Post-cholecystectomy bile leak is not always synonymous with acute bile duct injury: Need for reclassification
2020-10-23VishalGupta
Vishal Gupta
Department of Surgical Gastroenterology, King George’s Medical University, Lucknow, UP 226003, India
TotheEditor:
Bile leak after laparoscopic cholecystectomy remains a significant cause of postoperative morbidity.Cystic duct stump is the most common site (~70%) of bile leak after cholecystectomy [1].Incidence of bile leak from the cystic duct stump is 0.5% −3% which is higher (4% −7%) in cases with complicated gallstone disease (e.g.acute cholecystitis) [2].
Bile leak in postoperative period after cholecystectomy, manifesting as bile in intraoperatively placed drain or as an intrabdominal collection, localized or generalized, is considered a complication secondary to bile duct injury (BDI) that was sustained during the procedure.Irrespective to the site of leak, such bile leak is classified as an iatrogenic BDI, and is subsequently categorised depending on the site of leak if that is localized on subsequent investigations.
Bile leak from the cystic duct stump has been considered an iatrogenic BDI when the attention was drawn to higher BDI incidence noted after the introduction of laparoscopic cholecystectomy.It has been described under different classification systems for iatrogenic BDI.Cystic duct stump leak has different classification system, and it is mostly described as type A injury in Strasberg [3]and Amsterdam Academic Medical Center [4]classifications, subcategory type A1 in Neuhaus [5]and Hannover [6]classifications, type 1 in Lau [7]and Siewert [8]classifications, type II in Csendes classification [9], insignificant injured duct with bile leak in Kapoor classification [10], grade 1 in Cannon classificat ion [11], and non-main biliary duct (NMBD) injury in the most recent anatomic, time of detection, mechanism (ATOM) nominal European Association for Endoscopic Surgery classification[12]( Table 1 ).
Is cystic duct stump bile leak really an injury?
Based on the following points it can be argued that bile leak from the cystic duct stump should be considered only a complication of cholecystectomy, not an injury as has been referred to in various existing classification systems ( Table 1 ).
First, during laparoscopic cholecystectomy, cystic duct is secured with a variety of techniques, e.g.non-locking metallic clips(most common), locking absorbable or nonabsorbable clips, suture closure, and energy devices closure using Harmonic scalpel (Harmonic ACE, Ethicon Endo-Surgery) and LigaSure [2].Current evidence suggests cystic duct stump leak rate of 0-4% with a pooled leak rate of 0-1% with each of these techniques [2].This suggests that despite secured closure of the stump, there is an inherent risk of bile leak, albeit very low, from this stump which becomes higher in the presence of acute inflammation leading to edematous duct when the clip may dislodge once edema settles down.Other causes that may lead to such leak include insecure closure of the cystic duct, necrosis of the stump, slippage of ligature, or stump blowout due to raised upstream ductal pressure due to distal obstruction by the stone in the common bile duct with an incidence as high as 20% [1].All these mechanisms have been described as being responsible for type A/type 1/grade 1 BDI.
Second, bile leak after subtotal cholecystectomy is also common(18%) [13].Subtotal cholecystectomy is resorted to as a bailout option in a difficult situation to prevent BDI.If bile leak from the gallbladder stump (or from left open cystic duct opening in cases of fenestrating subtotal cholecystectomy) is taken as BDI, this bailout strategy would be considered a risk factor for BDI rather than being a protective strategy.Although this strategy may avert major BDI but still would be associated with an unusually (apparently)high overall rate of BDI.
Third, the term “injury”has more sinister connotation specially in the context of cholecystectomy.Labeling a complication arising out of an injury sustained during surgery has more potential for litigation than a complication developing in the absence of any intraoperative injury.Bile leak from the cystic duct stump can be compared with certain other scenario in abdominal surgeries.Duodenal stump blowout after Billroth-II gastrectomy, pancreatic stump leak leading to pancreatic fistula after distal pancreatectomy, blowout of rectal stump after Hartmann procedure are surgical complications which have never been labeled as injury but are always considered to be postoperative complication irrespective of underlying mechanism of such complication (e.g.technical reasons, distal obstruction or difficult duodenum/rectum).In fact,mechanisms involved in these scenarios are similar to mechanisms involved in the cystic duct stump leak.Similarly, bile leak or subsequent development of stricture after primary closure of choledo-chotomy done for common bile duct exploration cannot be considered BDI [12].
