Comparison of the modified Wiltse's approach with spinal minimally invasive system and traditional approach for the therapy of thoracolumbar fracture
2020-11-11JieChangJiangCaoZiyanHuangBoyaoWangTaoSuiXiaojianCao
Jie Chang, Jiang Cao, Ziyan Huang, Boyao Wang, Tao Sui, Xiaojian Cao
Department of Orthopedics, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu 210029,China.
Abstract Thoracolumbar fractures are usually treated by open posterior pedicle screw fixation. However, this procedure involves massive paraspinal muscle stripping, inflicting surgical trauma, and prolonged X-ray exposure. In this study, we observed 127 patients with single-segment injury thoracolumbar fractures. Thirty-six patients were treated by the modified Wiltse's paraspinal approach with minimally invasive channel system, while 91 patients were treated via traditional posterior approach. Operation time, intraoperative blood loss, intraoperative fluoroscopy frequency, screw placement accuracy, visual analogue scale score, and Cobb's angle of two groups were compared. The X-ray exposure times were notably reduced (4.2±1.6) in the new approach group (P<0.05).The pedicle screw placement accuracy and Cobb's angle after surgery were similar in the two groups. We conclude that modified Wiltse's paraspinal approach with spinal minimally invasive channel system surgery can significantly reduce the X-ray exposure times and is an alternative therapy for the thoracolumbar fracture.
Keywords: thoracolumbar fracture, Wiltse's paraspinal approach, spinal minimally invasive channel system
Introduction
Thoracolumbar fracture is one of the most common orthopedic diseases[1-3]. Conservative treatment of thoracolumbar fractures requires prolonged bed rest,which can cause severe kyphotic deformities and even secondary spinal nerve injuries[4]. In addition, patients who underwent conservative treatment experience poor quality of life and high nursing costs. The pedicle screw system, especially the minimally invasive internal fixation surgery, enables faster recovery of the after internal fixation and patients can immediately resume their normal activities of daily living[5].
The traditional surgical method is called the open pedicle screw rod reduction and internal fixation through the posterior median approach[6]. However,this method increases the risk of exposure, bleeding during the surgery, damage to the paravertebral soft tissue, and duration of fluoroscopy[7-10].
Large-scale soft tissue dissection during surgery increases surgical trauma, increases the amount of bleeding, weakens the soft tissue protective barrier around the lumbar spine, and affects the lumbar spine stability. As a result, there may be continuous pain in the lower back after surgery, and accelerated degeneration of the lumbar spine at the surgical segment and adjacent segments. In addition, large amounts of X-ray exposure may have an adverse impact on human health. Radiation exposure during radiology, cardiology and orthopedic surgery can increase the risk of dermatitis, cataract, and cancer[11-12].
In 1968, Dr. Wiltse first described a new approach that was involved splitting the muscles between the multifidus and longissimus to retain the integrity of the posterior osseous structure and the posterior ligamentous complex to the maximum extent[13-16]. He later made refinements in the paraspinal approach so that it could be applied to other lumbar diseases[17].This approach could help surgeons reach the intervertebral foramen, transverse process, and other surgical areas accurately with less paravertebral muscle dissection and less traction. Compared with the traditional approach, the Wiltse's approach requires a shorter incision length, less soft tissue injury, and has a faster recovery[18-19]. However, because the multifidus is well-developed, especially in the lower lumbar, it is difficult to expose the operative field using the ordinary spinal surgical instruments.Furthermore, the pressure of the multifidus increases due to traction and compression, which may cause irreversible damage such as necrosis and atrophy.
Controlling the intraoperative damage, a new surgical method was developed to reduce the radiation exposure, the modified Wiltse's paraspinal approach combined with spinal minimally invasive channel system surgery. Our spinal minimally invasive channel system surgery could allow adequate exposure of the surgical site, minimize muscle damage and simplify the surgery with the use of Wiltse's paraspinal approach. Moreover, we found the regular pattern of the angle between the screw and the supraspinal ligament[20]. All of these could help accurately implant the screw and reduce the use of Carm fluoroscopy. In this study, we aimed to review 3 years of clinical cases to assess whether the new approach is advantageous than the existing traditional surgical methods.
Materials and methods
Introduction of spinal minimally invasive channelsystem
The spinal minimally invasive channel system consists of an outer hook and an inner hook.
