Clinical efficacy of direct-acting antiviral therapy for recurrent hepatitis C virus infection after liver transplantation in patients with hepatocellular carcinoma
2021-01-13MohamedSalehIsmailManalHassanSairaAijazKhaderiWaelAhmedYousryMahaMohsenKamalElDinMohamedMohamedBahaaElDinOsamaAboelfotohElSayedAhmedOmarKasebJohnAlanGossFasihaKanwalPrasunKumarJalal
Mohamed Saleh Ismail, Manal Hassan, Saira Aijaz Khaderi, Wael Ahmed Yousry, Maha Mohsen Kamal El-Din, Mohamed Mohamed Bahaa El-Din, Osama Aboelfotoh El Sayed, Ahmed Omar Kaseb, John Alan Goss, Fasiha Kanwal, Prasun Kumar Jalal
Mohamed Saleh Ismail, Manal Hassan, Saira Aijaz Khaderi, Fasiha Kanwal, Prasun Kumar Jalal, Division of Gastroenterology, Baylor College of Medicine, Houston, TX 77030, United States
Mohamed Saleh Ismail, Wael Ahmed Yousry, Maha Mohsen Kamal El-Din, Osama Aboelfotoh El Sayed, Department of Internal medicine, Gastroenterology and Hepatology, Ain Shams University, Cairo 11566, Egypt
Mohamed Saleh Ismail, Saira Aijaz Khaderi, John Alan Goss, Prasun Kumar Jalal, Department of Surgery, Division of Abdominal Transplantation, Baylor College of Medicine, Houston, TX 77030, United States
Manal Hassan, Department of Epidemiology, the University of Texas MD Anderson Cancer Center, Houston, TX 77030, United States
Mohamed Mohamed Bahaa El-Din, Department of Surgery, Ain Shams University, Cairo 11566, Egypt
Ahmed Omar Kaseb, Department of Gastrointestinal Medical Oncology, the University of Texas MD Anderson Cancer Center, Houston, TX 77030, United States
Abstract
Key Words: Direct-acting antiviral; Liver transplant; Hepatocellular carcinoma; Recurrence
INTRODUCTION
Hepatitis C virus (HCV) infection is the leading indication for liver transplantation[1].Recurrent HCV infection of transplanted liver allografts is universal in patients with detectable HCV viremia at the time of transplantation[2].Evidence of recurrent HCV infection of an allograft occurs as early as 4 wk after transplantation, with development of hepatitis within 6-12 mo in 70%-90% of HCV-infected liver transplant (LT) recipients[3,4].Furthermore, allograft cirrhosis with a poor outcome occurs within 5 years after transplantation in 20%-30% of these patients[5].
Direct-acting antiviral (DAA) therapy has been adopted as the standard of care for recurrent HCV infection after transplantation[6].Patients with sustained virologic responses to antiviral therapy may experience fibrosis regression and reduced mortality rates[7,8].In pre-transplant studies, there are conflicting data regarding the impact of DAA treatment on de-novo or recurrent hepatocellular carcinoma (HCC) in HCV-infected patients[9-12].
Researchers have investigated the safety and efficacy of DAA treatment in LT recipients[13-15].However, the efficacy in LT recipients with a history of HCC has not been investigated.Moreover, there are no data regarding HCC recurrence in LT recipients following DAA therapy, especially patients who experienced treatment failure.Little is known about predictors of DAA treatment response after LT for HCC.Therefore, we performed this study to (1) Highlight the efficacy and safety of DAA therapy in LT recipients with HCV infections and history of HCC; and (2) Investigate the impact of DAA use on post-transplantation HCC recurrence.
MATERIALS AND METHODS
Study design
A total of 106 LT recipients given DAAs for recurrent HCV infection from January 1, 2015, to March 1, 2019, at Baylor College of Medicine were retrospectively identified.
