplicated pre-structured forms.The data were then reviewed and all disagreements were resolved by consensus.
Types of studies and patients
No language or date restrictions were applied during medical literature search.All articles that were written in Latin alphabet were considered as potentially eligible for inclusion.In addition,articles written in languages that use symbols such as Spanish were considered eligible,when they could be translated into plain English text using the Google translate service.All observational studies (both prospective and retrospective) that presented the diagnostic process,the surgical managements,and postoperative outcomes of XGC were included in this study.Studies that outlined the differences between several radiologic modalities such as ultrasound (US),computed tomography (CT) and magnetic resonance imaging (MRI) in diagnosing XGC before surgery were excluded.In addition,case reports,experimental animal studies and reviews were excluded.
Investigated outcomes
The primary outcomes of the present systematic review included the surgical outcomes (i.e.operative time,blood loss,hospital stay,mortality) and the postoperative complications (i.e.wound infection,bile fistula,bile leakage,hemoperitoneum,bile tract lesion,residual choledocholithiasis) after open and laparoscopic surgery for the management of XGC.All percentages of primary outcomes used the total number of patients from the studies that provided data about the outcome of interest as a denominator.
The radiological findings identified preoperatively were set as secondary outcomes.In addition,secondary outcomes included the clinical presentation of XGC,the intraoperative findings during open or laparoscopic cholecystectomy and the intraoperative procedures during open cholecystectomy.All percentages about secondary outcomes used the total number of patients from the studies that provided data about the outcome of interest as a denominator.
Quality assessment
The methodological quality of the included studies was assessed with the Newcastle-Ottawa Scale [11].According to that scale,each study was judged on eight items,categorized into three groups:the selection of the study groups,the comparability of the groups,and the ascertainment of either the exposure or outcome of interest for case-control or cohort studies,respectively.Stars awarded for each quality item served as a quick visual assessment.
Results
Excluded and included studies
Ten studies were excluded:four reported the diagnostic values of different radiologic means,such as US,CT and MRI,in the preoperative differential diagnosis between XGC and GBC [ 4,12–14 ];two described data on the histopathologic classification of XGC [ 15,16 ];four presented the outcomes of fine needle aspiration (FNA) under US guidance in preoperative diagnosis of XGC [17–20].
The methodological quality of the included studies was listed in Table 1 [ 1,21–53 ].The present systematic review included thirtyfour studies (Table 2) that cumulatively analyzed 1273 patients diagnosed with XGC after laparoscopic or open cholecystectomy.Patients’ characteristics were similar among the included studies (Table S1).
Primary outcomes
Among 999 patients with data provided in the included studies,341 (34%) were diagnosed with XGC after laparoscopic cholecystectomy,while 474 of 999 (47%) patients with available data,underwent open cholecystectomy.Among 525 patients,in which a laparoscopic cholecystectomy was initially attempted,184 (35%)were converted to open cholecystectomy (Table 3).
Houston et al.[23]reported that two patients died during the postoperative period.One patient died due to small bowel ischemia after superior mesenteric artery infarction and the other due to sepsis and multi-organ failure (Table 3).
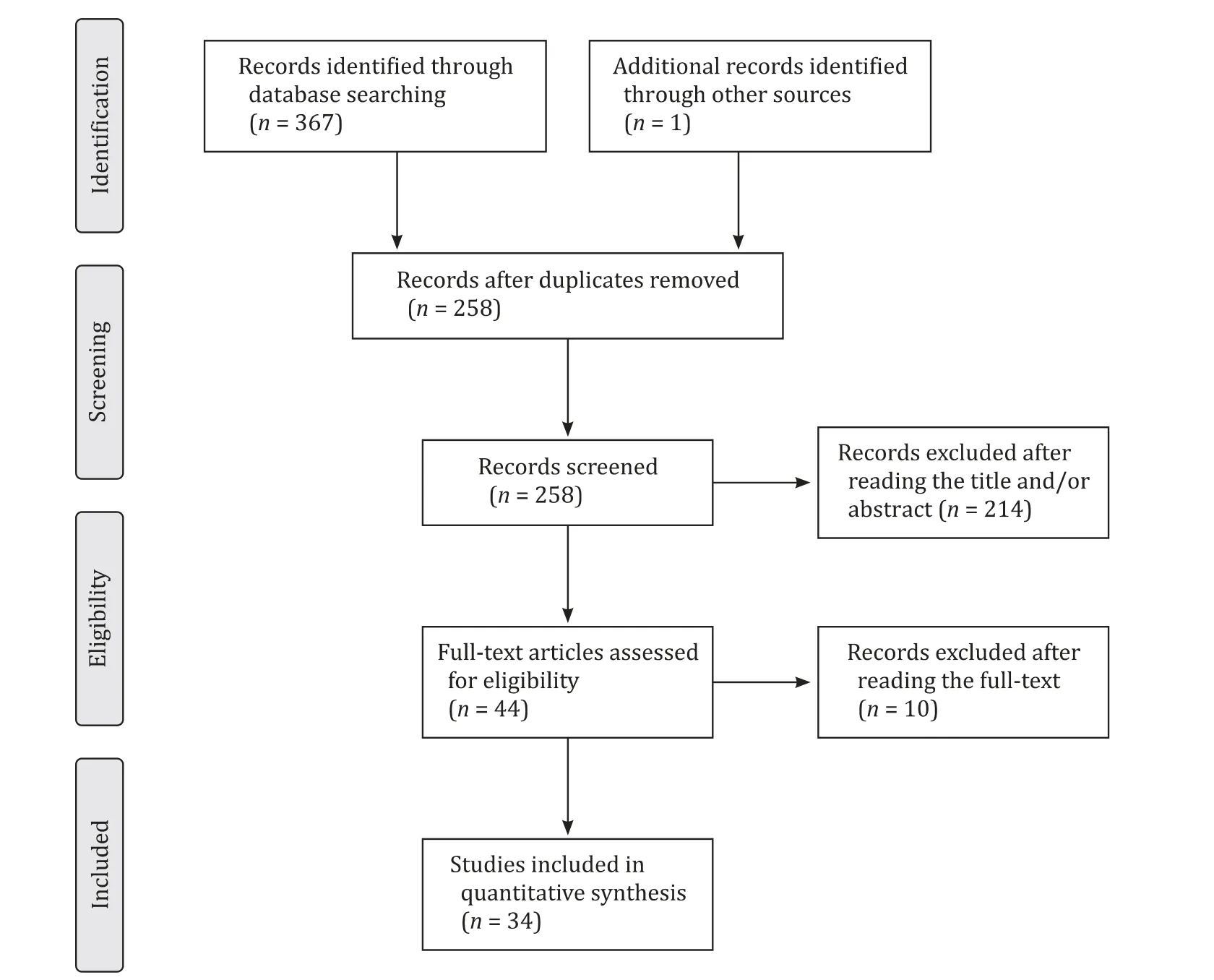
Fig.1.The PRISMA flowchart of study selection.