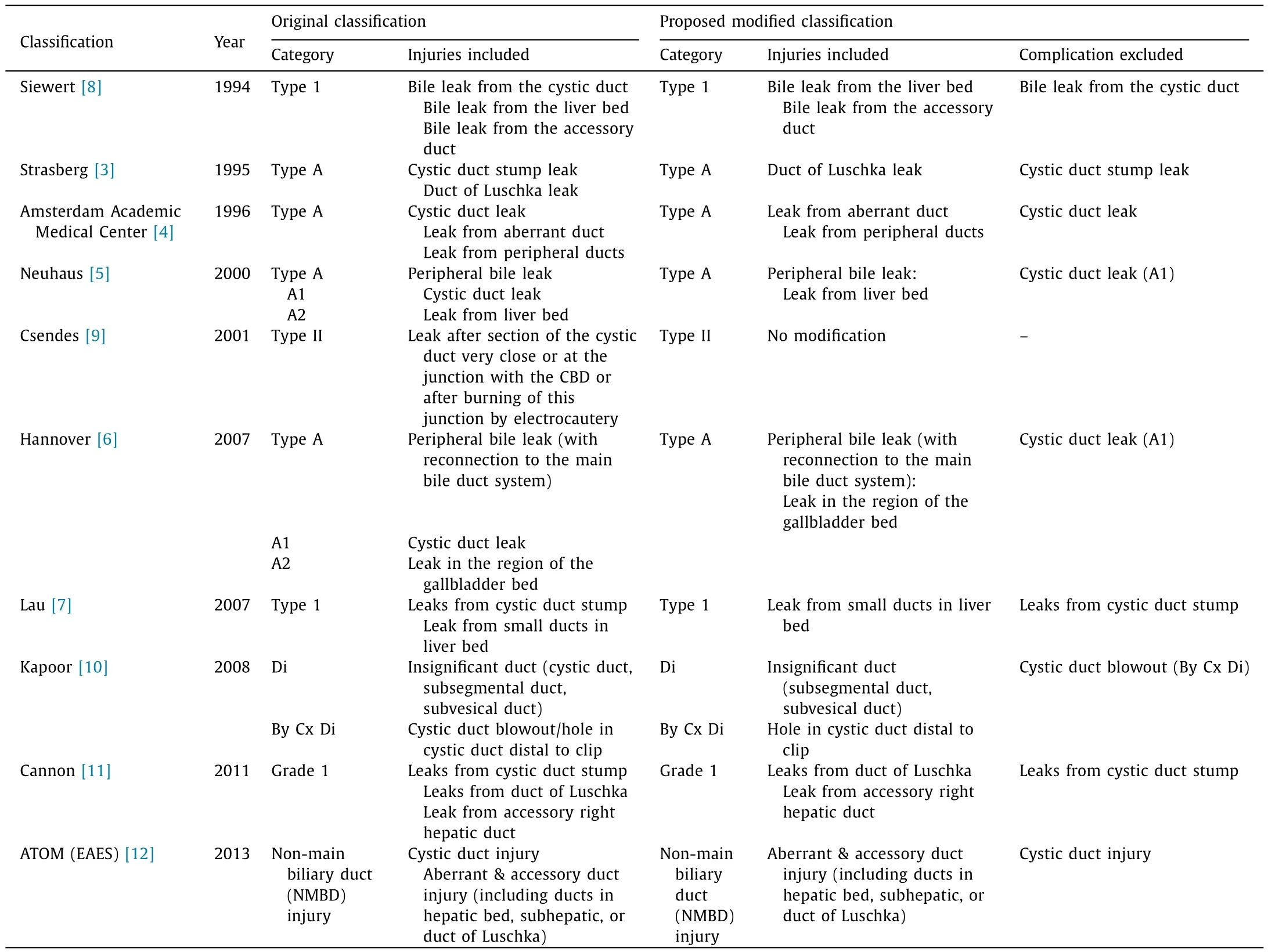
Table 1Existing classifications of post-cholecystectomy bile duct injury with respect to the cystic duct leak and their proposed modification.
Argument for not considering bile leak from the cystic duct stump a BDI has been made early in 2004 [14]and has been discussed in ATOM classification although it was still included as BDI in ATOM, latest, classification system [12].Connor and Garden [15]in their review in 2006, briefly mentioned this point,and suggested to consider cystic duct leak a complication because of low long-term morbidity and mortality.
While leak from the cystic duct stump after its avulsion (uncontrolled division) at origin (from the gallbladder) or at insertion(from the hepatic duct) or at any point in between due to excessive traction or in the presence of acute inflammation may be considered a BDI, bile leak from the well secured cystic duct (irrespective of its mode of closure), specially after achieving the critical view of safety, should be considered just a complication.It would be inappropriate to label this as an injury.
It would be appropriate to include all biliary adverse events as “biliary complications”after cholecystectomy ( Fig.1 ).These biliary complications include both bile leak and biliary stricture.Bile leak from the cystic duct stump after total cholecystectomy and from the gallbladder stump after subtotal cholecystectomy should be considered only as a complication, not an injury.Bile leak from other parts of the biliary system (end leak or side leak), including from the aberrant duct, and stricture is true BDI.Based on this, modification of existing classification systems is proposed as shown in Table 1.
To conclude, bile leak after cholecystectomy does not always result from BDI.Bile leak from the cystic duct stump is not an injury.This complication should be excluded from all current (and future) classification systems for the iatrogenic BDI as its underlying mechanisms are totally different from those responsible for other iatrogenic BDI and because of the medicolegal implications of term “injury”.