Outer hook
The outer hook has a double-head design, which can rotate with any head as fulcrum during surgery,and the other head can be used to expose the surgical site. As the traditional hook can easily compress the surrounding tissues and cause damage, our hook handle joint is designed as "fish mouth" to avoid this damage. The angle was made between the handle and the pull hook to ensure that the part holding the handle remains in an upright position to reduce the influence of the tissue around the incision on the placement of the pull hook. The lateral edge of the lamina was designed as a "double lingual process", so that the local lamina can be easily exposed during surgery, and the contact between the hook and the lamina will remain stable (Fig. 1A and B).
Inner hook
The inner hook was designed to create a small incision and was based on the local bone anatomy. It can easily pull the multifidus muscle to the inner side,is convenient to use, and can be easily adjusted.Traditional surgery required to the removal of the surrounding soft tissue to expose the location of nail placement. Based on the anatomical characteristics of the lumbar facet joints, the distal end of the medial lamina hook has an "arc concave crescent shaped",which can avoid damage to the surrounding soft tissue and bone structure and can easily expose the nail area.An obtuse angle was made between the handle and the pull hook to ensure that the part holding the handle remains in an upright position to reduce the influence of tissue around the incision on the placement of the pull hook. Moreover, according to the patient's body shape and individual needs during the surgery, the hooks have various depths and angles (Fig. 1C and D).
Patients and study design
A total of 127 patients (73 men and 54 women;aged from 19 to 73 years) with thoracic and lumbar vertebral fractures without neurological symptoms who underwent pedicle screw fixation between January 2015 and December 2017 in the First Affiliated Hospital of Nanjing Medical University were selected. Of them, 36 were treated using the modified Wiltse's paraspinal approach and the remaining were operated using the traditional approach. All patients had a fresh single-level thoracolumbar compression fracture 2 weeks prior to surgery. They had a thoracolumbar injury severity score of equal to or less than four. The demographics and clinical characteristics of the patients are shown inTable 1. The procedure was approved by the ethical committee of the First Affiliated Hospital of Nanjing Medical University. The digital radiography,computed tomography, and magnetic resonance imaging scans of all patients were assessed to provide an accurate diagnosis. We divided the patients into two groups for determining the effective surgical option of the two approaches. Group A consisted of 36 patients who underwent surgery using the spinal minimally invasive channel system, while group B underwent traditional pedicle screw fixation. The operations of the two groups were separately performed by a single senior surgeon.
Table 1 Patients' baseline data

Fig. 1 Spinal minimally invasive channel system. A and B: Outer hook; C and D: Inner hook.
New surgical procedure
Group A patients were treated by the modified Wiltse's approach with the help of the spinal minimally invasive channel system. All procedures were performed under general anesthesia in the prone position. The fracture site was confirmed using a radiograph, and the entry point was set. A posterior midline incision or several paramedian incisions were made, and the integrity of the supraspinous ligament and interspinous ligament were explored after the deep fascia was opened. A posterior midline incision was used for obese or muscular young individuals to prevent fat liquefaction and excessive bleeding, as we found longer incision was required for these patients to adequately expose the operative field. The intermuscular spatium between the medial multifidus and lateral longissimus muscles was bluntly separatedviathe Wiltse's approach[17], exposing the bilateral articular processes and transverse processes of the fractured vertebra, and the adjacent vertebrae. The entry point to the pedicle was easily exposed by the spinal minimally invasive channel system between the lateral border of the superior articular processes and the bisecting line of the transverse process. The angle was set at 90 degrees, keeping the trajectory of the screw perpendicular to the supraspinal ligament[20].Pedicle screws were then inserted into the adjacent vertebra above and below the fractured vertebral body.A shorter pedicle screw was inserted into the bilateral or unilateral pedicles of the fractured vertebra. The spinal minimally invasive channel system was used throughout the process of screw implantation (Fig. 2andFig. 4).
Traditional surgical procedure
Group B patients were treated using the traditional surgical approach. All procedures were performed under general anesthesia in the prone position. The fracture site was confirmed by C-arm fluoroscopy, and the entry point was set. A midline incision was made.The paraspinal muscle was separated to expose the supraspinatus and interspinous ligaments. The bilateral articular processes and transverse processes of the fractured vertebra were exposed using the help of the toothed retractor or other routine hooks. Pedicle screws were then inserted into the fractured vertebra,along with the adjacent vertebra after consideration.