Kwon et al.[27]reported the longest operative time for laparoscopic cholecystectomy,with a median of 120 minutes (range:60–230 minutes).Median time interval for open cholecystectomy was 240 minutes (range:180–270 minutes).Srinivas et al.[30]demonstrated the shortest mean operative time for laparoscopic cholecystectomy,which was 82.6 minutes.Mean time interval for open cholecystectomy was 59.6 minutes.The shortest mean operative time for cholecystectomies converted from laparoscopic to open cholecystectomy was 97.9 minutes.The longest mean operative time for the cholecystectomies converted from laparoscopic to open was 154 minutes [46].The median blood loss during open or laparoscopic cholecystectomy for XGC was 270.1 mL (range:20–1500 mL) according to Park et al.[51],while Takeda et al.[53]reported the blood loss to be 58 ± 85 mL (Table 3).
Kwon et al.[27]reported the longest median hospital stay for patients that had undergone a laparoscopic cholecystectomy,which was 9 days (range:7–12 days),while median hospital stay after open cholecystectomy was 18 days (range:15–40 days).Qasaimeh et al.[46]reported the shortest mean hospital stay for laparoscopic cholecystectomy (3 days) and open cholecystectomy (8.3 days).In addition,they described the longest mean hospital stay,which was 7.2 days,after laparoscopic cholecystectomy that was converted to open.On the other hand,Srinivas et al.[30]showed the shortest mean hospital stay,which was 6.8 days,after conversion from laparoscopic to open cholecystectomy (Table 3).
According to the number of patients available in the included studies,6% (56/964) patients presented wound infection after surgery.Eleven out of 439 patients demonstrated bile fistula,while 17/655 (3%) patients had bile leakage or biliperitoneum.Furthermore,9/491 (2%) patients had bile tract lesions and 5/294 (2%) patients presented residual choledocholithiasis (Table 4).
Secondary outcomes
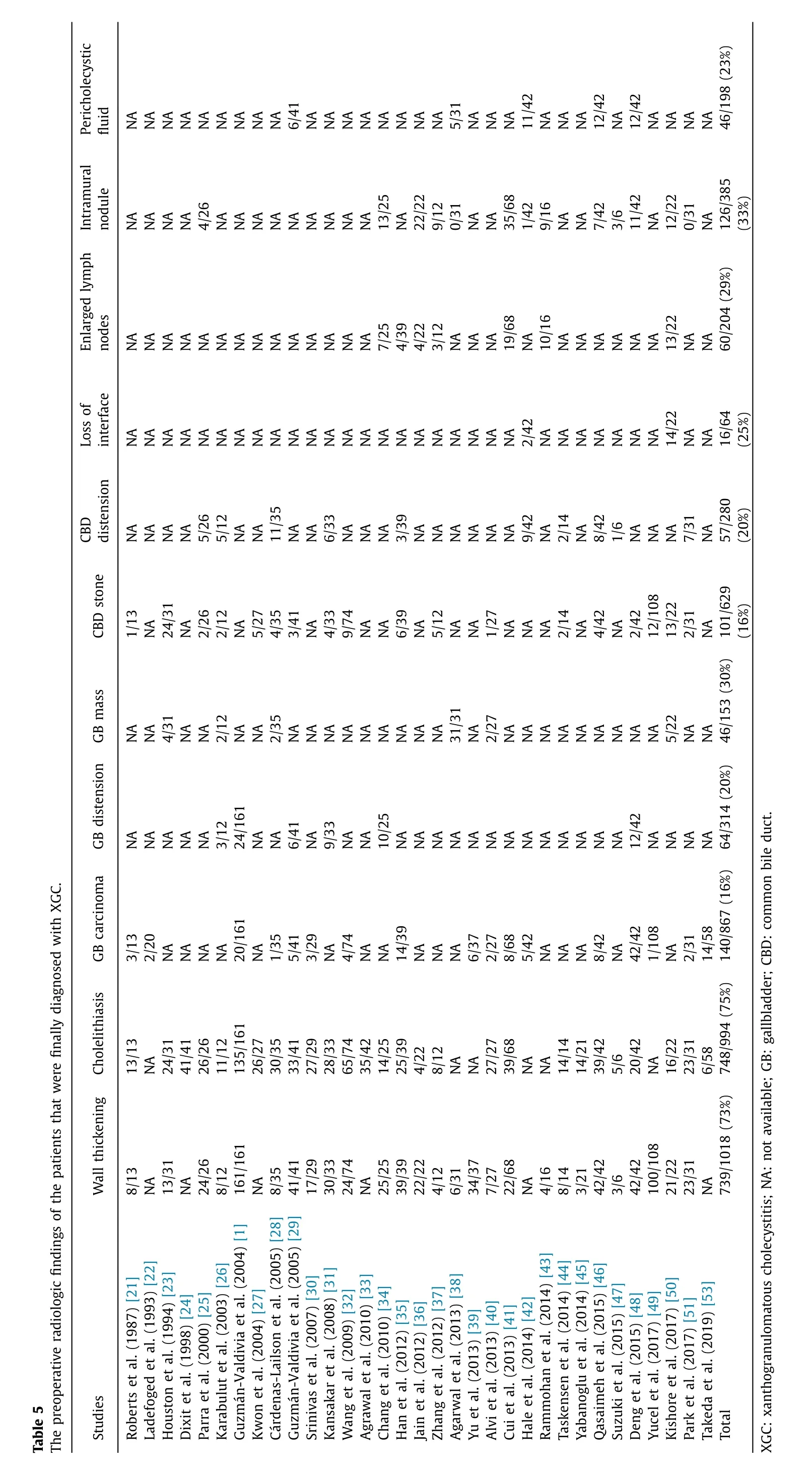
Gallbladder wall thickening was present in 739/1018 patients(73%) at radiologic examinations before surgery.748/994 patients(75%) presented cholelithiasis on imaging procedures.On the other hand,140/867 patients (16%) that were diagnosed with XGC after cholecystectomy,presented radiologic features that raised suspicion for GBC preoperatively.In addition,a gallbladder distension was found preoperatively in 64/314 patients (20%) and a