Composite hepatocellular and hemangiosarcomatous tumor: The prognosis is determined by the sarcomatous component
2020-05-10GiuseppeOrlandoQuirinoLaiJanLerut
Giuseppe Orlando , Quirino Lai , Jan Lerut
a Department of General Surgery, Wake Forest University School of Medicine, Winston-Salem, NC, USA
b Wake Forest Institute for Regenerative Medicine, Wake Forest University School of Medicine, Winston-Salem, NC, USA
c Starzl Unit of Abdominal Transplantation, Pôle de Chirurgie Expérimentale et Transplantation, Institute of Experimental and Clinical Research [IREC],Université catholique de Louvain, Brussels, Belgium
d Department of General Surgery and Organ Transplantation, Sapienza University of Rome, Rome, Italy
Nowadays, mixed liver tumors are more frequently diagnosed due to better imaging, advanced immunohistochemistry (IHC)staining techniques and better knowledge of hepatic tumorigenesis [1-3] . Such tumors represent a mosaic of components with distinct histogenesis and carcinogenic pathways. As their occurrence in the liver is very rare, their behavior and natural history are difficult to determine, and their management remains empirical.An uncommon case of a composite tumor harboring hepatocellular carcinoma (HCC) and hepatic hemangiosarcoma (HHS) components in a liver transplant (LT) recipient is reported herein.
A 65-year-old man was diagnosed with Child-Turcotte-Pugh B cryptogenic cirrhosis complicated with a two-cm wellencapsulated nodule in segment IV. Serum alpha-fetoprotein(AFP) and CA19-9 were negative. The patient simultaneously received percutaneous biopsy and locoregional treatment (LRT)with alcohol injection. The histopathological examination was consistent with the diagnosis of HCC. Eigtheen months after diagnosis, the patient underwent a successful LT. Immunosuppression included short-term (three months) corticosteroids and low-dose tacrolimus. The postoperative course was uneventful, and the patient was discharged after 13 days. Five months later, the patient presented with invalidating pain in the left leg, right maxilla, and mandible. Biochemistry revealed moderate anicteric cholestasis(γGT>2.5 times the upper limit of normality); tumor markers remained normal. At the ultrasounds, liver parenchyma was heterogeneous. A per-cause liver biopsy was performed and proved negative. Chest and lower limbs X-rays were normal, but bone scintigraphy revealed several areas of increased uptake in the trochanter, first rib, right mandible and maxilla, corresponding with osseous metastases. Palliative therapy was started, and immunosuppression was lowered to infra-therapeutic tacrolimus levels. The patient died two months later due to diffuse cancer spread, an evolution corresponding to the outcome of HHS following LT [4 , 5] .
Pathologic examination of the 1210 g heavy, cirrhotic, liver revealed a 40-mm large tumor in segment IV surprisingly harboring two distinct zones ( Fig. 1 ). Microscopic examination confirmed the presence of an inner 23-mm large part of the lesion corresponding to HCC and an outer 35-mm fibrous zone corresponding to a sarcoma. The first, non-necrotic lesion was composed of large hepatocytic plates giving rise to small bud formation. The cells contained hyperchromatic irregular nuclei, and had a high nucleocytoplasmatic ratio and sometimes an abnormal mitotic activity.The few present cytoplasms were basophilic. The HCC was surrounded by a lesion containing large areas of mesenchymatous tissue including several necrotic areas and cells with hyperchromatic,irregular nuclei and high, abnormal mitotic activity. All the findings corresponded to a sarcoma. IHC staining was negative for vimentin,alpha-actin, desmin, CD34, and factor-VIII but slightly positive for AFP and CEA in the HCC. All stainings were negative in the sarcomatous lesion.