Criteria for study inclusion were (1) Age of 18 years or older; (2) History of liver transplantation; (3) Positive anti-HCV and HCV ribonucleic acid prior to and after transplantation; and (4) Treatment with an oral DAA regimen with or without ribavirin.We excluded (1) Patients with active hepatitis B virus (HBV) infection evident by positive hepatitis B surface antigens or HBV deoxyribonucleic acid; (2) Patients with human immunodeficiency virus infection; and (3) Any other metabolic, viral or genetic causes of chronic liver disease.Patients were classified into two groups: Those with pre-transplantation HCC (PHCC;n= 68) and those without pretransplantation HCC (PnHCC;n= 38).The initiation of DAA treatment and the regimen type and duration were determined by the treating transplant hepatologists.Demographic and clinical information for each participant were documented and stored in a secure database under a Baylor College of Medicine Institutional Review Board-approved protocol.All patients gave written informed consent for data collection prior to their LTs.
Patient information
Clinical data:The collected information included the following baseline characteristics: Age, sex, ethnicity, body mass index (BMI), medical history (comorbid conditions, stage of liver disease), adverse events, baseline (at time of DAA initiation) and on-treatment laboratory values obtained every 4 wk, including HCV ribonucleic acid levels, until the end of treatment (EOT) and at follow-up visits.BMI was calculated at treatment initiation, the EOT, and the last follow-up visit (normal BMI, < 25 kg/m2; overweight, 25-30 kg/m2; obese, > 30 kg/m2).
Laboratory data:The following laboratory test results were analyzed: Anti-HCV and HCV ribonucleic acid levels; HCV genotypes; Hepatitis B surface antigens; Antihepatitis B surface antibodies; Hepatitis B core antibodies; Anti-human immunodeficiency virus antibodies; Epstein-Barr virus, cyotmegalovirus, iron studies, ceruloplasmin, auto-antibodies, serum albumin, alkaline phosphatase, creatinine, sodium, alanine aminotransferase, and total bilirubin levels; Prothrombin time and international normalized ratio; Hemoglobin levels; and Platelet counts.Test results were analyzed to exclude other viral, metabolic, autoimmune causes of liver disease.Estimated glomerular filtration rates were calculated using the Modification of Diet in Renal Disease equation.The model for end-stage liver disease-sodium score was calculated using serum bilirubin, creatinine, and sodium levels and the international normalized ratio.
Clinical efficacy:Treatment efficacy was demonstrated by sustained virologic response at follow-up week 12, defined as an undetectable HCV ribonucleic acid level in the blood at week 12 after the EOT.Accordingly, patients were classified as having DAA responses or failures.
Clinical safety:Adverse events were defined as any events that required an HCV medication dose reduction or treatment discontinuation or the addition of a concomitant medication for management.Events of special interest in this study were HCC recurrence, HBV reactivation and acute allograft rejection.
Statistical Analysis
Stata software (Stata Corp, College Station, TX, United States) was used for statistical analysis.Descriptive statistics were employed, with Studentt-test and Mann-Whitney-Wilcoxon test statistics used to assess the significance of mean and median differences in continuous variables between study groups.The Pearsonχ2or Fisher exact test was used to test for differences in the distribution of categorical data between groups.To adjust for the small sample size, multivariate exact unconditional logistic regression analyses were performed.For each risk factor, the adjusted odds ratios and respective 95% confidence intervals were calculated.All odds ratios were adjusted for age, sex, and significant factors from univariate analysis.Pvalue less than 0.05 was defined as significant.
RESULTS
Baseline patient characteristics
Most patients in the PHCC and PnHCC groups were male and white (Table 1).The patients with PHCC were significantly older (P= 0.01), with a significantly more extensive past history of smoking than the patients with PnHCC (P< 0.01).Baseline comorbidities and cirrhosis were similar in both groups.However, diabetes mellitus was significantly higher in the PHCC group (P< 0.01).
HCV genotypes 1a and 1b were present in 50%, and 21% of the PHCC patients, respectively, and 66% and 21% of the PnHCC patients, respectively (P= 0.1).Although not statistically significant, more PHCC patients had HCV genotype 3a than PnHCC patients (22%vs11%;P= 0.1).The mean ± SD BMIs at DAA treatment initiation were comparable in the PHCC and PnHCC patients (28.5 ± 4.5 kg/m2vs27.9 ± 5.5 kg/m2;P= 0.6).
Pre-transplant relapse rate to antiviral treatment was higher in the PHCC patients than in the PnHCC patients (34%vs16%;P= 0.06).Although there was no statistically significant difference, more PHCC patients received HCV- or anti-HBc-positive allografts than PnHCC patients [6%vs0% (P= 0.3) and 15%vs3% (P= 0.09), respectively].