Observation index
Preoperative, postoperative, and follow-up radiographs were evaluated to determine the success of the surgery. The frequency of X-ray fluoroscopy use,sagittal Cobb's angle, the accuracy of pedicle screw insertion, visual analogue scale (VAS), intraoperative bleeding, surgical duration, and length of postoperative hospital stay were determined to evaluate the efficacy of fracture-level screw incorporation in patients. The frequency of radiographs was measured every time when deciding the location of incision, determining the fractured vertebra before implanting screws, and determining the location of the positioning needles or screws after implantation. Carm fluoroscopy was performed ones, while lateral and frontal views of X-rays were counted twice. The sagittal Cobb's angle between the superior endplate of the upper and the inferior endplate of the lower vertebrae was measured.
Statistical analysis
The Prism 5 statistical software (GraphPad Software, USA) was used to perform all statistical analyses. Data were expressed as mean±standard deviation (SD). Count data were expressed as rate (%)and compared using the chi-square test. The VAS score, vertebral compression degree, and other data were compared using thet-test. APvalue of <0.05 was considered significantly.

Fig. 2 Preoperative, postoperative, and follow-up radiographs of the patients who underwent surgery using the spinal minimally invasive channel system. A and B: X-ray results prior to surgery; C and D: X-ray results 3 days after surgery; E and F: X-ray results 3 months after surgery.
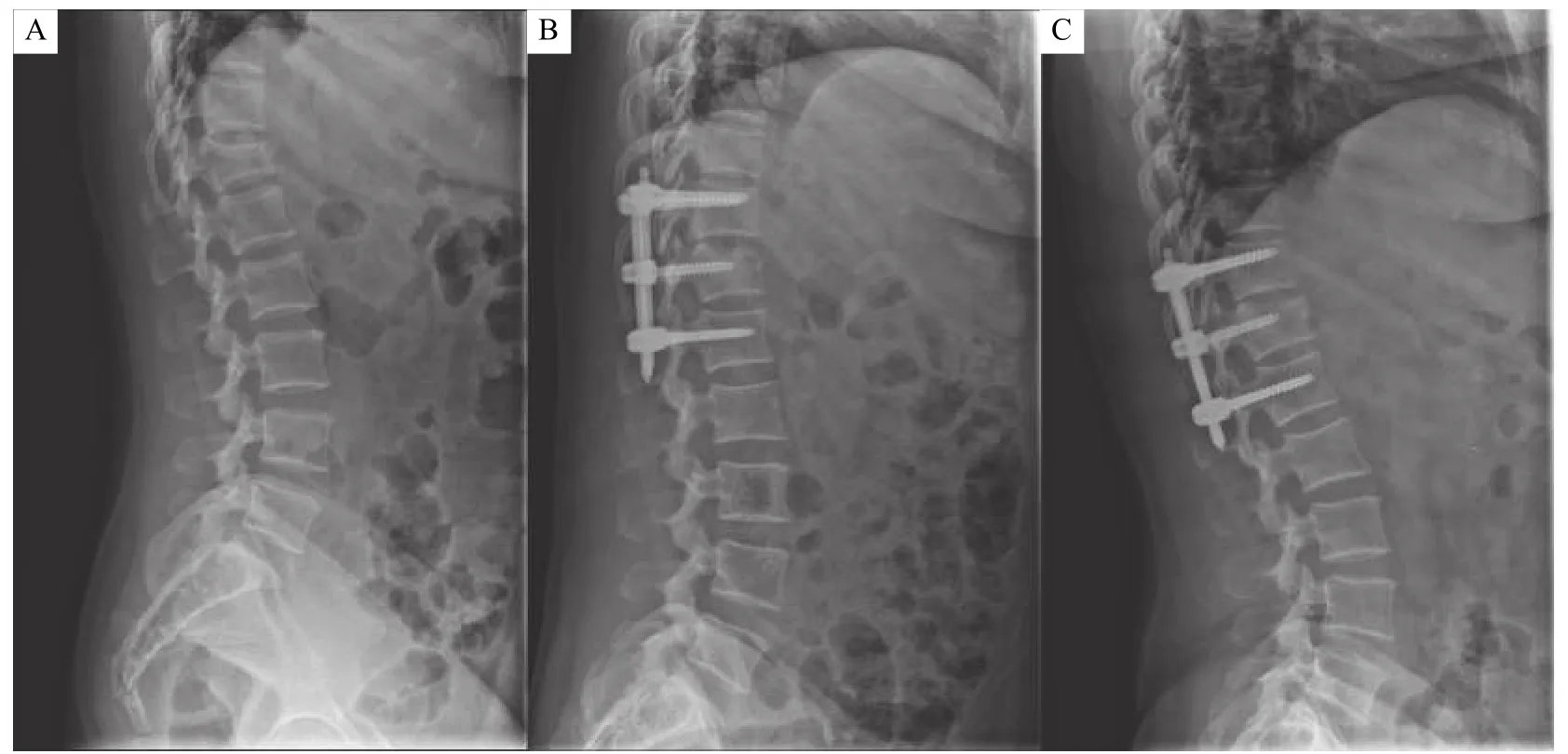
Fig. 3 Preoperative, postoperative, and follow-up radiographs of Cobb's angle. A: Cobb's angle prior to surgery; B: Cobb's angle 3 days after surgery; C: Cobb's angle 3 months after surgery.