gallbladder mass was demonstrated during the preoperative radiologic examinations in 46/153 patients (30%).Choledocholithiasis was present in 101/629 patients (16%),and the common bile duct(CBD) was dilated in 57/280 patients (20%),preoperatively.The loss of interface between the gallbladder and the liver bed was observed in 16/64 patients (25%).In 60/204 patients (29%),enlarged lymph nodes were identified,while 126/385 patients (33%) presented intramural nodules in gallbladder and 46/198 patients (23%)had pericholecystic fluid (Table 5).
261/651 patients (40%) were diagnosed with acute cholecystitis,339/466 patients (73%) with chronic cholecystitis,22/460 patients (5%) with cholangitis and 15/298 patients (5%) with pancreatitis.In addition,753/951 patients (79%) had pain,70/241 patients(29%) had anorexia,82/267 patients (31%) presented with nausea,98/300 patients (33%) experienced vomiting and 26/167 patients(16%) complained about recent weight loss.210/875 patients (24%)had jaundice,136/629 patients (22%) had fever,94/670 patients(14%) had a palpable mass and 34/181 patients (19%) had positive Murphy’s sign (Table S2).
Preoperative carcinoembryonic antigen (CEA) levels were reported in four studies and the mean CEA level ranged from 1.9 to 9.1 ng/mL.On the other hand,carbohydrate antigen 19-9 (CA19-9)levels were reported in five studies and the reported mean value ranged from 49.7 to 453 U/mL (Table S3).
Radical cholecystectomy was performed in 324/724 patients(45%).On the other hand,frozen section pathology was utilized in 219/556 patients (39%) during open cholecystectomy in order to rule out the possibility of GBC.Wedge hepatic resection wasperformed in 22/316 patients (7%),and 10/76 patients (13%) underwent lymph node dissection.Furthermore,in 52/291 patients(18%) a T-tube drainage was necessary,while in 23/340 (7%) patients a bile fistula repair was performed.Finally,an extrahepatic bile duct excision was performed during open cholecystectomy in 22/189 patients (12%) (Table S4).
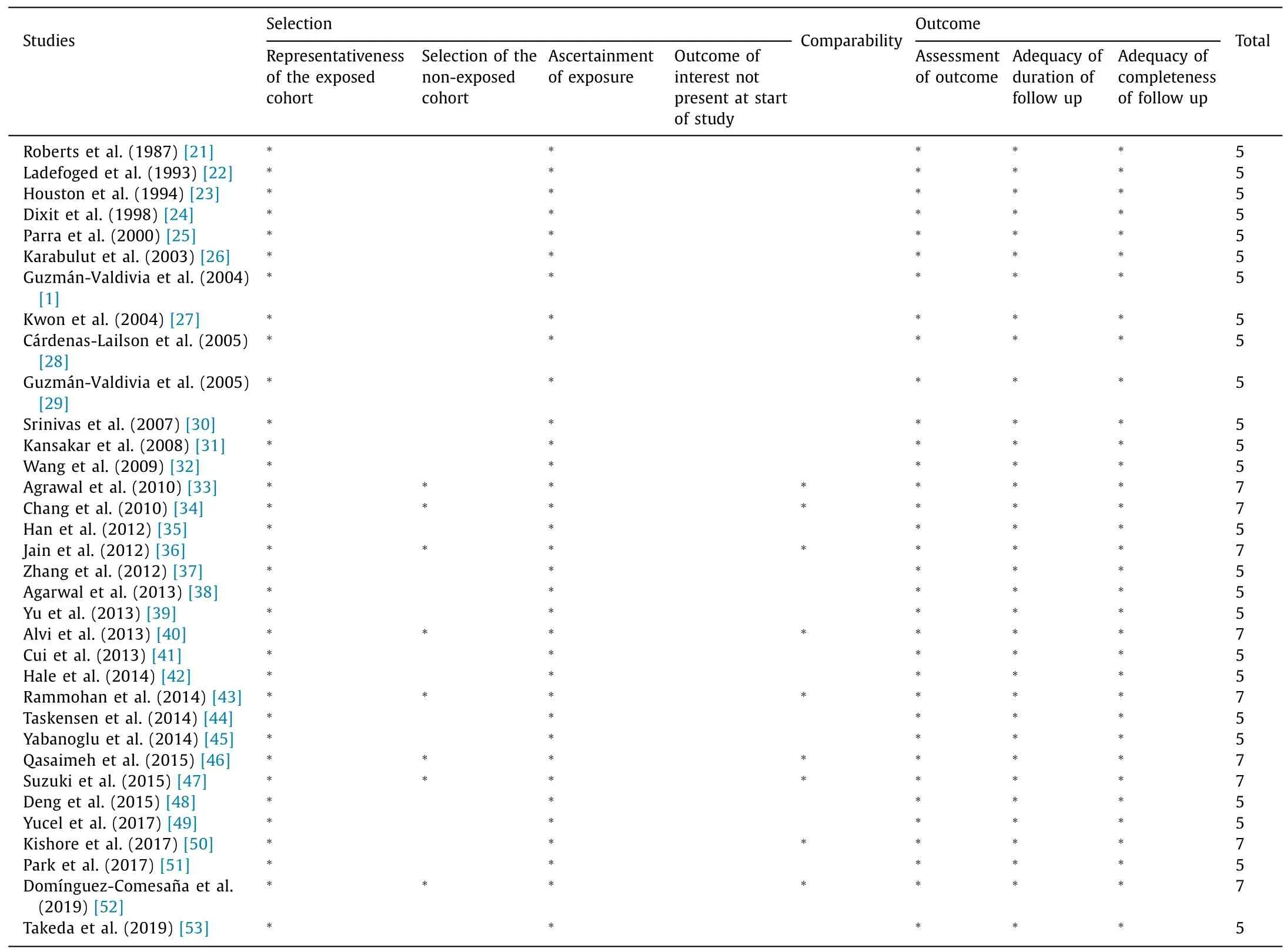
Table 1 Methodological assessment of the included studies according to the Newcastle-Ottawa Scale.
An empyema was encountered in 42/117 patients (36%) during cholecystectomy,while gallstones were found in 274/408 patients(67%).Mirizzi syndrome was demonstrated during laparoscopic or open cholecystectomy due to XGC in 26/464 patients (6%).In 151/365 patients (41%),adhesions were found during cholecystectomy,while obscure Calot’s triad anatomy was found in 27/97 patients (28%).Finally,17/93 patients (18%) had gangrenous cholecystitis as outlined intraoperatively (Table S5).
