Comprehensive review of hepatotoxicity associated with traditional Indian Ayurvedic herbs
2021-01-13CyriacAbbyPhilipsRizwanAhamedSasidharanRajeshTomGeorgeMeeraMohananPhilipAugustine
Cyriac Abby Philips, Rizwan Ahamed, Sasidharan Rajesh, Tom George,Meera Mohanan, Philip Augustine
Cyriac Abby Philips, The Liver Unit and Monarch Liver Lab, Cochin Gastroenterology Group, Ernakulam Medical Center, Kochi 682028, Kerala, India
Rizwan Ahamed, Philip Augustine, Gastroenterology and Advanced GI Endoscopy, Cochin Gastroenterology Group, Ernakulam Medical Center, Kochi 682028, Kerala, India
Sasidharan Rajesh, Tom George, Division of Hepatobiliary Interventional Radiology, Cochin Gastroenterology Group, Ernakulam Medical Center, Kochi 682028, Kerala, India
Meera Mohanan, Anesthesia and Critical Care, Cochin Gastroenterology Group, Ernakulam Medical Center, Kochi 682028, Kerala, India
Abstract With growing antipathy toward conventional prescription drugs due to the fear of adverse events, the general and patient populations have been increasingly using complementary and alternative medications (CAMs) for managing acute and chronic diseases.The general misconception is that natural herbal-based preparations are devoid of toxicity, and hence short- and long-term use remain justified among people as well as the CAM practitioners who prescribe these medicines.In this regard, Ayurvedic herbal medications have become one of the most utilized in the East, specifically the Indian sub-continent, with increasing use in the West.Recent well-performed observational studies have confirmed the hepatotoxic potential of Ayurvedic drugs.Toxicity stems from direct effects or from indirect effects through herbal metabolites, unknown herb-herb and herbdrug interactions, adulteration of Ayurvedic drugs with other prescription medicines, and contamination due to poor manufacturing practices.In this exhaustive review, we present details on their hepatotoxic potential, discuss the mechanisms, clinical presentation, liver histology and patient outcomes of certain commonly used Ayurvedic herbs which will serve as a knowledge bank for physicians caring for liver disease patients, to support early identification and treatment of those who present with CAM-induced liver injury.
Key Words: Ayurveda; Complementary and alternative medicines; Drug induced liver injury; Herb induced liver injury; Chronic liver disease; AYUSH system
INTRODUCTION
Ayurveda, an ancient traditional system of medicine, originated in the Indian subcontinent.According to Ayurvedic principles, the Universe is composed of five elements, namely,Vayu(Air),Jala(Water),Aakash(Space or ether),Prithvi(Earth) andTeja(Fire) that form the three elemental humors of the human body in varying combinations - theVata dosha,Pitta dosha, andKapha dosha, collectively called the“Tridoshas”that, along with five sub-categories for each of the primarydoshasare thought to control all of the essential physiological functions of the human body.Even though practitioners of Ayurveda believe it to be a complete system of medicine, Ayurvedic science lacks the rigorous and ideal scientific approach required for disease diagnosis and treatment.This is underscored by the fact that prospective, welldesigned, good quality controlled trials are deficient in the current literature concerning Ayurvedic practice[1].In contrast, integrative approaches toward practices in Traditional Chinese Medicine (TCM) has been exemplary, improving our understanding of beneficial active components in Chinese herbs which have been ultimately utilized in the management of lethal and resource burdening diseases such as malaria.Ayurvedic herbal medicines (AHM) are broadly divided into nonproprietary or classical and proprietary drugs.In the former, manufacturing methodology follows principles and guidelines as per approved classical texts of Ayurveda (such asCharak SamhitaorSusrut Samhita); while in the latter, private drug manufacturers decide on the content, composition and preparatory methods involved in the preparation of the AHM (examples include Himalaya®Liv 52™ or Charak®Livomyn™ syrup).Daset al[2]in a study from North-East India, found that unknown herbal medications were a significant cause of mortality among patients with acute liver failure (ALF).Similarly, Udayakumaret al[3]demonstrated that traditional indigenous herbal medications prescribed by South-Indian Tamil healers led to ALF with high mortality in affected patients[3].In a large single-center series from South-India, Devarbhaviet al[4]found that Indian Ayurvedic medicines caused drug-induced liver injury (DILI) in 1.3% of patients in whom almost half of those affected died due to progressive liver failure.In a pioneering study, Philipset al[5]addressed clinical outcomes and analyzed component toxicology of AHMs causing severe DILI.In this study, patients were prescribed AHMs mainly for non-specific gastrointestinal symptoms.The overall mortality was approximately 19% and most of the formulations were unlabelled polyherbals, with high levels of arsenic and mercury which were significantly associated with death on follow-up[5].The same authors showed that among cirrhosis patients consuming AHMs, 35.7% presented with severe DILI leading to acute on chronic liver failure (ACLF) with an overall mortality of 53%.In this series, the most common culprit leading to AHM-DILI were unlabelled polyherbal preparations followed by proprietary Ayurvedic drugs[6].A recent multicentre study spearheaded by the Asian-Pacific Association for the Study of Liver (APASL) demonstrated that ACLF in Asia-Pacific countries was predominantly due to CAMs (in approximately 72% of patients) inclusive of Ayurvedic herbals and herbal and dietary supplements[4].Components implicated in DILI related to Ayurvedic medicines are difficult to ascertain due to mislabelling or un-labelling of the product, presence of potentially toxic adulterants or contaminants, and importantly, the complex polyherbal nature of preparations.In this context, a precise knowledge regarding certain potentially hepatotoxic herbs is of utmost importance for the clinician while dealing with patients with AHM-related DILI.In this review, we discuss exhaustively from current literature, the hepatotoxicity of common Indian Ayurvedic herbs that are utilized in pure form or as mixtures; explore pertinent clinical presentations and outcomes with real-life patient examples and summarize to provide future directions on Ayurvedic herbs-related DILI.
