Prognostic impact of the Bismuth-Corlette classification: Higher rates of local unresectability in stage IIIb hilar cholangiocarcinoma
2020-05-10MichaelPasseriMariaBaimasGeorgeJesseSulzerDavidIannittiJohnMartinieErinBakerLeeOcuinDionisiosVrochides
Michael J Passeri, Maria R Baimas-George, Jesse K Sulzer, David A Iannitti, John B Martinie,Erin H Baker, Lee M Ocuin, Dionisios Vrochides
Division of HPB Surgery, Department of Surgery, Carolinas Medical Center, 1025 Morehead Medical Dr., Suite 600, Charlotte, NC 28204, USA
ABSTRACT
Keywords:
Bismuth-Corlette stage
Cholangiocarcinoma
Biliary tract surgical procedures
Biliary tree
Liver surgery
Introduction
The term cholangiocarcinoma incorporates a varied group of aggressive malignancies arising from biliary epithelium. This group can be further organized into subcategories based on location,growth pattern, histology, and genetic profile [1-5] . Accounting for roughly 60% of all cases, hilar cholangiocarcinoma is the most common subtype and includes tumors that originate between the cystic duct and the second order biliary radicals on either side of the common bile duct confluence [6] . Due to its location seated in the porta hepatis amongst a dense network of critical vascular and biliary structures, hilar cholangiocarcinoma has established notoriety for the difficulty inherent in its resection.
The Bismuth-Corlette (BC) system is a widely used classification system for preoperative staging of patients based on proximal extension along the biliary tree, classifying patients into four categories ( Fig. 1 ). This staging can be assessed through invasive or noninvasive techniques, and guides surgical planning for patients thought to have resectable disease [7] . While those with bilateral disease (BC IV) are often not candidates for curative resection, patients staged as BC IIIa and IIIb disease can be considered for surgical resection. However, given the nature of portal vasculobiliary anatomy, choosing the optimal method of resection is more complex than simply selecting a right hepatectomy for right sided disease or a left hepatectomy for left sided disease [8] . Notably, the right hepatic artery lies directly behind the left hepatic duct for part of its anatomic course. Thus, stage IIIb tumors could theoretically involve both the left duct and right artery which would result in a higher likelihood of unresectability. And, conversely, stage IIIa tumors should not involve the contralateral artery and be more likely to be resectable ( Fig. 2 ).
This theoretical concern has limited validation in the literature.The aim of this study was to review consecutive cases of hilar cholangiocarcinoma that were taken to the operating room for intended resection, with the hypothesis that resections of preopera-tively staged IIIb tumors are more likely to be aborted for reasons of local advancement due to the anatomic proximity of the contralateral artery.
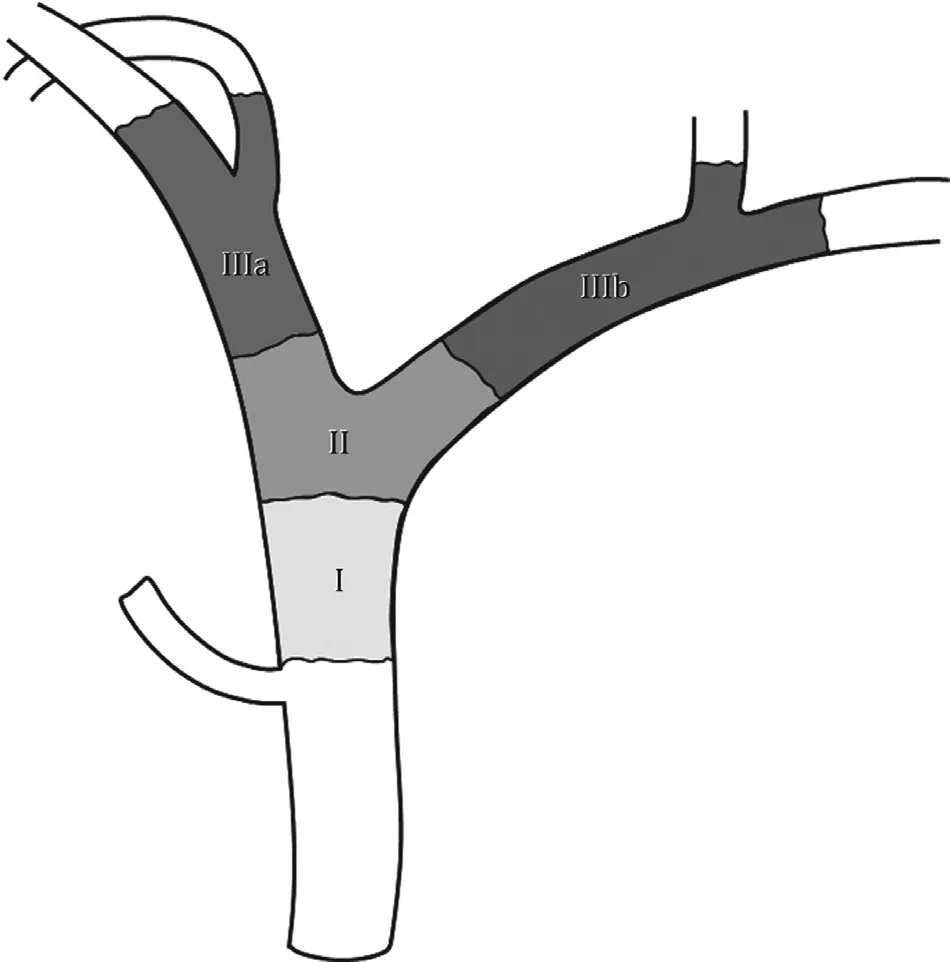