The sarcomatous HCC is a very rare variant of HCC, which combines both HCC and spindle cell components [6] . This tumor has several other names such as spindle-cell carcinoma, sarcomatoid carcinoma, pseudo-sarcoma and carcinosarcoma [5] . The diagnosis of this cancer is difficult, as serological tumor markers are normal and typical imaging findings are missing. Although the pathogenesis remains unclear, it seems that the sarcomatous component in HCC comes from dedifferentiated or anaplastic cells. The biologic behavior is very aggressive and, therefore, the outlook is very bad.Intrahepatic and/or extrahepatic metastases are frequent. Response after LRT [e.g., trans-arterial chemoembolization (TACE)] is poor.Early (metastatic) recurrence after partial resection and LT is the rule [7 , 8] .
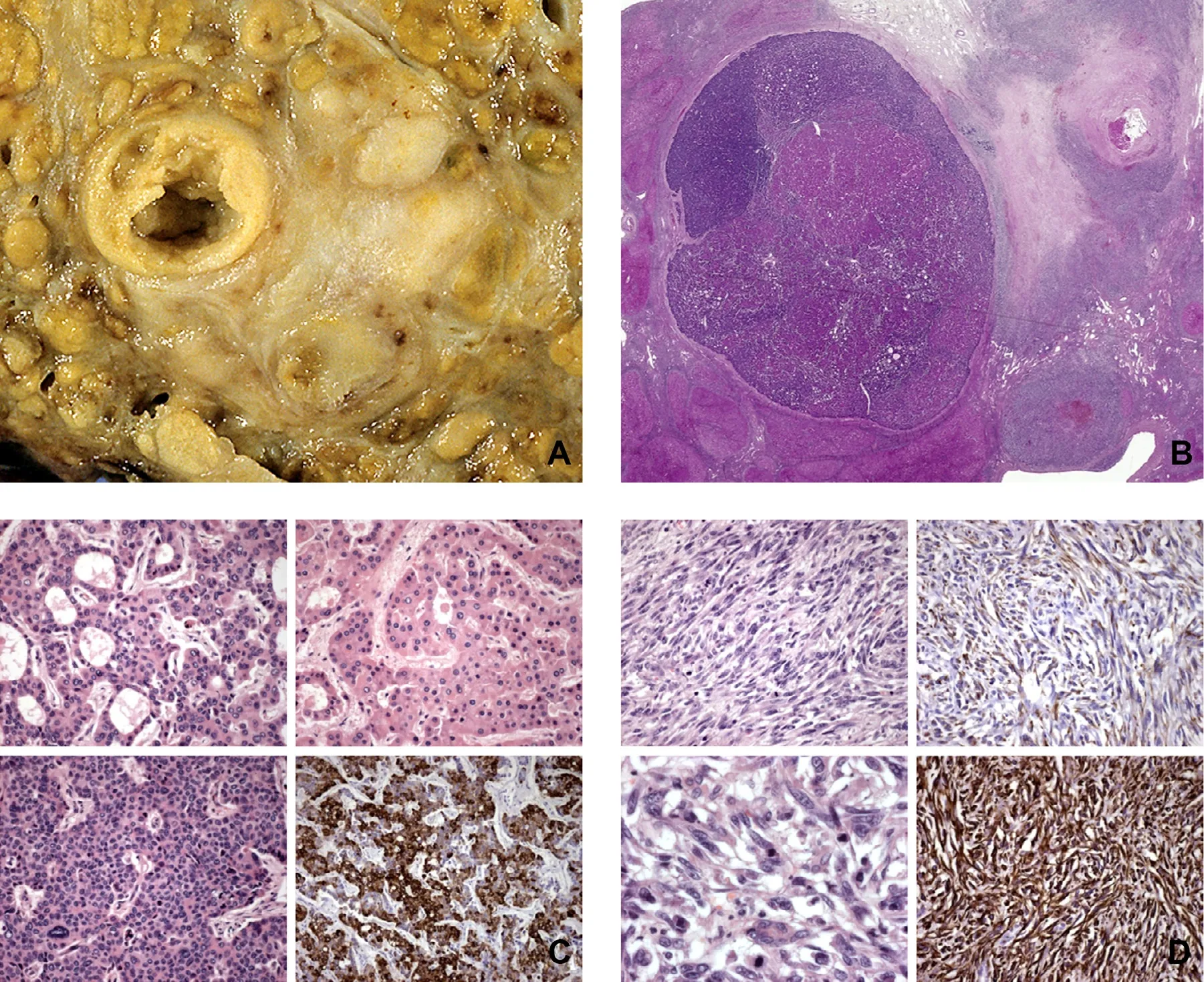
Fig. 1. ( A) Macroscopy shows a 40-mm large tumor in a cirrhotic liver harboring two distinct zones corresponding to an HCC (with bud formation) surrounded by a sarcomatous lesion. ( B) Microscopy shows the different glandular and spindle cell types corresponding to the two different tumor components. ( C) Immunohistochemistry of HCC part of the tumor was positive for AFP antigen. ( D) Immunohistochemistry of sarcomatous part of the tumor was negative for different stainings.