AYURVEDIC HERBS WITH POTENTIAL HEPATOTOXICITY
Withania somnifera (Ashwagandha)
Ashwagandha is a herbal extract derived from the roots ofWithania somnifera, an evergreen shrub endemic to India and Southeast Asia, commonly known as the Indian ginseng or winter cherry.It is claimed to have neuroprotective and anti-inflammatory properties and has been used to treat a variety of symptoms and diseases ranging from fatigue, stress, epilepsy and arthritis to cancer chemoprevention.Some Ayurvedic practitioners and drug manufacturers proclaim that Ashwagandha has “anti-aging” properties.Multiple studies performed on small animal-models and published in anecdotal journals have alleged a “liver safe” profile[7,8].Apart from a few randomized clinical trials with small patient numbers but with penurious methodology, and short follow-up, there have been no rigorously performed, scientifically sound, prospective studies confirming the efficacy and safety of Ashwagandha in the current literature[9].The bioactive compounds identified in Ashwagandha include steroidal lactone triterpenoids (called withanolides), alkaloids such as cuscohygrine, and anahygrine, flavonoids, phytosteroids and coagulins.The terpenoid Withaferin A is purported to have hepatoprotective properties.The first report of possible Ashwagandha-related DILI was from Japan.Inagakiet al[10]described a 20-year-old man with anxiety disorder who used twice the recommended dose of Ashwagandha bought online in combination with multiple antianxiety drugs.The pattern of DILI was of ”highly possible” cholestatic type as per the Digestive Diseases Week – Japan 2004 (DDW-J) diagnostic criteria.The liver biopsy showed severe intrahepatic cholestasis with extensive canalicular bile plugs.The patient recovered uneventfully within 2 mo after treatment with ursodeoxycholic acid, phenobarbitone, and withdrawal of the offending drug.A drug-induced lymphocyte stimulation test revealed reactivity and drug interactions between Ashwagandha, propranolol, and alprazolam[10].Björnssonet al[11]reported on a series of patients from Iceland and the United States Drug-Induced Liver Injury Network (DILIN) with liver injury due to Ashwagandha.The authors described five patients, mostly males with a mean age of 43 years, who developed cholestatic jaundice after consuming a herbal supplement ranging from 2 to 12 wk.Liver injury was cholestatic or mixed type and liver biopsy showed severe cholestatic hepatitis.The clinical course was prolonged, ranging from 5 to 20 wk and normalization took up to 5 mo.None of the patients developed liver failure.Chemical analysis using liquid chromatography coupled to quadrupole time-of-flight mass spectrometry on the retrieved products confirmed the presence of Ashwagandha, the absence of other toxic compounds or the presence of potentially hepatotoxic conventional drugs.In one patient, the additional consumption ofRhodiola rosea(golden root or roseroot) was suspected to have caused a herb-herb interaction resulting in the liver injury[11].Ashwagandha-containing herbal medications can result in severe cholestatic liver injury, which may be prolonged, but self-liming without the development of chronic DILI or ALF (Figure 1).
Bacopa monnieri and Centella asiatica (Brahmi/Gotu Kola)
The herb Brahmi, used synonymously with Gotu Kola is extensively utilized in Ayurveda due to its seemingly beneficial effect on neurocognitive functions.Both have distinct biochemical component properties, pharmacokinetics, and pharmacodynamics, and are considered separate herbs in the ancient Ayurvedic texts.Nonetheless, both are commonly used as memory ”boosters” or cognition enhancers.Brahmi is essentiallyBacopa monnieri, a perennial non-aromatic creeping herb, also called the water hyssop.The primary bioactive constituents of Brahmi include steroidal saponins called bacosides, alkaloids such as Brahmine, herpestine, and nicotine.Gotu Kola orCentella asiaticacommonly called the Indian pennywort, is a perennial flowering plant that is indigenous to the Indian subcontinent and Southeast Asia.Similar to Brahmi, the bioactive components in Gotu Kola are saponintriterpenoids, which include asiaticosides, brahmoside, and Brahminoside as well as the glycosides isothankuniside and thankuniside[12,13].In their report on severe hepatotoxicity due to Ayurvedic herbal products, Teschke and Bahre described an older woman who developed a severe hepatocellular type of DILI after consuming multiple herbal products for 9 mo for vitiligo.All other competing causes were systematically excluded by the authors.On structured causality assessment using the Council for International Organizations of Medical Sciences (CIOMS) scale on individual products, the authors found that primary hepatotoxicity was possibly due to ”Bakuchi” tablets (score 8+), containing extracts ofPsoralea corylifolia(also called babchi or purple fleabane; discussed later).However, the CIOMS score was 6+ (possible) for Brahmi tablets.Properly conducted structured studies or pharmacovigilance on organ-specific toxicity of Brahmi is deficient in current literature[14].Gotu Kola is also implicated in contact dermatitis (due to the presence of madecassoside) and infertility due to bioactive components, isothankuniside, and thankuniside[15,16].An Argentinian group of researchers were the first to describe a series of women in whom ingestion of Gotu Kola for weight loss for approximately one to two mo resulted in severe cholestatic hepatitis.Liver biopsy revealed acute granulomatous hepatitis, with marked necro-inflammatory activity and eosinophilic degeneration mainly in zone 3, along with a lymphoplasmacytic infiltrate in all patients, and additional features of chronic hepatitis with prolonged cholestasis and progression to cirrhosis in one patient.In the patient with chronic DILI-related cirrhosis, acute decompensation developed with repeat intake.In other patients, drug withdrawal, along with a short course of corticosteroids and ursodeoxycholic acid therapy resulted in a complete reversal of liver injury at one year follow-up.In the first patient, repeat consumption of Gotu Kola seven mo later led to recurrence of DILI with similar biopsy features to the initial biopsy.In both instances, autoantibodies were positive favouring the possibility of immune-mediated DILI[17].In another report, Gotu Kola intake for 6 wk for acne treatment led to ALF in a 15-year old girl with complete resolution of illness after drug withdrawal[18].Phytochemicals such as alkaloids and cyclic compounds undergo biotransformation in the liver leading to the generation of metabolites that cause direct damage to hepatocytes and cholangiocytes or generate antigens, which trigger immune-mediated liver injury.In Gotu Kola, the bioactive compounds such as asiaticoside are triterpenoids which belong to the same family of hepatotoxic saponosides found in other herbs such as germander and Chinese skullcap.These bioactive compounds induce apoptosis through alteration of cellular transport at the cell membrane level, which characteristically could result in eosinophilic degeneration and cellular necrosis seen on liver histopathology[14-17].Brahmi or Gotu Kola related DILI presents with cholestatic granulomatous hepatitis and severe autoantibody mediated necroinflammation (Figure 2).A strong suspicion for the intake of these herbs should be considered in patients presenting with acute onset cholestatic hepatitis with autoantibodies and biopsy features of granulomatous hepatitis after excluding other causes.