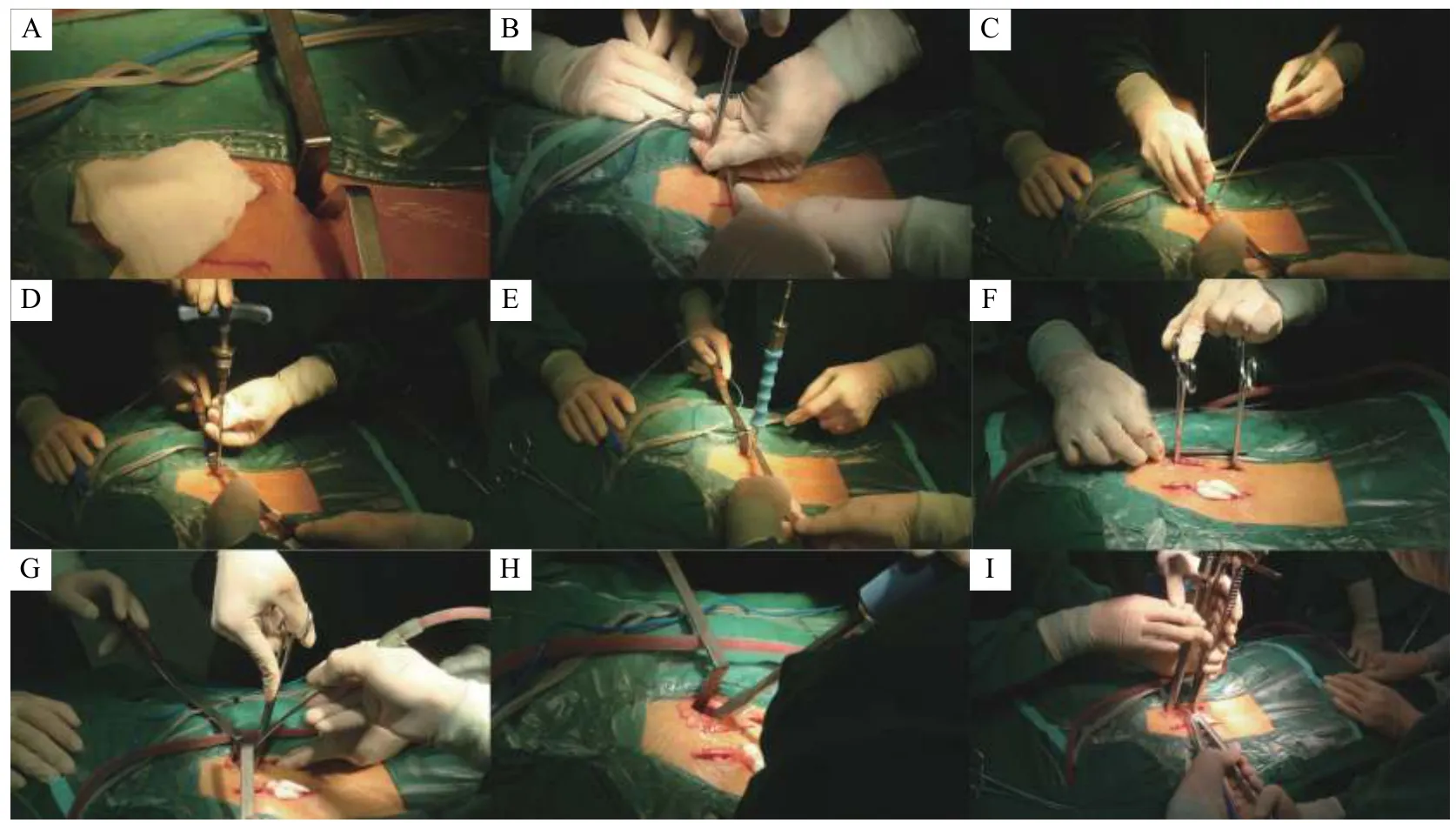
Fig. 4 Procedure of modified Wiltse's paraspinal approach combined with spinal minimally invasive channel system A-E: Inserting pedicle screws. F-I: Inserting the rod and distracting the vertebra.