Fig. 1. Bismuth-Corlette staging system for hilar cholangiocarcinoma based on proximal extent of the tumor. Stage I is limited to the common hepatic duct below the confluence. Stage II involves the confluence but is limited proximally to the first order right and/or left ducts. Stage IIIa extends up to or beyond the second order biliary radicals on the right, while stage IIIb extends up to or beyond the second order biliary radicals on the left.
Methods
A review of a prospectively maintained internal database at Carolinas Medical Center, a tertiary care center, was used to identify patients between April 2008 and September 2016 for intended resection of hilar cholangiocarcinoma. Inclusion criteria included preceding staging laparoscopy to rule out metastatic disease followed by a preliminary dissection and evaluation of the biliary tree. Cases were grouped based on unresectability and resectability ( Fig. 3 ).The primary outcome was to determine and compare the percentage of explored cases that were resectable between the BC stages;particularly BC IIIb cases and all other BC stages. The secondary outcome included comparing the percentage of total cases that made it to resection out of all cases including those aborted for either metastatic or locally advanced disease. Chi-square test was employed in SPSS (IBM SPSS, IBM Corp., Armonk, NY, USA) to determine whether the primary outcome (cases resected over cases explored) or secondary outcome (cases resected over all cases) was significantly lower in BC IIIb tumors compared to other tumors.
Results
There were 68 consecutive cases of hilar cholangiocarcinoma identified that were taken to the operating room for intended resection. All the cases were preoperatively staged using a combination of cross-sectional imaging and cholangiography. There were 39 BC I/II cases (57.4%), 9 BC IIIa cases (13.2%), and 20 BC IIIb cases(29.4%).
After initial diagnostic laparoscopy, 16 cases (23.5%) were aborted due to metastatic disease [10 BC I/II (62.5%), 4 BC IIIa(25.0%), 2 BC IIIb (12.5%)]. The majority of metastases were found as peritoneal disease or liver surface lesions ( Table 1 ). Of the remaining 52 cases that proceeded with laparotomy and dissection/evaluation of the hepatic hilum, an additional 14 cases (26.9%)were aborted due to locally unresectable disease. Five of these aborted cases were staged as BC I/II (35.7%), one as BC IIIa (7.1%),and eight as BC IIIb (57.1%) ( Table 2 ).
Ultimately, 38 cases proceeded with attempted R0 resection.Fourteen cases (36.8%) were reported as left hepatectomy, nine(23.7%) as right hepatectomy, eight (21.1%) as bile duct resection without major hepatectomy, two (5.3%) as right trisectionec-tomy, two (5.3%) as right hepatectomy with concomitant Whipple procedure, and three (7.9%) as bile duct resection with concomitant Whipple procedure. Of these cases, 24 were staged as BC I/II(63.2%), 4 as BC IIIa (10.5%), and 10 as BC IIIb (26.3%).