Acknowledgments
None.
CRediT authorship contribution statement
Vishal Gupta:Conceptualization, Writing - original draft, Writing - review & editing.
Funding
None.
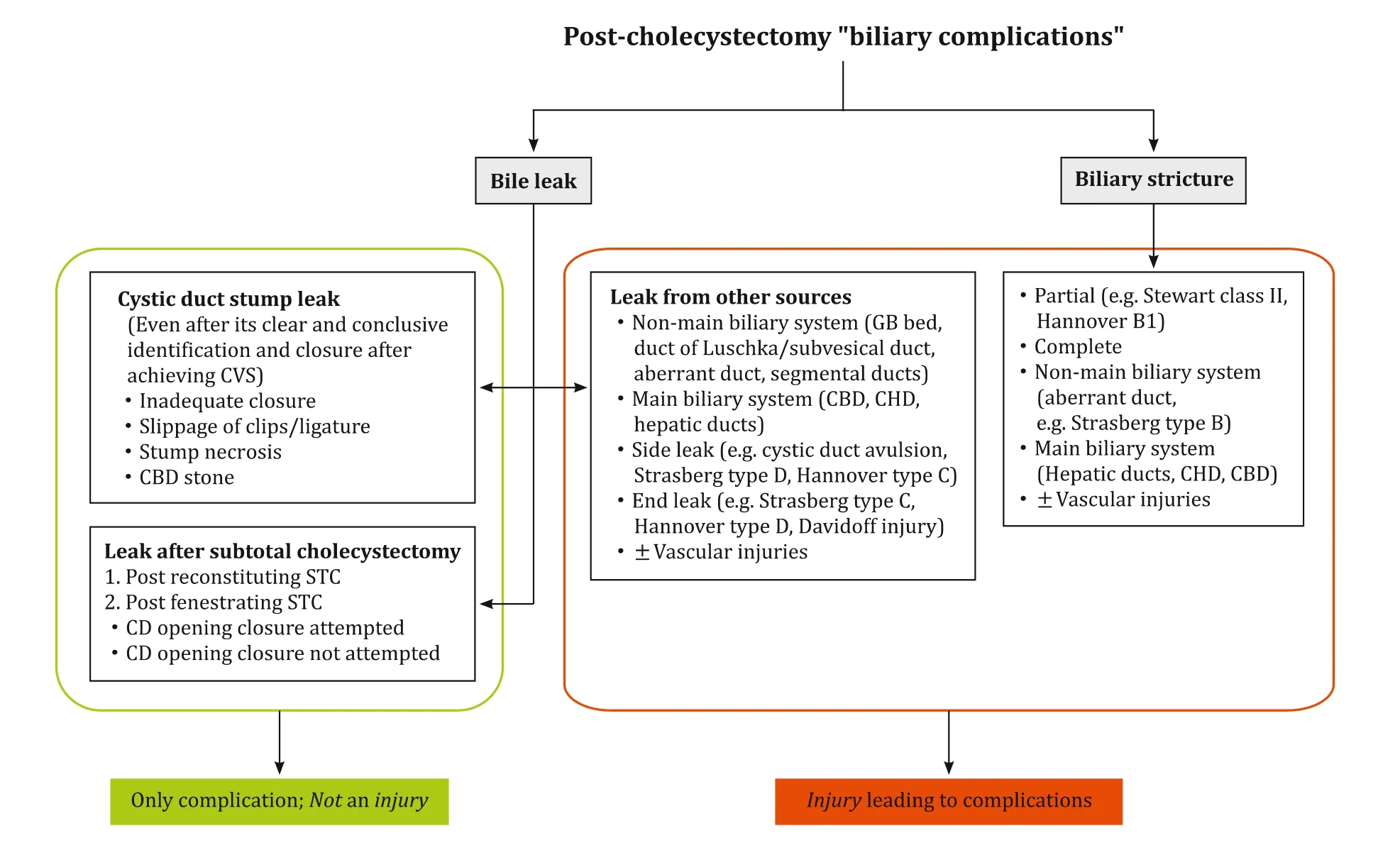
Fig.1.All post-cholecystectomy biliary adverse events are combined as “biliary complications”which consists of two defined groups of bile leak and biliary stricture. Not all bile leaks result from biliary injuries.CVS: critical view of safety; GB: gallbladder; CBD: common bile duct; CHD: common hepatic duct; STC: subtotal cholecystectomy;CD: cystic duct.
Ethical approval
Not needed.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Hepatobiliary&Pancreatic Diseases International
- No difference in mortality among ALPPS, two-staged hepatectomy, and portal vein embolization/ligation: A systematic review by updated traditional and network meta-analyses
- Telomerase reactivation is associated with hepatobiliary and pancreatic cancers
- Critical role of estrogen in the progression of chronic liver diseases
- Robotic isolated partial and complete hepatic caudate lobectomy: A single institution experience
- C -C motif chemokine ligand 16 inhibits the progression of liver cirrhosis via inactivating hepatic stellate cells