Table 1 shows significant variations in the mean and median laboratory and clinical values between the two groups.Baseline (at time of DAA initiation) laboratory values were similar in the PHCC and PnHCC patients except for the serum creatinine level, estimated glomerular filtration rate, and the model for end-stage liver disease-sodium score, which were markedly lower in the PHCC patients (Table 1).
Clinical efficacy
The median time from liver transplantation to DAA treatment initiation in the entire cohort was 34 mo (range, 1-331 mo), and the median follow-up duration after DAA treatment completion was 20 mo (range, 3-46 mo).The median time from liver transplantation to DAA treatment initiation in the PHCC patients was 28 mo (range, 1-171 mo) which is significantly shorter than in the PnHCC patients, 91.5 mo (range, 2.0-331.0 mo) (P< 0.0001).One hundred patients (94%) experienced sustained virologic response at follow-up week 12 (SVR12) (DAA response), whereas 6 patients (6%) did not (DAA failure).The median times from transplantation to DAA therapy initiation were 32.5 mo (range, 1.0-331.0 mo) in the DAA response group and 54.5 mo (range, 8.0-148.0 mo) in those who had DAA failure (P= 0.7).
All patients who did not experience SVR12 were non-cirrhotic.Two patients had relapses at follow-up week 12, three patients did so at follow-up week 4, and one patient suffered viral breakthrough at treatment week 12.
In the DAA response group, the rates of concordance between SVR12 and SVR at follow-up week 24, and between SVR12 and quantitative HCV polymerase chain reaction at the last follow-up visit were both 100%, as no patients had relapses after experiencing SVR12.
Figure 1 shows the numbers of patients who had responses to and failures of the 16 DAA regimens used in this study.We observed no significant variations in the treatment distribution between the PHCC and PnHCC groups (P= 0.3).The six patients who had DAA failures received five DAA regimens: (1) Sofosbuvir (SOF)/velpatasvir /voxilaprevir plus ribavirin (RBV) for 12 wk (n= 2); (2) SOF, daclatasvir, and RBV for 24 wk (n= 1); (3) SOF/ledipasvir for 24 wk (n= 1); (4) SOF/simeprevir for 12 wk (n= 1); and (5) Glecaprevir /pibrentasvir for 12 wk (n= 1).
Table 2 lists the univariate and multivariate odds ratios (ORs) and 95% confidence interval (CI) for potential predictors of post-LT DAA therapy failure.Univariate analysis showed a significant risk of failure (P< 0.05) in patients with HCV-positive allografts; HCV genotype 3a; high alanine aminotransferase (ALT) level > 35 U/L and or quantitative HCV polymerase chain reaction > 15 IU/mL at treatment week 4.However, multivariate analysis after adjustment for these predictors demonstrated a high ALT level > 35 U/L at treatment week 4 was significantly associated with DAA therapy failure (P= 0.04) after adjustment for the confounding effect of the significant factors described above.Pre-transplant relapse to DAA treatment and history of pretransplant HCC did not impact SVR12 rates in patients treated with DAA post-LT.

Table 1 Characteristics of the study population according to pre-transplantation hepatocellular carcinoma status
We observed normalization of ALT levels ≤ 35 U/L at treatment week 4 in 85% of the patients (Figure 2 and Table 3).Moreover, the mean platelet count in all patients improved significantly over the follow-up period with a mean difference of -36 (-47.9 to -6),P< 0.001 (Figure 3 and Table 4).
HCC recurrence after DAA treatment
In the PHCC group, six patients (9%) experienced HCC recurrence after DAA treatment initiation.The median time from DAA therapy initiation to HCC recurrence was 8.5 mo (range, 1.0-29.0 mo).
The demographic characteristics, HCC risk factors, and clinical features were similar in the patients who had HCC recurrences after DAA treatment (n= 6) and those who did not (n= 62), demonstrating a lack of a significant impact of these factors on prediction of recurrence after the treatment (Table 5).Of the patients who experienced HCC recurrence after DAA treatment, 5 patients (83%) had relapses to pre-transplant DAA treatment, suggesting pre-transplant relapse is a predictor of post-transplant HCC recurrence.The estimated adjusted OR was 14.9 (95%CI: 1.1-219.3).