XGC pathology
The histological diagnosis of XGC was based on pathological analysis of the resected specimens after cholecystectomy.XGC is a rare variant of chronic cholecystitis.The hallmark of this entity is the intramural accumulation of lipid-laden macrophages and acute and chronic inflammatory cells.XGC is characterized macroscopically by greyish-yellow nodules or streaks in the gallbladder wall,which are mainly caused by lipid laden macrophages.In addition,histological diagnosis is based on diffuse or focal mural changes in the form of nodules of xanthoma cells (foamy histiocytes containing lipids and bile pigment),giant multinucleate histiocytes and acute or chronic inflammatory cells.These histiocytes are positive for CD68 on immunohistochemistry.Confined perforations of gallbladder wall and extension of inflammation lead to adhesions with the adjacent liver,duodenum and transverse colon,which could easily be mistaken for GBC [30].
Discussion
The present systematic review summarized the clinical management of XGC,the surgical approach of XGC,along with the postoperative outcomes and complications after cholecystectomy.Cholecystectomy for XGC is a technically difficult procedure.The similar number of laparoscopic and open cholecystectomies and the significant conversion rate from laparoscopic to open cholecystectomy support this finding.On the other hand,cholecystectomy for XGC was associated with low mortality,limited intraoperative blood loss,low complication rates,along with moderate operative time and hospital stay.The diagnostic process of XGC remained a challenge,mainly due to the similar clinical presentation and laboratory findings,as most of the diseases cause a biliary colic,such as acute cholecystitis or choledocholithiasis.However,a lot of patients presented special radiologic signs in preoperative US or MRI,such as loss of interface between gallbladder and liver bed.Finally,com-plicated findings like empyemas and Mirizzi syndrome,have been observed during cholecystectomies for XGC.Also,complex surgical procedures like wedge hepatic resections and bile fistulas repairs,were required in the setting of cholecystectomy for XGC.