Curcuma longa (Turmeric)

Figure 1 Liver histopathology of acute liver injury in a patient ingesting Ashwagandha.
Turmeric and its bioactive compound curcumin are derived from the root ofCurcuma longa, a perennial plant that is native to India, belonging to the ginger family.In Ayurvedic practice, it is heavily used as an anti-inflammatory and antioxidant as well as for digestive system-related symptoms and diseases such as pharyngitis, inflammatory bowel disease and fatty liver disease.Turmeric contains 3%-6% polyphenolic compounds (curcuminoids) such as curcumin, desmethoxycurcumin, and bisdemethoxycurcumin, which are responsible for its bioactivity.Turmeric is also rich in phytosteroids and bioactive compounds that have immunomodulatory properties[19,20].Even though Ayurvedic practitioners vouch for the multisystemic beneficial effects of turmeric, a strong scientific basis for its efficacy and safety has not been proven through meticulous clinical studies.The majority of the beneficial effects of turmeric or its bioactive agents are still confined to small animal model studies without adequate translation to human diseases[21].Lukefahret al[22]described the case of highly probable drug-induced autoimmune hepatitis (AIH) ascribed to ingestion of turmeric dietary supplement for 10 mo in a 76-year old woman.The immunoglobulin G levels were elevated along with positive autoantibody titres for atypical perinuclear anti-neutrophil cytoplasmic antibodies and antibody to smooth muscle actin.Liver histopathology was compatible with AIH, and other causes of acute hepatitis were ruled out.After withdrawing the turmeric supplement, liver injury improved within 1 mo and returned to normal within a year and remained so at the three year followup[22].Similar reports of AIH-like severe hepatitis associated with turmeric use were reported by Suhailet al[23]and Leeet al[24].Imamet al[25]reported the case of a 78-year old female who ingested an over-the-counter curcumin supplement for dyslipidemia for 1 mo.She presented with progressive jaundice without cholestasis.The DILI was of hepatocellular type and other competing causes of acute hepatitis were ruled out.After stopping the supplement, the liver tests showed approximately 50% improvement at the end of one week and complete resolution by day 42.The authors did not review or analyse the curcumin supplement for adulterants and contaminants, and a liver biopsy was not performed given clinical improvement[25].Luber and coworkers described two cases of curcumin-related severe hepatocellular DILI in their paper.The first patient was a woman in her early fifties with cholestatic hepatitis on Ancient Wisdom™ High Potency Turmeric (375 mg curcuminoids + 4 mg black pepper) for 1 mo before the onset of symptoms.Her liver biopsy revealed severe lobular mixed inflammation and interface hepatitis.After resolution of liver injury within 2 mo, she restarted the turmeric supplement (1125 mg curcuminoids per day) for 3 wk and presented with severe cholestatic hepatitis again.Further withdrawal resulted in complete resolution of symptoms.Analysis of the sample did not reveal any adulterants, toxins, heavy metals, or synthetic drugs.The second case was of DILI with autoantibodies in a 55-year-old male with metabolic syndrome after ingestion of turmeric-based supplements for cardiovascular health[26].Similar biopsy findings and clinical outcome related to turmeric-induced severe liver injury was reported by Chandet al[27].The patient developed additional features of severe myalgia, skin rash, and arthritis which resolved with normalization of liver tests after turmeric supplement withdrawal.We noted that in a middle-aged female patient with compensated hepatitis B virus-related cirrhosis, the use of turmeric capsules (1g per day for 3 wk) resulted in severe spur-cell anemia requiring blood transfusion, which resolved spontaneously on drug withdrawal, but reappeared after rechallenge (same dose for 2 wk) to resolve again after halting the turmeric supplement (Figure 3).To summarize, turmeric and its bioactive compounds have been implicated in rare but severe autoimmune hepatitis-like liver injury and rarely, severe self-limiting cholestasis with the potential to recur with drug rechallenge.

Figure 2 Granulomatous hepatitis in a patient consuming multiple Ayurvedic herbs.
Commiphora wightii or mukul and Boswellia serrata (Guggul, Guggulu or Gugulipid)
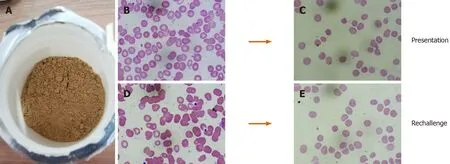
Figure 3 Turmeric-induced spur cell anemia in a patient with compensated cirrhosis.
Guggul is the gum resin procured from the white sap of various plants used in Ayurvedic practice.Two plants,Commiphora wightii(Indian bdellium or myrrh tree) andBoswellia serrata(Salai or Sallaki guggul or Shallaki from Indian olibanum or frankincense tree) are commonly utilized to prepare guggul.Guggul is considered to have beneficial effects on multiple organ systems and is used to treat symptoms ranging from leg swelling and non-specific ulcers to diseases such as inflammatory bowel disease and aggressive malignancies.The main ingredients of guggul are guggulsterone, guggulsterol, boswellic acid and an ethyl-acetate soluble fraction called guggulipid consisting of highly bioactive phytochemicals.A large number ofin vitroandin vivostudies have shown that guggul and its bioactive components act on multiple molecular targets leading to anti-inflammatory, antioxidant, and antiapoptotic activity.This has led to the use of guggul for conditions such as arthritis, in fat-burners, for dyslipidemia and cardiovascular health.However, studies on the safety and clinical efficacy of guggul or its specific bioactive components are nonexistent in published literature[28].Griecoet al[29]described the case of a 63-year-old woman who consumed an over-the-counter lipid-lowering Ayurvedic product called ”Equisterol®” (containing guggul sterol, sitosterol, chlorogenic acid, policosanol, multivitamins and red yeast rice derived monacolin) for 6 mo which was followed by the development of acute severe hepatitis.Liver biopsy revealed extensive necroinflammation with eosinophilic infiltration of hepatic lobules.Drug withdrawal and supportive care led to complete resolution of symptoms and normalization of liver tests within 10 d.The liver injury could have been due to the monacolin (with statins like activity) in red yeast, even though herb-yeast interaction was not ruled out[29].Yellapuet al[30]described a female bodybuilder who consumed a multiingredient fat burner supplement leading to ALF.The supplements (Somalyz and Lipolyz, Species Nutrition, United States) contained usnic acid, L-carnitine, choline and ethanolamine, gamma-aminobutyric acid, vitamin E, green tea extract, guggulsterone Z, and guggulsterone E.She underwent cadaveric liver transplantation and was discharged uneventfully.Explant histopathology revealed massive hepatic necrosis and parenchymal collapse with a few areas of ductular regeneration.Even though various known plant-derived hepatotoxins (such as usnic acid, green tea extracts) were components of the supplement, the presence of guggul and its interactions were not ruled out.Guggul use has been implicated in the development of skin rash, diarrhea, headaches, nausea, and liver toxicity with high doses[30].As reported by Polavarapu and co-workers, a 44-year old male developed fatigue, malaise, and jaundice after consuming a fat-burner product (Lipo-6™ containing guggulsterones and green tea extract) for 1 mo.Withdrawal of the herbal supplement resulted in complete clinical resolution after 1 mo[31].Dalalet al[32]described a middleaged woman who developed severe hepatocellular jaundice due to the intake of three different Ayurvedic herbal and Homeopathic medications (punarnaya mandur, extract from theBoerhavia diffusaand kanchnar guggulu, extract fromBauhinia variegate).Liver biopsy demonstrated mild portal chronic inflammation and interface activity with grade 3 bridging fibrosis, presence of ceroid-laden Kupffer cells, and conspicuous eosinophils suggestive of herbal-induced liver injury.Analysis of the retrieved herbal products and other medications did not reveal known hepatotoxic components, and the patient improved after a short follow-up[32].Guggul and its bioactive compounds have been implicated in possible and probable DILI with hepatocellular pattern of liver damage, which is usually self-limiting.However, there have been reports of ALF requiring liver transplantation when guggul compounds have been part of multiherbal fat-burner products, a herb-herb interaction that remains unexplored (Figure 4).