In addition, we identified relapse to the post-transplantation DAA therapy as a potential predictor of HCC recurrence (P= 0.05), with a 10-fold greater risk of recurrence in patients who had treatment failures than in responders.The estimated adjusted OR was 10.6 (95%CI: 1.0-121.6) (Table 5).
RBV-containing regimens
We also categorized patients into two groups according to use of RBV (Table 6).Demographic characteristics and baseline laboratory values were similar for patients given DAA therapy with and without RBV except for the serum creatinine and hemoglobin levels, the model for end-stage liver disease-sodium score, estimated glomerular filtration rate, and presence of chronic kidney disease.
Patients who received DAA regimens with and without RBV had similar SVR12 rates (95.5%vs92.1%;P= 0.7).
BMI and DAA therapy
A high baseline BMI (≥ 25 kg/m2) did not have a more significant impact on SVR12 or HCC recurrence after DAA treatment than a low BMI (< 25 kg/m2) (Tables 2 and 5).However, among those with PHCC, weight loss by the end of DAA treatment was a significant predictor of HCC recurrence (P= 0.03).
Safety and tolerability
Only one patient in the PnHCC group had to discontinue DAA treatment SOF/ ledipasvir at 16 weeks due to adverse events, which consisted of significant fatigue and headache, but achieved SVR12.However, of the patients receiving RBVcontaining DAA regimens, 26 (38%) needed RBV discontinuation or dose modification due to adverse events, including anemia, fatigue, nausea, and elevated serum creatinine level.
No patients experienced decompensation during or after DAA treatment until the last follow-up visit.Also, none of anti-HBc-positive patients (30%) experienced HBV reactivation during or after DAA therapy until the last follow-up visit.
Physicians administered tacrolimus-containing regimens to 83% of the patients during DAA therapy.We found no significant changes in immunosuppressive drug dosages or levels during DAA treatment.Five patients (5%) experienced mild acute rejection episodes within a median time of 11 mo (range, 5-28 mo) after DAA treatment completion, all of whom experienced SVR12 and rejection episodes were controlled.
DISCUSSION
The present study is the first to demonstrate that pre-transplant relapse to DAA therapy is a significant predictor of post-transplant HCC recurrence.Post-LT DAA therapy relapse is also associated with HCC recurrence in LT recipients.High ALT level > 35 U/L at treatment week 4 is a predictor of DAA treatment failure.
All oral DAA treatments were recently adopted as the standard of care for treatment of recurrent HCV infection in LT recipients.However, contradictory data regarding the increased risk of HCC recurrence in pre-transplant patients after DAA therapy, and HCC influence on DAA SVR rates may affect the decision to treat unique populations of patients as LT recipients with past histories of HCC.

Table 2 Risk factors for post-liver transplant direct-acting antiviral therapy response (Logistic regression analysis)

Table 3 mean (± SD) alanine aminotransferase levels in patients who had direct-acting antiviral therapy responses and failure (baseline, week 4, week 8, and week 12)
There is increasing evidence of interaction between DAA therapy and HCC in the recent literature.Patients with HCC tend to have low rates of SVR12, whereas those who do not experience SVR12 have increased risk of HCC[16-18].In an editorial, Hollande and Pol[19]recommended intensive surveillance for HCC in patients who had DAA therapy failure.Yet researchers did not investigate these findings in LT recipients with PHCC[17].Consistently, we observed high risk of HCC recurrence in LT recipients who had DAA treatment failure.However, history of pre-transplant HCC did not impact SVR12 rates in patients treated with DAA post-LT as we removed tumor-affected livers.
LT recipients may be a reliable population to study the interaction between DAAs and HCC, especially in those with a failed DAA therapy after transplantation.This is driven by two factors.First, LT recipients have the benefit of receiving non-cirrhotic liver allografts with low prevalence of non-characterized nodules, which investigators have pointed to as the cause ofde-novoand recurrent HCC in patients undergoing DAA treatment[20].Moreover, LT recipients are not decompensated, as some authors attributed increased HCC risk in the DAA era to less selection bias when compared with that in the interferon era, as they excluded interferon-based treatment from decompensated patients with Child-Pugh class B or C[21].Second, the use of explant pathology to confirm the diagnosis of HCC rather than relying on imaging modalities that can misdiagnose HCC supports the use of LT recipients in investigating the interaction between DAA therapy and HCC.