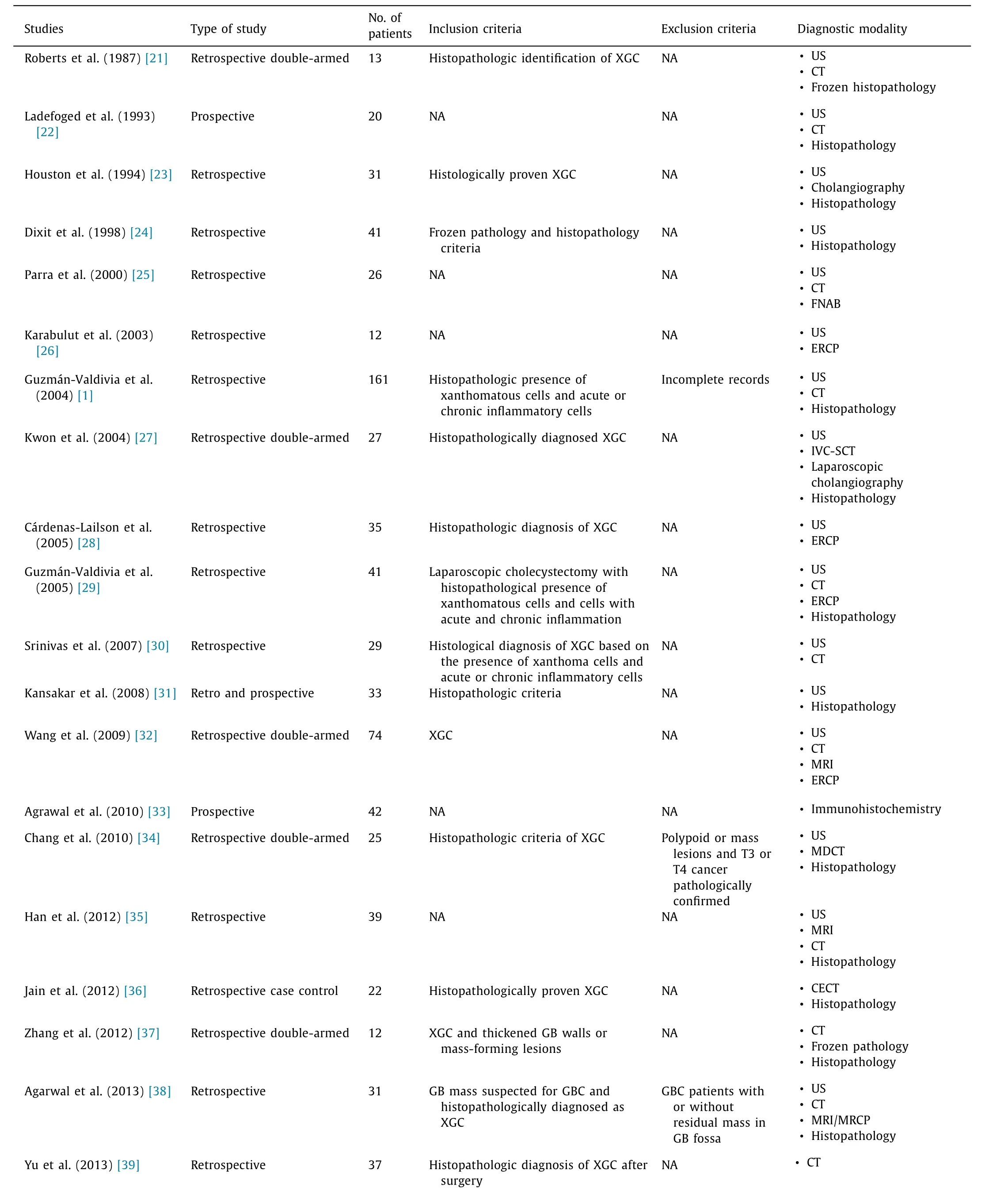
Table 2 The characteristics of the studies that were included in the present systematic review.
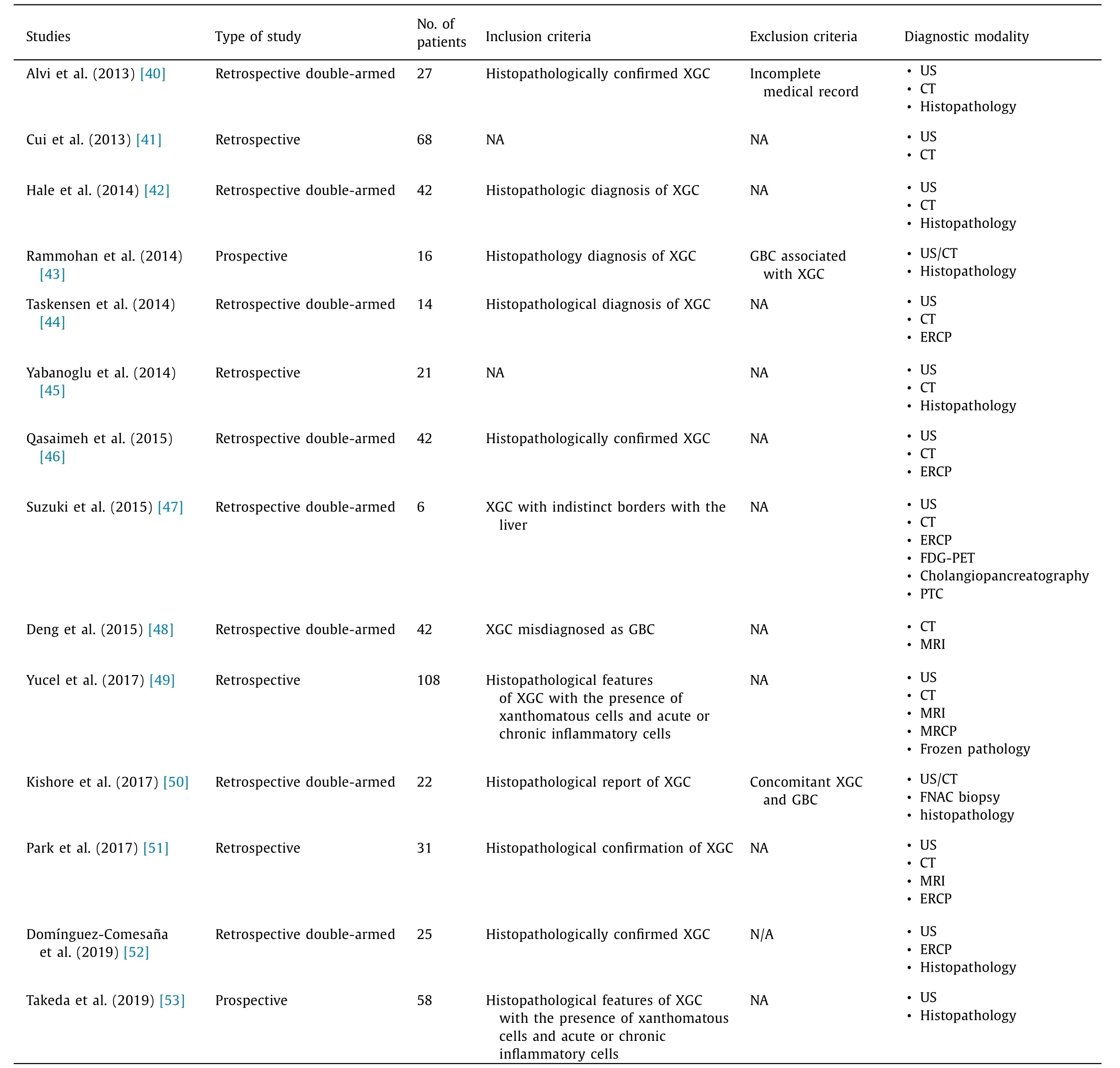
Table 2 (continued)
Cholecystectomy for XGC has similar surgical outcomes with cholecystectomy for acute cholecystitis.Rice et al.[54]demonstrated that the complication rate after delayed or elective cholecystectomy due to acute cholecystitis was 7.4%.The mortality was 0.6%,similar to the findings of the present systematic review.Moreover,the complication rate for non-elective cholecystectomies was 9.8% and the median length of hospital stay was 4 days (range:3-6 days) [55].Finally,laparoscopic cholecystectomy due to acute cholecystitis is related to shorter operative time and shorter hospital stay compared to those of open cholecystectomy [56].The present systematic review demonstrated similar outcomes for laparoscopic cholecystectomy for XGC.