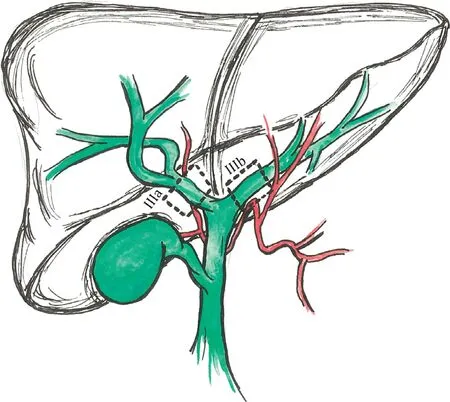
Fig. 2. Left sided hilar cholangiocarcinoma (Bismuth-Corlette stage IIIb) involving the contralateral (right sided) artery and right sided hilar cholangiocarcinoma (Bismuth-Corlette stage IIIa) away from the contralateral (left sided) artery.
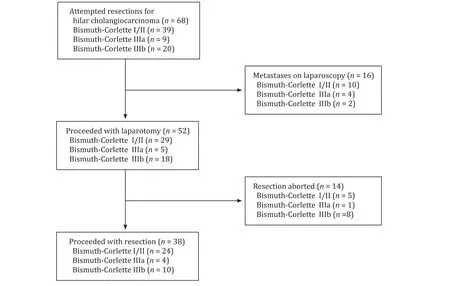
Fig. 3. Study flowchart.
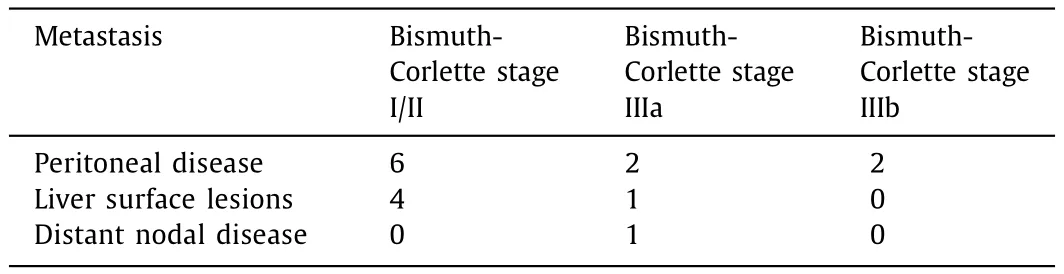
Table 1Aborted cases for metastatic disease.

Table 2Aborted cases for locally advanced disease.
After excluding for cases aborted for distant metastatic disease,the resection rate for BC IIIb lesions was 55.6% compared to 80.0%of BC IIIa lesions and to 82.4% of lesions from BC I-IIIa staged groups (P<0.05). About 44.4% of BC IIIb lesions were aborted for locally advanced disease versus 17.6% of remaining BC stages( Table 3 ). If cases with distant metastatic disease were included,the resection rate for BC IIIb lesions was 50.0% compared to 44.4%of BC IIIa lesions and 58.3% of BC I-IIIa staged lesions. Fifty percent of BC IIIb lesions were aborted for locally advanced disease and distant metastases versus 41.7% of remaining BC stages ( Table 3 ).
Postoperative length of hospital stay was 15 days for BC I/II,13 days for BC IIIa and 8 days for BC IIIb patients ( Table 4 ). The 30-day readmission rate was statistically different between groups:16.7% for BCI/II, 0% for BC IIIa and 30.0% for BC IIIb (P= 0.017).The 30-day complication rate was equivalent at 50.0% among all three groups. Adjuvant chemotherapy was started in 54.2% of BC I/II patients, 75.0% of BC IIIa, and 80.0% of BC IIIb. There was evidence of regional recurrence in 29.2% of BC I/II, 50.0% of BC IIIa,and 20.0% of BC IIIb patients. There was no significant difference in regional recurrence rates or length of time to recurrence between groups. Metastatic recurrence was rare and occurred in only one patient in the BC I/II group and two patients in the BC IIIb group.Only three patients in the BC I/II group suffered a 30-day mortality; and there was no significant difference in disease-free survival and overall survival between groups ( Fig. 4 ).