Table 4 mean (± SD) platelet counts in patients who had direct-acting antiviral therapy responses and failure (baseline, week 4, week 8, and week 12)

Table 5 Risk factors for hepatocellular carcinoma recurrence post-liver transplant (Logistic regression analysis)
None of the patients in the present study who had DAA therapy failure or recurrence of HCC were cirrhotic.This contradicts the suggestion that HCC recurrence or DAA failure risk is greater in cirrhotic than non-cirrhotic populations.
Whereas a specific explanation for the interaction between HCC and DAA therapy has yet to be established, some studies suggested that cross-talk among inflammatory, immune response, and angiogenesis pathways modulates the impact of DAAs on progression of HCC and the risk of its recurrence[22,23].Additionally, HCC may interact biologically with DAA therapy, which may influence pre-transplant SVR12 achievement and increases the risk of HCC recurrence in patients who failed DAA therapy with a prior history of HCC irrespective of HCC treatment response or liver transplantation[17,19].Genetic susceptibility and variability in the genes involved in HCC risk or DAA metabolism may also play a role in the interaction between DAAs and HCC.Integration of the use of molecular markers with DAA therapy should be explored in future studies.

Table 6 Characteristics of the study population according to use of ribavirin
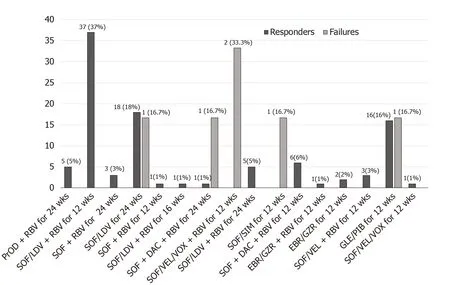
Figure 1 Numbers and percentages of the study patients who had responses to (n = 100) and failure of (n = 100) the 16 direct-acting antiviral regimens.
There is no consensus regarding the optimum time to start DAA treatment after an LT.We found no difference in the SVR12 rate between patients who received early (< 1 year) and late (≥ 1 year) DAA therapy after LTs.Nevertheless, five of six patients who did not experience SVR12 received DAA therapy more than 1 year after their LTs.
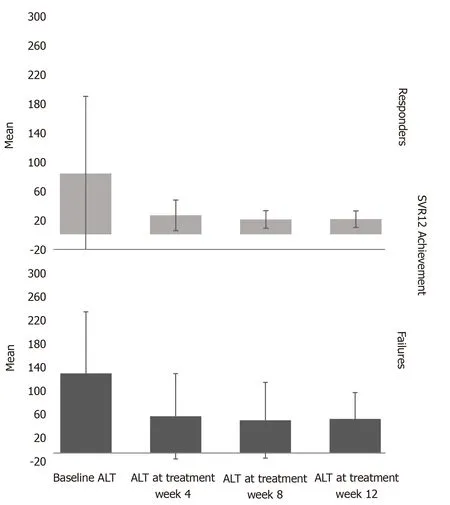
Figure 2 mean (± SD) alanine aminotransferase levels in patients who had direct-acting antiviral therapy responses and failure (baseline, week 4, week 8, and week 12).
We have no explanation why patients with PHCC received DAA treatment earlier than patients with PnHCC in our study.This may be attributed to more rigorous follow-up, better compliance, and fear of decompensation or HCC recurrence after liver transplantation in patients with PHCC.
During post-treatment follow-up, no patients had relapses after SVR12, with 100% concordance between SVR12 rates and SVR rates at follow-up week 24 and between SVR12 rates and quantitative HCV polymerase chain reaction at the last follow-up visit.This establishes SVR12 as an appropriate endpoint for demonstrating the clinical efficacy of all-oral DAA treatment similar to that in previous trials of sofosbuvir/RBV with and without interferon[24].
Consistent with a previous study[25], we showed that failure of the ALT level to normalize at treatment week 4 was a strong predictor of DAA treatment failure.This may result in enhancement of patient managementvia(1) Intensification of DAA treatment, either with RBV or extension of the treatment period, and (2) Thorough evaluation for other causes of a persistently elevated ALT level at treatment week 4, such as alcoholism, high body mass index, and type 2 diabetes mellitus.