Psoralea corylifolia (Bakuchi)

Figure 4 Guggul-related liver toxicity.
Psoralea corylifolia, commonly known as purple fleabane, is a popular herb used in Ayurvedic medicine for the treatment of various skin disorders.It is a perennial plant with growth throughout the plains of the Indian continent.Seeds of the plant (known asFructus Psoraleae, FP) are mainly used for treating leprosy (hence the Sanskrit name, ”kushtanashini” or destroyer of leprosy), psoriasis, leukoderma, and vitiligo.The monoterpenoid phenol called bakuchiol is the most important phytochemical component.Other constituents include coumarin compounds such as active psoralens, benzofuran derivatives and flavonoids[33].A case of severe acute cholestatic hepatitis associated withFPwas reported by researchers in South Korea in a post-menopausal woman consuming more than the recommended dose of the extract for osteoporosis.The liver biopsy findings were suggestive of zone 3 necrosis, cholestasis, and mixed inflammation in the lobules[34].Three further cases of severe hepatotoxicity due toFPwas reported by Cheunget al[35].The analysis of the retrieved proprietary medicines revealed psoralens and bakuchiol[35].In another report, Bakuchi tablets were considered the cause of severe hepatocellular type liver injury in an older woman consuming Ayurvedic medicines for vitiligo[32].A similar case was reported by Smithet al[36], of a 52-year old female who presented with a one-week history of jaundice and severe pruritus with abdominal pain after ingesting Bakuchi seeds for vitiligo.The liver biopsy revealed centrilobular necrosis with collapse, extensive cholestasis with mixed lobular inflammation.Clinical improvement and normalization of liver chemistries were notable at 3 mo follow-up[36].Recently, Li and colleagues described a case of severe cholestatic hepatitis leading to fatal ALF due to the consumption of Bakuchi seeds over 7 mo in a 53-year-old with vitiligo.Studies have shown multiple mechanisms for Bakuchi-related liver toxicity.The psoralen-induced inhibition of the mTOR signalling pathway, mitochondrial injury, and impairment in liver regeneration with deleterious effects on liver lipid metabolism (such as reduction of mRNA expression of CYP7A1, HMG-CoA reductase, PPARα and increased expression of BSEP) along with dose and frequency related accumulation of psoralen has been shown to promote hepatotoxicity in small animal andin vitrostudies[37-39].To summarize, prolonged use of Bakuchi is associated with severe cholestatic hepatitis, mostly related to hepatotoxic psoralen compounds and bakuchiol, that can lead to ALF and death in predisposed patients.
Cassia angustifolio (Indian Senna)
Cassia angustifoliaor the Indian or Tinnevelly senna (containing tinnevellin glucosides) belong to the legume family of Fabaceae, which comprise mostly ornamental plants.Leaves and sometimes flowers and fruits of the senna plant are used in herbal teas and as laxatives in Ayurvedic and Egyptian or Alexandrian (species known asCassia acutifolio; containing 6-hydroxymusicin glucoside) traditional medicine.Some consider senna to be a safe herbal alternative for weight loss.The major bioactive components are anthracoids (sennoside A and B), which are primarily anthraquinone glycosides[40].Beuerset al[41]described a 26-year old nurse who presented with severe cholestatic hepatitis after consuming high doses of senna-based medicines for 1 mo (senna fruit extracts corresponding to 100 mg sennoside daily along with 10 g of folia sennae laxative herbal tea twice weekly).Her liver biopsy showed extensive necrosis around the central veins, moderate portal and lobular infiltration of lymphohistiocytes and occasional plasma cells in the absence of autoantibodies.After drug withdrawal, liver tests, and clinical symptoms normalized, only to recur after resuming senna medications after 2 mo, and improving again, after drug withdrawal.Sennosides are converted into rhein anthron in the intestine most commonly byEscherichia coli, which is then absorbed through the intestinal mucosa, glucuronidated, or sulfated and excreted through feces and urine.Rhein anthron is structurally similar to danthron, which is a well-known hepatotoxic laxative.The anthraquinones in rhubarb of which rhein anthron is a major component has been shown to be associated with liver injury[41].A similar case was reported by Sonmezet al[42]in a 77-year old male in whom liver biopsy revealed bridging hepatocellular necrosis and canalicular cholestasis with slow but steady normalization of DILI on long-term follow-up.Seyboldet al[43]reported the case of a young woman with CYP2D6*4 homozygous variant in whom, the repeated use of comparatively small quantities of senna herbal tea led to severe acute hepatitis which resolved after drug withdrawal.The authors concluded that ”poor metabolizers” of phase I hepatic detoxification were predisposed to severe liver injury due to senna[43].Vanderperrenet al[44]demonstrated that chronic ingestion of large amounts of senna fruits in the form of herbal tea led to ALF associated with acute kidney injury and severe coagulation failure in a 52-year old woman.Investigations revealed large amounts of cadmium on urine toxicology consistent with possible contamination of the herbal product with heavy metals[44].Cadmium is a well-known cumulative nephrotoxic and hepatotoxic agent, demonstrated in multiple Ayurvedic herbal products as a contaminant or adulterant and associated with severe liver injury[4,5,45,46].Severe hepatotoxicity leading to fatal ALF was noted in an older woman consumingSenna occidentalis(S.occidentalis) herb for constipation.S.occidentalisis a common weed that is considered highly toxic to cattle and small herbivores.Recurrent annual outbreaks of a hepato-myo-encephalopathy syndrome in children in western Uttar Pradesh in India due toS.occidentalispoisoning was also reported by Vashishthaet al[47,48].In the absence of proper regulatory standards, oversight, and poor manufacturing practices associated with Ayurvedic medicines, contamination of classical senna preparations with similar but more toxic herbs remain a possibility for causes concerning sporadic liver injuries[49].Portal vein thrombosis due to consumption of boiled, dried Indian senna leaves in a 42-year old woman without underlying comorbid disease or prothrombotic conditions was also reported in the literature[50].To summarize, senna is associated with severe hepatocellular and cholestatic liver injury and possible renal injury due to the presence of anthraquinone alkaloids in predisposed patients.The clinical course is usually self-limiting with liver toxicity proven on re-challenge; however, in rare instances, fatal ALF has been reported.