Table 3Rates of resectability for different stages of hilar cholangiocarcinoma.
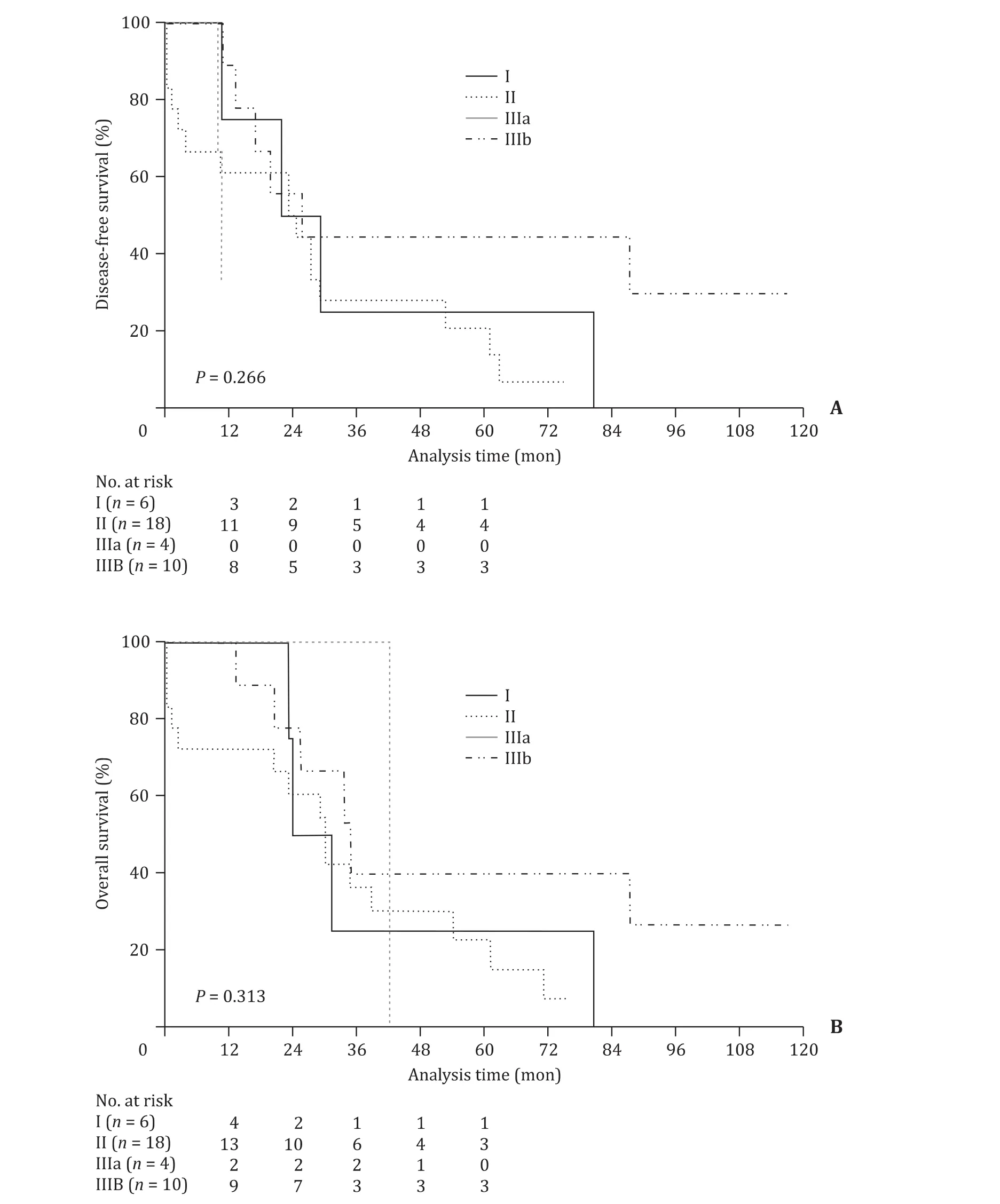
Fig. 4. Disease-free survival ( A) and overall survival ( B) after resection compared between Bismuth-Corlette staged groups.