Nevertheless,distinguishing XGC from GBC remains an important clinical issue.There are no specific radiological findings for the two entities,except from discontinuous mucosal lining,diffuse wall thickening and intramural nodules that suggest XGC,but these findings are only present in about 25% of cases.XGC is a rare form of chronic cholecystitis accompanied by a focalor diffuse destructive inflammatory process,with varying proportions of fibrous tissue,acute and chronic inflammatory cells and accumulation of lipid-laden macrophages in areas of inflammation [57].Several chronic inflammatory conditions of the gastrointestinal tract have been correlated to malignant transformation,such as ulcerative colitis or Barrett’s esophagus;however,a pathogenetic link between XGC and GBC has not yet been proven [ 1,58 ].There are some theories that both XGC and GBC are late complications of chronic cholelithiasis and cholecystitis.In addition,it has been supposed that GBC causes bile infiltration through the gallbladder wall and that the chronic inflammatory process is exacerbated [59].In fact,an association between XGC and GBC has been observed in 0.2%-12.5% of cases as described in a few case series [ 23,24,60 ].
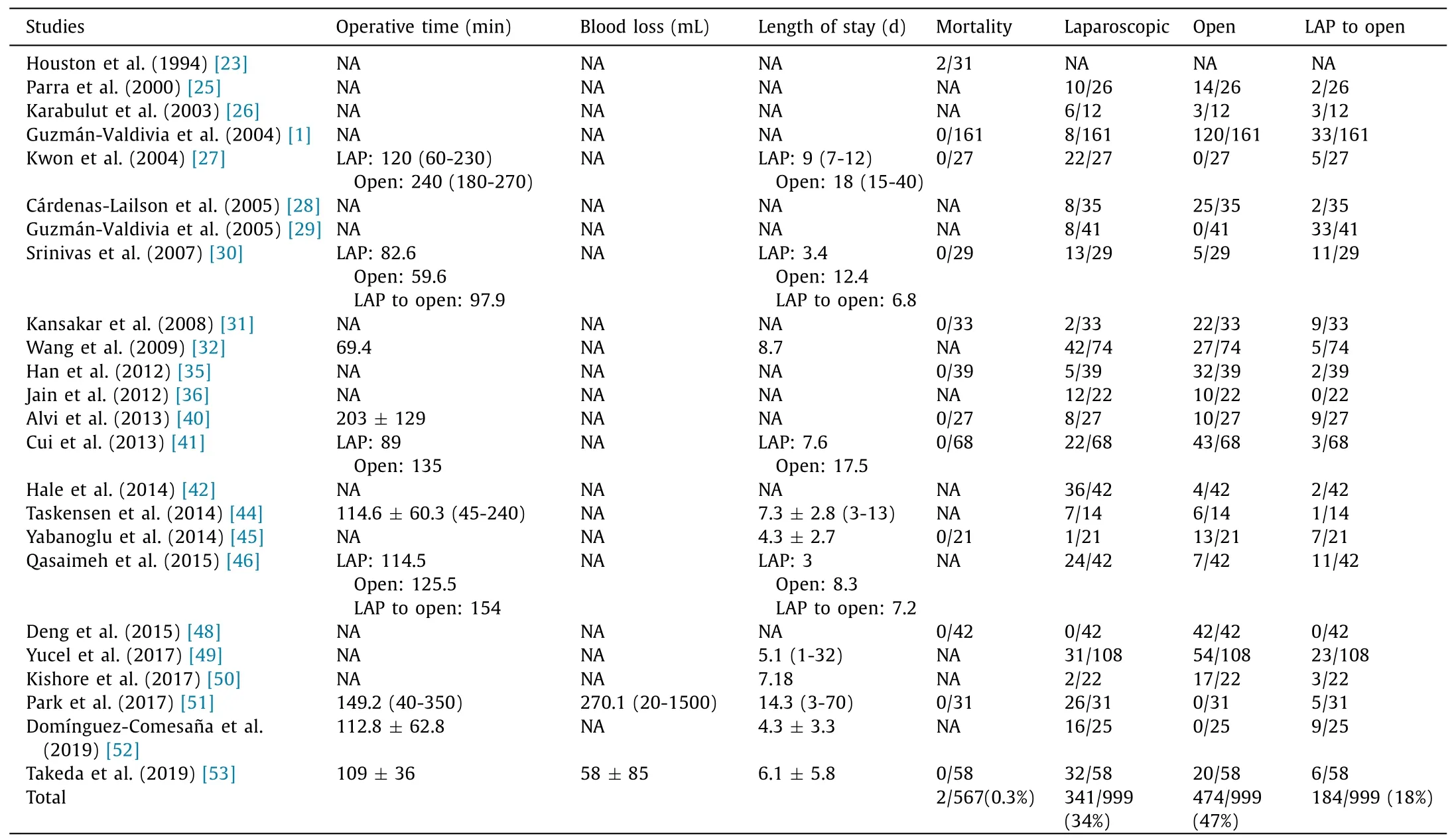
Table 3 The surgical outcomes after cholecystectomy of the patients that were finally diagnosed with XGC.