Aloe barbadensis mille (aloe vera)
Aloe vera is a perineal, xerophytic, succulent, cactus-like shrub belonging to the Lily family used for centuries in traditional medicine for the management of skin diseases, wound healing; and orally as an anti-oxidant.Aloe is derived from the Arabic word ”Alloeh, ” meaning ”shining bitter substance” while ”vera” is Latin for ”true” and called by Egyptians as the ”plant of immortality.” The aloe leaf contains glucomannans such as acemannan, the anti-inflammatory glycoprotein alprogen and multiple anthraquinones such as aloin and emodin and the plant hormones auxins and gibberellins[51].The first report of aloe-induced acute hepatitis was published by Rabeet al[52]from Germany in 2005.In their paper, a middle-aged woman developed acute severe cholestatic jaundice after ingesting aloe supplements (500 mg tablets) for 4 wk to delay ”aging”.The liver biopsy revealed portal and lobular lymphoplasmacytic infiltrates and eosinophilic granulomas with bridging necrosis and bilirubinostasis.The liver injury and symptoms abated after stopping the aloe tablets.The authors contemplated that the liver injury was possibly due to the presence of bioactive aloe alkaloids acting on the cytochrome P450 system resulting in detoxification process interference and direct action of biotransformation end metabolites causing hepatocytotoxicity[52].Since its original description, multiple reports, including patient series from Korea and Sweden and an extensive literature review on aloe-induced hepatitis, have been published in the literature.Liver biopsy findings in subsequent studies also featured severe hepatocyte ballooning, apoptosis, extensive cholestasis, and the presence of eosinophils predominant lobular inflammation[53,54].Apart from hepatotoxicity, additional systemic toxicity in the form of severe intraoperative bleeding due to probable interaction between aloe plant-derived prostaglandins and sevoflurane during leg surgery in a young woman; renal failure due to over-dosing on aloe products; aloe-induced Henoch-Schonlein purpura and cathartic melanotic colon with adenomas are reported with aloe vera use[55].Patient series of herbal and dietary supplements induced liver injury, mostly due to Herbalife®products, containing aloevera extracts leading to severe liver injury are also well documented in certain pharmacovigilance registries such as the Spanish DILI registry[56].Even thoughin vitroandin vivostudies have demonstrated the detoxifying and hepatoprotective potential of aloe vera, well-conducted translational clinical trials in humans confirming this aspect are still lacking in published literature.Aloe-related acute decompensation of cirrhosis in a chronic hepatitis C virus patient, presenting with acute severe cholestatic jaundice, was reported by Vázquez-Fernándezet al[57].To summarize, oral aloe vera use ranging from 2 wk to 24 wk, reportedly leads to severe cholestatic hepatitis among predisposed patients as well as acute severe decompensation in patients with underlying chronic liver disease.The injury is mostly of the hypersensitive type and self-limiting but may have a prolonged morbid course (Figure 5).
Morinda citrifolia (Indian mulberry or Noni juice)
Morinda citrifolia, commonly known as noni, belongs to the coffee family cultivated throughout the tropical countries.Due to its strong and pungent odor, it is also known as cheese fruit or vomit fruit.Noni-related products in the form of juice or extracts are considered by traditional medicine practitioners to benefit diseases from mouth ulcers to diabetes and HIV-AIDS even though high quality and reproducible studies demonstrating alleged clinical efficacy are non-existent in the literature.Published data on the efficacy and safety of noni juice and extracts are limited toin vivoandin vitrostudies that are widely (and inaccurately) quoted by manufacturers and sellers of noni juice as strong evidence for its practical and safe use.Compositional analysis of noni demonstrated alkaloids (xeronine), polysaccharides, anthraquinones (damnacanthal, morindone), and glycosides such as citrifolinoside[58].Austrian researchers described a 45-year-old man who consumed noni juice for 3 wk as a ”prophylactic antioxidant, ” and developed acute hepatitis.The liver biopsy revealed severe mixed inflammation of the portal tracts along with marked eosinophils, hepatocellular cholestasis in zone 3, and histiocytic infiltration of the sinusoids.Complete resolution occurred within ten days of stopping noni juice[59].Stadlbaueret al[60]described the occurrence of ALF requiring liver transplantation in a 29-year-old man and severe acute hepatitis due to consumption of noni juice for 3-mo in an elderly woman with a self-limiting disease course in the latter.The biopsies revealed severe mixed inflammation of portal tracts and lobules along with extensive centrilobular necrosis and severe ballooning associated with mixed inflammation[60].Nonetheless, the development of ALF in the former patient cannot be solely attributed to noni juice since multiple other potentially toxic herbal supplements such as Skullcap (a known hepatotoxic Chinese herb), and green tea extracts were also consumed during the same period.Further reports of liver injury due to noni juice have been published from Croatia, Germany, and recently the United States.In these cases, where liver biopsy was performed, the findings were similar to previously described cases – a predominant hepatocellular form of liver injury with a mixed pattern of inflammation with marked eosinophilic infiltration of portal tracts, perivenular hepatocellular zonal necrosis with hepatocellular or canalicular cholestasis.All had a self-limiting disease course with complete clinical resolution within weeks to months[61].Manufacturers and proponents advocating the benefits of noni juice with vested business interests have been keen to publish their retaliation against published literature on noni juice-related hepatotoxicity.However, almost all of their justifications have been biased and based on anecdotal and narrative evidence especially the efficacy and safety aspects of noni juice since idiosyncratic hepatotoxicity as a possibility has never been ruled out[62].Further to this, multiple instances of the United States Food and Drug administration serving warning letters to manufacturers for making false claims on the curative and health benefits of noni has been in the limelight recently[63].Current literature on the hepatotoxicity of noni juice demonstrates a possible self-limiting idiosyncratic type of herb-induced liver injury, probably due to anthraquinones, presenting with a severe hepatocellular type of liver damage with a predominance of eosinophilic portal inflammation, central necrosis, and cholestasis.