Multivariate analysis showed no impact of HCV genotype 3 or an HCV-positive allograft on the risk of failure or HCC recurrence after DAA treatment.
Similar to other studies[13,14], we did not observe a significant difference in SVR12 rates between LT recipients who received DAA regimens with and without RBV.However, such an observation should be interpreted conservatively, as these patients were not randomized to receive RBV.Moreover, patients who received RBV were either cirrhotic or had a history of failure to antiviral therapy or quantitative HCV polymerase chain reaction > 15 IU/mL at treatment week 4, with RBV added to their regimens to intensify them and achieve SVR12.Use of RBV therefore may have helped this population to have an SVR12 rate similar to those in other favorable populations.
Overweight or obesity at baseline did not influence SVR12 achievement or HCC recurrence after DAA treatment.We observed no significant changes in body mass index from baseline to the end of DAA treatment.However, among those with PHCC, weight loss by the end of DAA treatment was a significant predictor of HCC recurrence, which may be attributed to release of inflammatory cytokines[26].
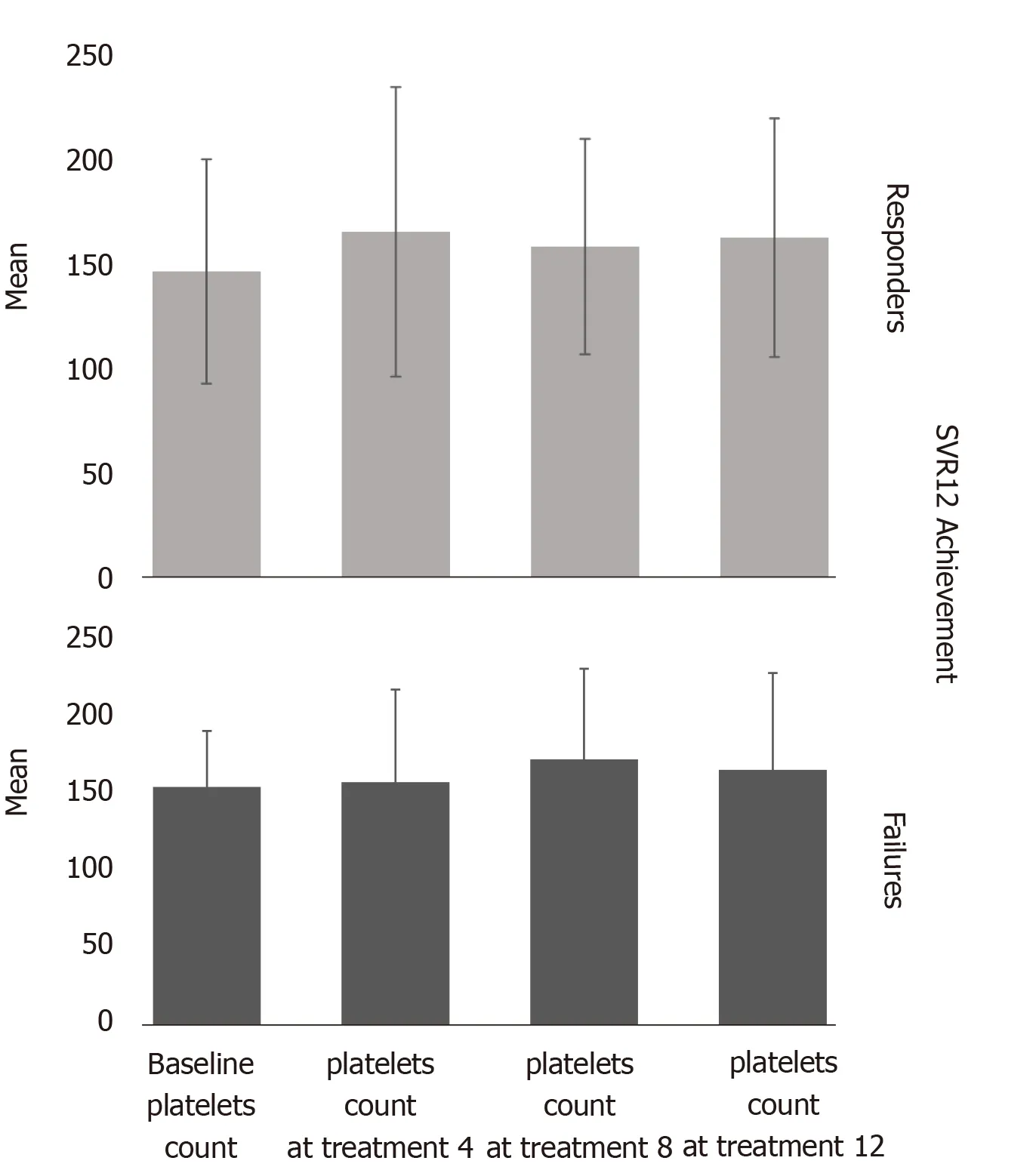
Figure 3 mean (± SD) platelet counts in patients who had direct-acting antiviral therapy responses and failure (baseline, week 4, week 8, and week 12).