The fatal outcome reported in the presented case highlights four points of major concern in the context of transplantation,given the ever-increasing organ scarcity and the extremely poor results of LT in case of aggressive liver tumors. Firstly, HHS should be regarded as an absolute contraindication to LT [4 , 9] . Indeed,the European experience based on the ELTR-ELITA data from 22 HHS recipients showed that tumor recurrence occurred in all patients at a mean of 6 months and that no patient survived for more than two years after LT. Osseous metastases were the most frequent site of early tumor recurrence [4 , 5 , 9] . Secondly, prognosis after LT for mixed malignancies is steered by the most aggressive component of the tumor [7 , 8 , 10-12] . The occurrence in our patient of a widespread metastatic disease six months after LT indicates that the sarcomatous component became the dominating part of the tumor. Thirdly, routine percutaneous biopsies should be more deliberately considered, especially in potential liver recipients presenting unspecific tumor imaging [13] . The Asan medical experience showed that except for liver biopsy, no diagnostic method could distinguish sarcomatous from ordinary HCC [7] . Fourthly, the precise pathologic evaluation, including extensive immunostaining,of each tumor is key for accurately predicting the prognosis and interpreting the outcome of surgery and LT. In the case of sarcomatoid HCC, the survival rates are extremely poor, with 3-year overall and disease-free survivals of 18% after resection, and 37% and 25% after LT. Early recurrence and frequent extrahepatic metastases, even after R0 resection, are the rule [7 , 8 , 11 , 14] .
In conclusion, in the absence of special or unique clinical and serological features, mixed tumors are difficult to diagnose preoperatively, and thorough identification of the dual component at the pathology of the liver biopsy or hepatectomy specimen is often the only way to make a correct diagnosis. Clinical awareness and recognition of such tumors are critical, as they dictate appropriate treatment strategies dependent on the individual biological aggressiveness of each of the tumor components. Recognition of these mixed tumors is of special importance in the field of LT because of their dismal outcome questioning the use of scarce allografts.
CRediT authorship contribution statement
Giuseppe Orlando:Investigation, Writing - original draft.Quirino Lai:Investigation, Writing - original draft.Jan Lerut:Conceptualization, Investigation, Writing - original draft, Writing - review & editing.
Funding
None.
Ethical approval
This study was approved by the Ethics Committee of the Université catholique de Louvain.
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Neoadjuvant chemoradiotherapy before resection of perihilar cholangiocarcinoma: A systematic review
- Hepatobiliary&Pancreatic Diseases International
- Human microbiome is a diagnostic biomarker in hepatocellular carcinoma
- Current practice of anticoagulant in the treatment of splanchnic vein thrombosis secondary to acute pancreatitis
- Enhanced recovery after surgery program in the patients undergoing hepatectomy for benign liver lesions
- Assessment of biological functions for C3A cells interacting with adverse environments of liver failure plasma