Ayurvedic herbs containing pyrrolizidine alkaloids
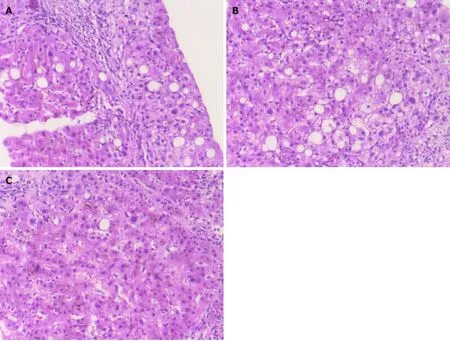
Figure 5 Aloe vera-induced liver injury in a middle-aged diabetic woman.
Alkaloids belong to the group of amino acid-derived, nitrogen-bearing molecules displaying a wide range of biochemical activities.Pyrrolizidine alkaloids (PAs) are those derived from ornithine and are commonly found as esters formed by a necine base (amino alcohols) and one or more necic acids (mono- or aliphatic dicarboxylic acids).Accordingly, based on the structure of the necine base, PAs may be sorted into four groups: Retronecine-, heliotridine-, otonecine- and platynecine-types.The following plant species -Heliotropium sp., Trichodesma sp., Symphytum sp.(known as Comfrey),Senecio sp.(used in Bush teas),Eupatorium sp., Crotalaria sp.(commonly used in Indian Ayurveda),Chelidonium majus sp., andCastilleja sp.are known to be rich in PAs.In 1968, Mattocks was the first to describe the hepatotoxicity mechanism of PA, which leads to hepatic veno-occlusive disease, currently known as hepatic sinusoidal obstruction syndrome (HSOS), a condition that can lead to liver failure potentiating organ transplantation or to cirrhosis and portal hypertension[64].PAs are transformed and activated into intermediate metabolites of which dehydropyrrolizidine alkaloids (DHPAs) are of significance.DHPA bind with groups containing sulfur, nitrogen, and oxygen present in proteins to form adducts that penetrate the nucleus and react with DNA, ultimately causing DNA cross-links and DNA-protein cross-links resulting in genotoxicity and abnormal cellular function primarily in the liver, leading to hepatocyte damage.These adducts pass to the adjacent space of Dissé as well as the sinusoidal lumen, where they injure the sinusoidal cells leading to HSOS.Apart from the liver, DHPA can also reach the pulmonary arterioles leading to secondary pulmonary hypertension and, in the long-term, congestive heart failure.Tricodesmine, a PA metabolism byproduct is neurotoxic and can cause encephalitis, vertigo, delirium and coma.The case of HSOS in a newborn of a woman who consumed herbal tea prepared fromTussilago farfaraL showcasing the teratogenicity of PA is also reported[65].The cognizance that PA-containing herbs can promote HSOS development comes from the identification of a large number of sporadic cases from Africa and the Indian subcontinent among those consuming herbal teas and ingesting traditional healer concoctions.Cross-contamination of herbal teas with PA-rich herbs leading to liver toxicity is also described.In India, consumption of honey processed (during pollen drying) using PA containingCrotalaria junceaL has been demonstrated to promote PA toxicity[66].Figure 6 demonstrates the serial liver biopsy of a young male who developed HSOS leading to cirrhosis and portal hypertension at one year followup, after consuming over-the-counter capsule extracts ofHolarrhena antidysenterica (pubescens)for ”indigestion” for 1 mo.H.antidysentericacontains PAs, and rats fed with extracts demonstrated liver toxicity in the form of injury to centrilobular veins, centrilobular sinusoidal hemorrhage, congestion and centrilobular and focal hepatocellular necrosis compatible with PA-induced damage[67].Thorough knowledge of herbs promoting chronic and sub-acute liver injury, and careful assessment of herbal components in polyherbal medications is mandated by physicians treating probable cases of DILI due to Ayurvedic drugs to diagnose rare but possible causes of herbal hepatotoxicity that may progress to chronic liver disease and portal hypertension.

Figure 6 Hepatic sinusoidal obstruction syndrome in a young male who consumed Holarrhena antidysenterica, known to contain pyrrolizidine alkaloids.