Tacrolimus-containing regimens were the most commonly used immunosuppressive medications in DAA therapy.Acute cellular rejection occurred in 5% of the patients after DAA treatment (median time of 11 mo after therapy), which is comparable with rejection rates in the literature[13].
HBV reactivation with DAA treatment is rare, with an estimated risk of 1.4% in patients with resolved HBV infections[27].In our study, none of anti-HBc-positive patients experienced HBV reactivation during or after DAA therapy until the last follow-up visit.
This study has several strengths.It is the first to highlight predictors of HCC recurrence in patients in whom DAA treatment failed after an LT while adjusting for potential confounding factors.Furthermore, pre-transplant relapse to DAA therapy may predict post-transplant HCC recurrence.Given the uniqueness of LT recipients with recurrent HCV infection and HCC, we acknowledge the limitation of a singlecenter, retrospective study with a small sample size.Accordingly, we applied a rigid exact method of logistic regression analysis to overcome this limitation.
CONCLUSION
In conclusion, our results support the safety and efficacy of DAA treatment in LT recipients with history of HCC.Relapse to pre-transplant DAA therapy is a significant predictor of HCC recurrence following transplantation.Furthermore, relapse to posttransplant DAA therapy is associated with HCC recurrence.ALT level > 35 U/L at treatment week 4 is a significant predictor of treatment failure.Future validation of our findings in a multicenter study of a larger sample is warranted.
ARTICLE HIGHLIGHTS
Research background
Recent studies have shown lower sustained virologic response in patients with hepatocellular carcinoma (HCC) pre-transplant.Moreover, there are conflicting data regarding HCC recurrence in patients treated with direct-acting antivirals (DAAs).However, there are insufficient data regarding the efficacy of DAA in liver transplant(LT) recipients with past history of HCC.
Research motivation
To identify risk factors for DAA relapse and HCC recurrence after LT.
Research objectives
To highlight the efficacy and safety of DAA therapy in LT recipients with hepatitis C virus infections and history of HCC and to investigate the impact of DAA use on posttransplantation HCC recurrence.
Research methods
We retrospectively analyzed the data of our center of LT recipients who received DAA therapy for hepatitis C virus recurrence and their relapse and HCC recurrence outcomes.
Research results
Six patients (6%) experienced DAA therapy failure post-LT and 100 (94%) had a sustained virologic response at follow-up week 12.DAA relapse post-LT was associated with post-transplantation HCC recurrence,P= 0.05.Pre-LT DAA relapse is a predictor of post-LT HCC recurrence,P= 0.04.
Research conclusions
DAA is safe and effective in LT recipients with history of HCC.High alanine aminotransferase > 35 U/L at treatment week 4 and pre-LT DAA relapse are predictors of HCC recurrence after transplant.Relapse to DAA therapy post-LT is a potential risk factor for HCC recurrence.
Research perspectives
Performing a multicenter study of a larger sample to validate our findings.
杂志排行
World Journal of Hepatology的其它文章
- Clinical implications, diagnosis, and management of diabetes in patients with chronic liver diseases
- Biomarkers for hepatocellular cancer
- Comprehensive review of hepatotoxicity associated with traditional Indian Ayurvedic herbs
- N-acetylcysteine and glycyrrhizin combination: Benefit outcome in a murine model of acetaminopheninduced liver failure
- Transaminitis is an indicator of mortality in patients with COVID-19: A retrospective cohort study
- Surgical treatment of gallbladder cancer: An eight-year experience in a single center