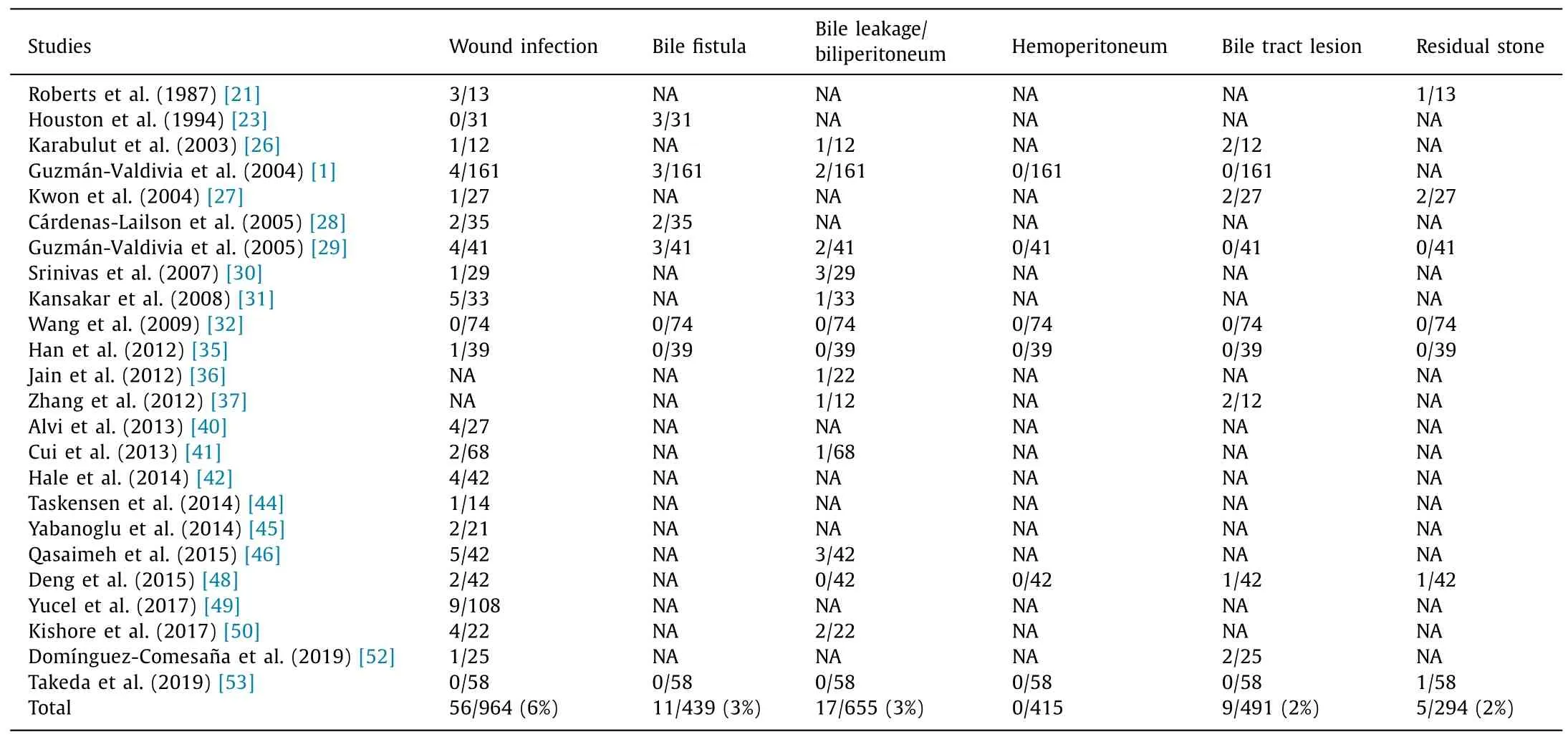
Table 4 The postoperative complications after cholecystectomy of the patients that were finally diagnosed with XGC.
The underlying pathophysiological mechanisms of XGC have not been completely understood.One theory refers to the rupture of Rokitansky-Aschoff sinuses due to increased intraluminal pressure and intramural extravasation of bile with subsequent xanthogranulomatous reaction [60].Another theory includes the important role of gallstones,which cause obstruction and stasis in the gallbladder leading to chronic inflammation and mucosal ulceration,that also results in extravasation of bile into the gallbladder wall [24].Nevertheless,although its pathogenesis is not clear,XGC is characterized by a focal or diffuse destructive inflammatory process,with accumulation of lipid laden macrophages,fibrous tissue,and acute and chronic inflammatory cells.
The focal or diffuse pattern seems to represent a histopathologic spectrum,which is associated with differences in incidence,presentation and treatment.Firstly,the incidence of early focal XGC in patients with symptomatic gallbladder disease ranges widely depending on geographical region,studied population,and cohort size,and can be found,on average,in 1.3% of patients with cholecystectomy in Europe,1.5% in America,1.9% in Japan and Korea,and over 9% in India.On the other hand,severe diffuse and tumor-like variant of XGC with extensive inflammatory fibrosis,affecting the surrounding tissues and organs,is rare,with only a few cases published in the literature [61].In addition,the presentation of patients with focal and less severe XGC is usually similar to that of chronic or acute cholecystitis,including postprandial right upper quadrant abdominal pain with or without positive Murphy’s sign,fever,nausea,and vomiting.On the contrary,the presentation of diffuse and tumor-like XGC with severe inflammatory fibrosis,involving the surrounding tissues,may also include right upper quadrant mass,abdominal tenderness unrelated to meals,jaundice with or without cholangitis,and weight loss that makes XGC indistinguishable from GBC [62].