Discussion
For patients with hilar cholangiocarcinoma, the only chance for cure is a complete operative resection. Since Dr. Gerald Klatskin first drew attention to the disease with a case series of 13 patients in 1965, the introduction of increasingly complex operative techniques, including portal vein resection, extended hepatectomy,and preoperative liver molding, have brought more and more cases within reach of R0 resection [9-12] . However, as evidenced by high rates of microscopically positive margins reported after hilar cholangiocarcinoma resection, surgical resection remains one of the most challenging operations in the field of hepatobiliary surgery [6 , 13-15] . Further, unlike over malignancies, numerous studies have validated the importance of complete tumor clearance, concluding that obtaining microscopically negative margins provides significant survival advantage [6 , 15-17] .
Obtaining an R0 resection of hilar cholangiocarcinoma that extends above the second order biliary radicals on either side of the liver (BC IIIa or IIIb disease) generally requires resection of the ipsilateral hemiliver and consequent need to preserve thecontralateral hemiliver. For this reason, tumors involving a second order hepatic duct and a contralateral hepatic artery are considered to be unresectable at most centers. The ability to anticipate bilateral vasculobiliary disease preoperatively could better inform patient discussions and critically influence care plans.
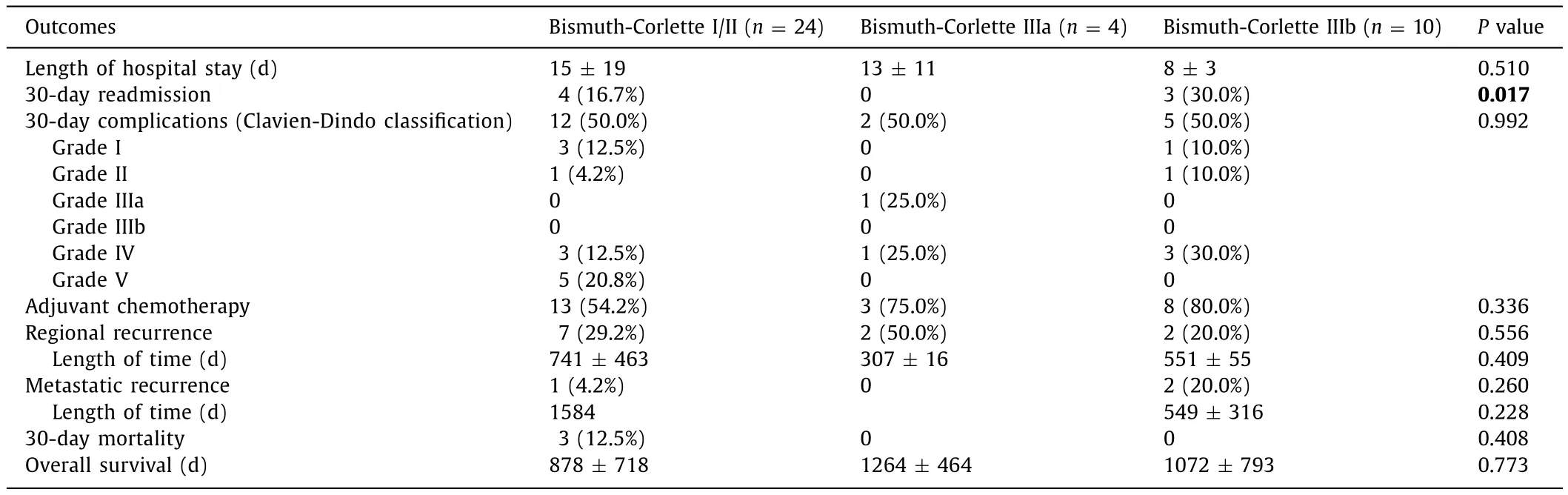
Table 4Postoperative and oncologic outcomes.
Cross sectional imaging may be able to assess invasion of the right hepatic artery by left sided tumors with reasonable accuracy,although this has not been widely replicated. Our data demonstrate that, even when right hepatic artery involvement is not evident in preoperative imaging, BC IIIb tumors should be regarded with a high level of suspicion for local unresectability [18] . After distant metastatic disease was excluded, 8 of 18 (44.4%) cases for BC IIIb tumors were aborted, compared to 1 out of 5 (20.0%) cases of BC IIIa and to 5 of 29 (17.2%) cases of other BC staged tumors. Of note, all cases were deemed potentially resectable based on preoperative imaging.