Results
Patients
A total of 127 patients were included in this study.The baseline clinical characteristics of the study participants are listed inTable 1which summarizes the demographic data. The mean age of the new channel system group (group A) was (47.8±14.2)years, while that of the traditional group (group B) was(51.9±11.6) years. Group A comprised 23 men, while group B comprised 50 men. There was no significant difference in sex and age between the two groups.
Outcome measure
There was a significant difference in X-ray exposure times between the two groups (P<0.01). The new channel system group underwent radiographic evaluation 4.2 times [95% confidence interval (CI),2.6-5.8], while the traditional group underwent X-ray 6.0 time (95% CI, 3.9-8.1). Group A had the surgical duration of 120.8 minutes (95% CI, 82.1 -159.5),which was similar to that of group B (121.2 minutes;95% CI, 80.3-162.1;P=0.96).
The accuracy rate of pedicle screw insertion in the new channel system group (97.4%, CI 90.0% to 100%) was similar to that in the traditional group(97.9%, CI 91.5% to 100%) (Table 2). The Cobb's angle in the two groups was measured before, after,and 3 months after surgery (Table 3andFig. 3). The preoperative VAS scores of the two groups had no significant difference (P>0.05). The postoperative VAS scores of the two groups were significantly different as compared to the preoperative scores(P<0.05) (Table 4). Three patients of the traditional group experienced surgical complications. All of them developed infection at the incision site, which eventually healed after receiving an anti-infective treatment.

Table 2 Clinical findings
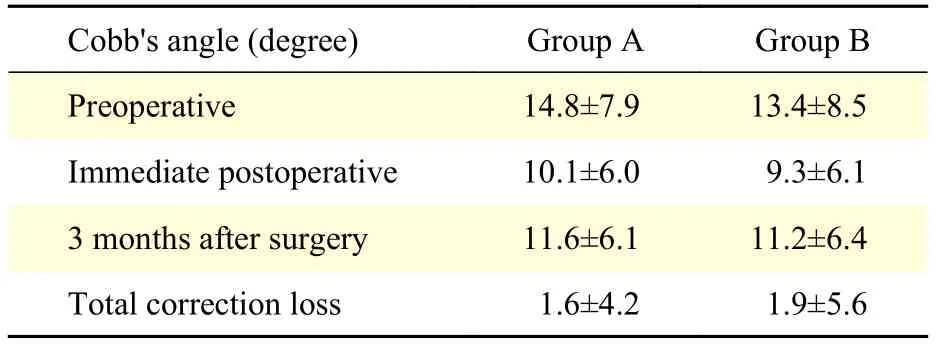
Table 3 Changes in radiological findings
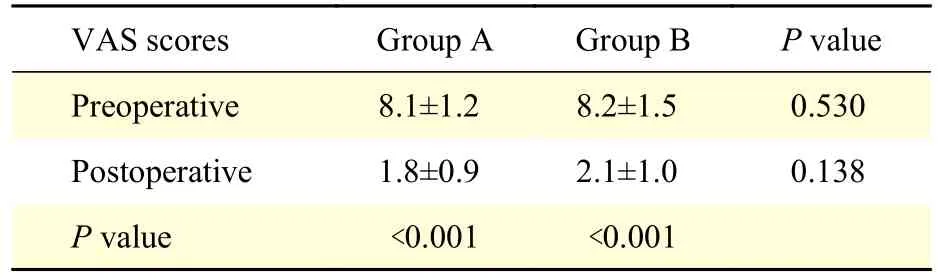
Table 4 VAS scores of the two groups
Discussion
The conventional posterior approach has been considered a classical method for the treatment of thoracolumbar fracture with satisfactory clinical outcomes. However, the traditional open posterior surgery requires massive stripping of the paraspinal muscle to expose the spinous process, lamina, and facet, followed by a short-segment or long-segment internal fixation[21]. Stripping of the paraspinal muscles is usually the primary cause of ischemia,necrosis and denervation of the paraspinal muscle,resulting in atrophy and contractile property loss of the paraspinal muscles postoperatively[10,22-23]. Therefore,in recent years, minimally invasive techniques have been widely used in spine surgery[24-25].