Miscellaneous Ayurvedic Herbs
Garcinia cambogia (Malabar Tamarind):Currently known asGarcinia gummi-gutta(L) Roxb, the fruit rind is extensively used as a flavouring agent in many parts of the Indian subcontinent.In Ayurvedic medicine, it has been purported to be a safe remedy for constipation, rheumatic diseases, helminthic infestation, and as a weight-loss agent due to its appetite suppressing activity.Hydroxy-citric acid (HCA), an α-,β-dihydroxy tricarboxylic acid, is the major component present in the fruit rind, which may be responsible for the anorexic property.Garcinia fruit contains approximately 10% to 30% HCA, which reduces weight gain by inhibiting adenosine triphosphate (ATP)-citrate lyase, the enzyme responsible for catalytic reactions during fatty acid synthesis.Further appetite suppression occurs through increased release of serotonin neurotransmitter that dissipates eating behaviour.Multiple small animal model studies have demonstrated the anti-diabetic, anti-obesity, hypolipidemic, antiinflammatory, antimicrobial, anti-parasitic activity as well as hepatoprotective effects ofGarcinia.However, none of these have translated into clinical practice or confirmed in randomized studies.Those endorsing the safety and efficacy ofGarciniauphold their beliefs on the basis of low quality studies[68].A randomized double-blind controlled trial onGarciniafailed to show significant change in fat mass and body weight compared to placebo, while a recent meta-analysis demonstrated an uncertain overall effect on long-term weight[69,70].A total of 24 case reports and 8 case series reporting adverse events among 66 patients afterGarciniaextract consumption was published in the literature.Of these, 17 studies out of 32 describe cases of acute liver injury, liver failure, and hepatotoxicity, observed among 50 patients consuming pureGarciniaor supplement mixtures.The latency period lasted from a few days to one year with continued ingestion in some patients.Two patients died, eight required liver transplantation, while one developed chronic DILI leading to cirrhosis[71,72].Hepatotoxic adulterants and contaminants such as high levels of chromium, cadmium, and thallium in marketedGarciniasupplements leading to acute liver injury have been reported in the literature[73].Garcinia cambogiahas been implicated in acute self-limiting hepatitis, as well as ALF requiring liver transplantation and progression to cirrhosis.Furthermore, poor manufacturing practices resulting in adulteration and contamination of proprietaryGarciniasupplements add to the hepatotoxic potential ofGarciniaindependently or synergistically.
Gymnema sylvestre (Cow plant or ”Gurmar”):Known as the ”sugar destroyer, ” this perennial woody climbing herb belonging to the milk-weed family is commonly used for treating diabetes mellitus.The most important phytochemical constituents include triterpene saponins, which are collectively called gymnemic acids, the polypeptide gurmarin, and the alkaloid conduritol.Gymnemic acid type A is the most potent hypoglycemic component, highly concentrated in the shoot tips and least in the seeds.Some of the alkaloids and saponins also act as appetite suppressants.Shiyovichet al[74]described the case of a 60-year-old female who developed severe acute hepatitis after consuming ”gurmar tea” for diabetes for one week.The work-up for other competing causes of acute hepatitis was non-contributory.The liver histopathology revealed lobular disarray with severe necroinflammatory changes in the hepatic lobules, marked ductular proliferation, and neutrophilic infiltration of portal areas.A short course of corticosteroids and ”gurmar” withdrawal resulted in complete resolution of symptoms[74].Gymnemais also one of the components of the well-described hepatotoxic herbal and dietary weight loss supplement, Hydroxycut®[75].Physicians caring for patients with DILI and patients with diabetes mellitus opting for additional alternative therapies must be made aware of the potential liver-damaging effects of herbs such asGymnema(Figure 7).
Tribulus terrestis (”Gokshura” / Goat’s head / Devil’s weed or Puncture vine):Tribulus terrestris(TT), a tap-rooted herb belonging to the caltrop family, is native to regions with a tropical climate.It is known to be a noxious weed with a woody prickly fruit.Its use in Ayurveda for impotence and sexual disorders, and its use as a dietary supplement among bodybuilders and athletes, stems from the belief that it increases testosterone level, has anabolic steroid properties, and improves muscle strength – efficacy that lacks scientific proof through quality studies.The main biologically active phytochemicals in TT are steroidal saponins (mainly protodioscin, prototribestan, and dioscin), flavonoids, Harman alkaloids and lignan amides.TT ingestion is known to produce tribulosis (renal and liver injury) associated with the accumulation of phylloerythrin and beta-carboline alkaloids in the blood of cattle.It also causes staggers (neuromuscular ataxia) and geeldikkop (cholestatic liver injury and bile cast nephropathy) in sheep[76].Talasazet al[77]described a 28-year-old man who, after ingesting ”Tribulus Water, ” developed severe liver (transaminases > 40 times the upper limit of normal) and kidney dysfunction, and seizures leading to hypertensive crisis and advanced azotemia due to acute renal tubular dysfunction requiring haemodialysis.After a stormy 2 wk hospital course, both liver and renal parameters improved, and the patient was discharged[75].Similarly, Ryanet al[78]described a young, healthy male who ingested TT herbal tablets for a few months as part of bodybuilding, who presented with severe jaundice and pruritus, followed by acute renal failure with bile-casts in the renal tubules on histopathology evaluation.A percutaneous liver biopsy showed only severe cholestasis, well-preserved hepatic lobules without inflammation supporting evidence for cholestasis-induced renal damage in the patient, possibly due to TT use[78].These reports shed light on the role of herb-induced non-serious liver injury, such as bland cholestasis indirectly leading to severe extrahepatic organ failure.

Figure 7 Acute cholestatic hepatitis due to Gymnema sylvestre (gurmar or sugar destroyer) herb.
Valeriana officinalis (Valerian):Valerian is an herbal root extract form ofValeriana officinalis, a perennial flowering plant growing in Europe and Asia.The name is derived from the Latin verb ”valere” meaning ”strong, healthy.” Valerian is known to contain multiple bioactive phytochemicals such as actinidine alkaloid, valerianine, valerene and, gamma-aminobutyric acid.It is used as an anxiolytic and sedative in Ayurvedic medicine.Potential mechanisms for sedation are not yet fully identified as phytochemicals such as valeric acid, and other root-specific components did not demonstrate sedative properties in experimental models.It is believed that valerenic acid by acting on the 5-HT5Aserotonin receptor modulates the sleep-wake cycle.The doubtful use of valerian as a sedative is underscored by a report on overdose in which the patient presented with mild symptoms that resolved within 24 h after consuming 20 times the recommended dose[79,80].Valproic acid is a derivative of valeric acid.A small number of case reports have showcased hepatotoxicity associated with valerian.MacGregoret al[81]were the first to report on the potential hepatotoxic effects of valerian in 1989 in a series of four patients, all of whom consumed over-the-counter sleeping pills that also included other herbs.The presence of Chinese skullcap was thought to be the major inciting agent in these patients, but caution was advised against using valerian-based herbal combinations[81].Cohenet al[82]described a young woman who developed self-limiting severe acute cholestatic jaundice after consuming capsules of valerian root extract 300 mg twice daily for 3 mo in the absence of other competing causes.Vassiliadiset al[83]described a 50-year-old woman with valerian extracts and tea consumption for 3 wk, after which she developed acute hepatitis.The liver biopsy showed mild portal fibrosis, lymphocytic, and eosinophilic inflammation of portal tracts, inflammatory changes of the small bile duct with ductular reaction and necrosis in the perivenular zone.Liver injury resolved after 10 mo on conservative management[83].In a study on herb-induced liver injury in the Berlin Case-Control Surveillance program, possible causality for valerian-induced DILI was notable in five (four females) patients.The liver injury was hepatocellular and cholestatic in type, and two patients developed jaundice.In two patients, biopsy revealed extensive necrosis while in one, it was perivenular (zone III) in nature, with all showing severe lobular and portal-based mixed type of inflammation.The disease course was self-limiting with symptom resolution and improvement of liver dysfunction on follow-up[84].In Figure 8 we illustrate the baseline and follow-up liver histopathology of a young woman who developed severe acute cholestatic hepatitis that progressed to chronic DILI and chronic liver disease at 6 mo follow-up, after consuming Indian valerian (Valeriana wallichi) root extract (Tagara®, The Himalaya Drug Company) for three to seven days.A summary of all discussed Ayurvedic herbs and their hepatotoxic details is shown in Table 1.