To our knowledge,the present review was the first that systematically presented all available studies related to the clinical management and surgical approach of XGC.It also summarized the overall surgical outcomes along with the complications.In addition,our study was based on a meticulous review of a wide range of databases.The search strategy was not restricted by language and date criteria;hence,limiting the possibility of missing eligible articles that could significantly alter the findings of the systematic review.However,the small number of patients in the included studies rendered their results rather inconclusive in the majority of cases.Moreover,the differences in methodological strategy of studied population,raised the level of heterogeneity among included studies.Finally,XGC is a condition that could only be diagnosed histopathologically after cholecystectomy.Therefore,there were no case-control studies available in the literature that might compare surgical outcomes and complications between open and laparoscopic or laparoscopic and converted cholecystectomy for XGC.The high level of heterogeneity among the included studies and the lack of comparison between laparoscopic and open cholecystectomy for XGC did not allow the conduction of a meta-analysis.
Preoperative diagnosis remains the greatest challenge for surgeons in order to form the best curative plan and avoid useless extensive operations.However,specific radiologic diagnostic signs,such as discontinuous mucosal lining,diffuse wall thickening and intramural nodules,could not definitely distinguish XGC from GBC [14].Moreover,XGC and GBC often share similar clinical,biochemical and intraoperative features.The possibility of coexistence of these two diseases has been reported between 0%and 13% [57].Serum CA19-9 is not helpful in the differential diagnosis,because it is usually elevated in both conditions.All these factors may lead to over or undertreatment in some cases.
In addition,several biomarkers that could be detected by immunochemistry on FNA or surgical specimens,have been supposed to facilitate differential diagnosis between XGC and GBC.Thep53mutation is more frequent in GBC than that in XGC (52% vs.3%).Moreover,proliferating cell nuclear antigen expression is more frequent in GBC than that in XGC (65% vs.11%).Beta-catenin is expressed in both GBC and XGC,but the expression pattern in XGC is homogenously membranous,whereas in GBC the expression pattern is cytoplasmic and nuclear [58].Furthermore,B and T lymphocyte attenuator (BTLA) and anergy cell marker Casitas-B-lineage lymphoma protein-b (Cbl-b) seem to play a role in histological differential diagnosis between XGC and GBC.The density of infiltrating T cells is higher in XGC than that in GBC.The density ratio of BTLA+cells to CD8+T cells (BTLA/CD8) and that of Cbl-b+cells to CD8+T cells (Cbl-b/CD8) are significantly higher in GBC than those in XGC [63].
Nevertheless,definite preoperative diagnostic means,such as FNA under US guidance,did not offer any advantage in distinguishing XGC from GBC [64].Therefore,the surgical plan is a multifactorial process depending on patient-related,disease-related,and procedure-related factors,which must be taken into account and discussed in detail with the patient.Focal or diffuse uncomplicated XGC,even when a synchronous stage 0-I GBC is present,can be treated with simple laparoscopic cholecystectomy [65].On the other hand,the poor prognosis of GBC (5-year survival about 50%)suggests wide surgical excisions,when there is a doubt in preoperative examinations,in order to avoid the possible complications of a second operation [66].Radical cholecystectomy with anenblocresection of the involved adjacent organs,such as the liver,duodenum,pancreas,colon,omentum and extrahepatic bile ducts,is advocated for GBC stage II to IVa and may be warranted in some cases of aggressive,mass-like XGC inseparable from the surrounding tissues or in which GBC cannot be excluded [67].
Conclusion
XGC is a rare benign type of cholecystitis that is often difficult to be distinguished from GBC.However,due to the poor prognosis of GBC,any preoperative suspicion in diagnosis should lead to wide surgical excisions,just like in GBC.For XGC treatment,laparoscopic and open cholecystectomy rates are almost similar and an important conversion rate from laparoscopic to open cholecystectomy has been observed.Surgical management of XGC might require complex procedures,for which surgeons should be prepared.When surgeons face XGC,they should keep in mind that it is a benign disease with low mortality and complication rates,despite the possible intraoperative difficulties.
Acknowledgments
None.
CRediT authorship contribution statement
Maximos Frountzas:Data curation,Formal analysis,Writing -original draft.Dimitrios Schizas:Conceptualization,Data curation,Writing -review &editing.Efstathia Liatsou:Methodology,Validation,Writing -original draft.Konstantinos P Economopoulos:Methodology,Project administration.Christina Nikolaou:Data curation,Writing -original draft.Konstantinos G Apostolou:Formal analysis,Validation,Writing -original draft.Konstantinos G Toutouzas:Conceptualization,Writing -review &editing.Evangelos Felekouras:Project administration,Supervision.
Funding
None.
Ethical approval
Not needed.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Supplementary materials
Supplementary material associated with this article can be found,in the online version,at doi:10.1016/j.hbpd.2021.01.002 .
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Practice of precision surgery in primary liver cancer
- Reporting of longitudinal pancreatojejunostomy with partial pancreatic head resection (the Frey procedure) for chronic pancreatitis:A systematic review
- Hepatobiliary&Pancreatic Diseases International
- Transjugular intrahepatic portosystemic shunt is effective in patients with chronic portal vein thrombosis and variceal bleeding
- Long-term follow-up of HCV patients with sustained virological response after treatment with pegylated interferon plus ribavirin
- Laparoscopic hepatectomy is superior to open procedures for hepatic hemangioma