Minimally invasive spine surgery became increasingly popular during the past several years.Less invasive surgery requires substitution of the typical tactile and visual feedback that is used during open surgery for navigation with some form of imageguided navigation[26]. Consequently, the number of healthcare workers, especially operators, exposed to low-dose ionizing radiation has increased. The biological effects of low levels of radiation have been investigated and debated for more than a century.Some studies suggest that it is unlikely to directly and precisely quantify the risk of cancer at low doses[27],while others believe that fluoroscopy is associated with malignancies, skin problems[11,28]and cataracts[29-30].
Our screw placement relied less on intraoperative fluoroscopy than the placement of traditional open surgery. Surgeons should wear lead aprons, thyroid shields, and leaded glasses, since surgical techniques can increase radiation exposure to surgeons[31]. Spinal surgery, especially percutaneous pedicle screw placement, is considered safe; the use of lead aprons during this surgery protects surgeons from radiation exposure. However, the use of lead aprons, thyroid shields, and leaded glasses is often neglected. Wearing full protection is needed to reduce the surgeon's exposure to radiation exposure of the surgeon.Furthermore, the spinal surgeon frequently has to hold the instrument during fluoroscopic imaging, thereby placing the hands at the risk of exposure[32].
Our custom-made channel system, the spinal minimally invasive channel system, consists of two types of hooks, the outer hook and the inner hook[33].The outer hook is a double-headed design, which can be easily rotated with either head as a fulcrum during the surgery, and the other end can easily expose the operative site. The inner hook can pull the multifidus muscle to the inner side, which is convenient to use and adjust. Through the combined application of the two hooks, we can minimize the incision length and tissue damage, which is a great improvement in the field of minimally invasive surgery under the premise that the needle point is fully exposed. Furthermore,our new free-hand pedicle screw placement technique could also help reduce the use of C-arm. We detected the angle between the upper vertebral endplate and the supraspinal ligament and found a regular pattern: the angle from T1 to L4 was about 90° and 80° of L5[20].This technology can assist in evaluating the position of the screw during radiographic evaluation and confirm its position (lateral and frontal) at the end of the surgery. As a result, radiographic evaluation will be needed only four times, when deciding the incised location, determining the fractured vertebra before implanting screws, and determining the position of screws and rod (lateral and frontal) before suturing the incision. In this study, C-arm was performed in the new channel system group only 4 times. No complications occurred in 36 patients, who underwent a combination of minimally invasive surgery with the new channel system.
In our study, monoaxial pedicle screws were used in the two groups, which sufficiently restored the sagittal Cobb's angle sufficiently. As monoaxial pedicle screws showed greater stability in flexion and extension than that of polyaxial pedicle screws[34], this type of screw was successfully applied to the new channel system group. Each patient was placed on the operating table in a prone position with cushions under the iliac crests and thorax to perform postural exercises. Supine postural reduction was also performed prior to surgery if required.
The new channel system approach showed similar effect in terms of improving and maintaining the Cobb's angle, accuracy of screw placement, and relief of pain compared with traditional approach.Therefore, the new channel system approach was effective in the treatment of thoracolumbar fractures.The limitations of this study should also be noted.First, the new approach can only be performed in the lumbar and thoracic fractures. Patients with severe lamina fractures that have entrapped the dural tissue or neural elements cannot be treated by this approach. In addition, the number of patients included in the new channel group were less for optimal statistical analysis. Moreover, a valid conclusion should be drawn when evaluating cases that require a longer follow-up.
In conclusion, our new surgical method was successfully applied in patients with the thoracolumbar fractures without neurologic deficits.Compared with the traditional approach, it notably decreased the duration of X-ray exposure, which is beneficial for patients and spine surgeons. It also reduced surgical trauma with a lower incidence rate of related complications and achieved similar or even better clinical outcomes.
Acknowledgments
This work was financially supported by the National Natural Science Foundation of China (Grant No. 81672152 and No. 81871773) and the Jiangsu Natural Science Foundation (Grant No. BE2018132).
杂志排行

THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- Postprandial dyslipidemia in insulin resistant states in adolescent populations
- TIR/BB-loop mimetic AS-1 protects vascular endothelial cells from injury induced by hypoxia/reoxygenation
- Cofilin participates in regulating alpha-epithelial sodium channel by interaction with 14-3-3 isoforms
- Cumulative live birth rates of in vitro fertilization/intracytoplasmic sperm injection after multiple complete cycles in China
- Exposure to environmental bisphenol A inhibits HTR-8/SVneo cell migration and invasion
- Pre-evaluation of humoral immune response of Bactrian camels by the quantification of Th2 cytokines using real-time PCR