CONCLUSION
Ayurvedic herb-related hepatotoxicity and liver injury can present as asymptomatic minor transaminase elevations, acute and chronic hepatitis, granulomatous hepatitis, asymptomatic to severe cholestasis, sinusoidal obstruction syndrome, acute liver failure requiring transplantation as well as progression to cirrhosis and portal hypertension.It is essential that physicians and specialists caring for patients with acute and chronic liver disease understand the small, but central role of herb-induced liver injury in a subset of patients who follow complementary and alternative medical practices and in whom an etiology of liver disease cannot be ascertained after extensive and conventional evaluation.The type of herb-induced liver injury and knowledge of its natural course is also important for treatment decisions and prognostication.Further studies that focus on the identification of beneficial and toxic components in Ayurvedic herbs, regulated curbing on the use of polyherbal formulations and educating the masses through public-industry partnerships, on the potential severe toxicity of certain herbs remain an unmet need.

Table 1 A summary of all Ayurvedic herbs implicated in liver injury with potential mechanisms of toxicity, liver injury pattern, histopathology patterns and clinical outcomes

hepatotoxicity described Yellapu et al[30]/report/United States Hepatocellular type Massive hepatic necrosis Acute liver failure necessitating cadaveric liver transplantation Polavarappu et al[31]/report/United States Hepatocellular type Not performed Spontaneous resolution on drug withdrawal loss supplements)Dalal et al[32]/report/United States Hepatocellular type Mixed portal inflammation, interface hepatitis, eosinophilic lobular inflammation with ceroid laden macrophages Spontaneous resolution on drug withdrawal Nam et al[34]/report/South Korea Mixed type Zone 3 necrosis, cholestasis and severe mixed inflammatory infiltration of lobules Terpenoids like bakuchiol and coumarinoids Complete clinical resolution Cheung et al[35]/series (n = 3)/Hepatocellular type Not performed All three patients had uneventful recovery after drug withdrawal Psoralea corylifolia (Bakuchi, Babchi seeds)Smith et al[36]/report/United Kingdom Hepatocellular type Cholestatic acute hepatitis Clinical resolution on drug withdrawal Beuers et al[41]/report/Germany Mixed type Perivenular necrosis, lymphohistiocytic portal and lobular inflammation Anthracoid sennoside and rhein anthron metabolites Complete resolution, recurrence on rechallenge Sonmez et al[42]/report/Turkey Mixed type Bridging hepatocellular necrosis and canalicular cholestasis Complete resolution Seybold et al[43]/report/Germany Hepatocellular type Not performed Complete resolution Cassia angustifolio (Indian Senna)Vanderperren et al[44]/Belgium Hepatocellular type Not performed High amounts of cadmium on toxicology evaluation Acute liver failure with renal failure, resolved on aggressive supportive care Rabe et al[52]/report/Germany Cholestatic type Portal and lobular lymphoplasmacytic inflammation, eosinophilic granulomas, bridging necrosis and bilirubinostasis Aloe alkaloids, anthraquinones Complete resolution on herbal drug withdrawal Parlati et al[53]/report and review series (n = 9)/France Hepatocellular type All patients had portal and lobular inflammation with neutrophils and lymphoplasmacytes along with granulomas, acidophil bodies, ballooning of hepatocytes, extensive bridging necrosis and bilirubinostasis All cases had clinical resolution of symptoms, no acute liver failure and no chronicity noted on follow up Manso et al[56]/series on Herbalife® products/Spain Hepatocellular type Cholestatic hepatitis Complete resolution after supplement withdrawal Aloe vera Vázquez-Fernández et al[57]/report/Spain Cholestatic type Cholestatic hepatitis with lymphocyte predominant portal inflammation Acute decompensation of cirrhosis (underlying HCV related infection); outcome not reported Millonig et al[59]/report/Austria Hepatocellular type Severe mixed inflammatory infiltration of portal tracts with lobular eosinophilic inflammation and hepatocellular cholestasis in zone 3 Suspected noni anthraquinones Complete resolution on herbal medicine withdrawal Stadlbauer et al[60] / two cases report/Austria Both cases hepatocellular type First case, confluent necrosis, second case centrilobular necrosis and mild inflammatory infiltration in both First patient progressed to acute liver failure and underwent successful liver transplantation; second patient had complete clinical recovery on conservative care Acute hepatitis with portal inflammation and periportal necrosis, Paediatric case (14-year-old boy) with Morinda citrifolia (Noni juice)Yu et al[61]/report/United States Hepatocellular type

HCV: Hepatitis C virus; DILI: Drug-induced liver injury.

Figure 8 Development of acute severe cholestatic hepatitis leading to chronic herb-induced liver injury resulting in cirrhosis in a young female, after ingestion of Valerian (Tagara®).
杂志排行
World Journal of Hepatology的其它文章
- Clinical implications, diagnosis, and management of diabetes in patients with chronic liver diseases
- Biomarkers for hepatocellular cancer
- N-acetylcysteine and glycyrrhizin combination: Benefit outcome in a murine model of acetaminopheninduced liver failure
- Transaminitis is an indicator of mortality in patients with COVID-19: A retrospective cohort study
- Clinical efficacy of direct-acting antiviral therapy for recurrent hepatitis C virus infection after liver transplantation in patients with hepatocellular carcinoma
- Surgical treatment of gallbladder cancer: An eight-year experience in a single center