These data suggest that BC IIIb tumors may involve the contralateral artery, resulting in higher rates of spread and thus local unresectability. As such, when preparing for a BC IIIb resection,surgeons should consider a contingency plan in the event that disease is more extensive than assessed on preoperative imaging.Abortion of the procedure is certainly an acceptable option, though it results in the morbidity of a laparotomy and hilar dissection without any oncologic benefit. Other strategies can include right hepatic artery resection and reconstruction which can allow surgeons to achieve R0 resections for advanced BC IIIb tumors.The literature does report that arterial resection can offer some benefit; however, many other authors find either no difference or detrimental effects, increasing mortality rates from less than 2%to an estimated 16% [14 , 19-24] . Another surgical option in the setting of locally advanced disease is the performance of right trisectionectomy for left sided tumors [8] . While this may seem counterintuitive, it is logically consistent with the hepatic arterial anatomy as described above. Finally, intraoperative irreversible electroporation has demonstrated efficacy in extended palliation of biliary obstruction from advanced hilar cholangiocarcinoma and may play a future role in margin enhancement for tumors with arterial involvement [25] . As these aggressive options are not available at most centers, it is reasonable to consider transferring well selected BC IIIb staged patients to locations where they are offered and to include them in preoperative discussion.
Neoadjuvant concurrent chemoradiation therapy may also have a role to play in the treatment of BC IIIb tumors. Neoadjuvant concurrent chemoradiation therapy is already an established cornerstone of the transplant pathway for hilar cholangiocarcinoma lesions, and may also be able to downstage hilar cholangiocarcinoma lesions and impact local resectability [26 , 27] . Further research is needed to investigate such.
There were several limitations present in this study. As a retrospective analysis whose sole inclusion criterion was intended resection of hilar cholangiocarcinoma, there was implicit selection bias. Furthermore, hilar cholangiocarcinoma is already a rare disease, and rarer still are cases taken to the operating room for intended resection, resulting in a small sample size. Regardless,the higher proportion of BC IIIb cases aborted for locally advanced disease in comparison to all BC cases still attained statistical significance.
In conclusion, when hilar cholangiocarcinoma is preoperatively staged as BC IIIb, surgeons should anticipate a higher probability of locally unresectable disease due to the arterial and biliary anatomy.This information can appropriately inform patient discussions prior to intended resection and may warrant consideration for neoadjuvant chemoradiation or transfer to a center where advanced methods of arterial clearance are available.
Acknowledgment
We thank Keith J. Murphy, MSPH for assistance with statistical analysis.
CRediT authorship contribution statement
Michael J Passeri:Conceptualization, Data curation, Formal analysis, Writing - original draft.Maria R Baimas-George:Data curation, Formal analysis, Visualization, Writing - original draft, Writing - review & editing.Jesse K Sulzer:Data curation, Supervision.David A Iannitti:Data curation, Supervision, Writing - review &editing.John B Martinie:Data curation, Supervision, Writing - review & editing.Erin H Baker:Data curation, Supervision, Writing - review & editing.Lee M Ocuin:Data curation, Supervision,Writing - review & editing.Dionisios Vrochides:Conceptualization, Methodology, Supervision, Writing - review & editing.
Funding
None.
Ethical approval
This study was approved by the Institutional Review Board of Carolinas Medical Center (Charlotte, NC, USA).
Competing interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
杂志排行
Hepatobiliary & Pancreatic Diseases International的其它文章
- Neoadjuvant chemoradiotherapy before resection of perihilar cholangiocarcinoma: A systematic review
- Hepatobiliary&Pancreatic Diseases International
- Human microbiome is a diagnostic biomarker in hepatocellular carcinoma
- Current practice of anticoagulant in the treatment of splanchnic vein thrombosis secondary to acute pancreatitis
- Enhanced recovery after surgery program in the patients undergoing hepatectomy for benign liver lesions
- Assessment of biological functions for C3A cells interacting with adverse environments of liver failure plasma