Hemodynamic responses of patients with stable coronary artery disease to a comedy film: study protocol for a randomized controlled trial
2019-10-14RosaneMariaNeryRaquelPetryBuhlerboraSantosMacedoJulianaMaiaDelfinoFilipeFerrariAndersonDonelliSilveiraMarcoAurlioLumertzSaffiRicardoStein
Rosane Maria Nery , Raquel Petry Buhler , Débora Santos Macedo , Juliana Maia Delfino , Filipe Ferrari ,Anderson Donelli Silveira , , Marco Aurélio Lumertz Saffi , Ricardo Stein , ,
1 Exercise Cardiology Research Group (CardioEX), Hospital de Clínicas de Porto Alegre, Universidade Federal do Rio Grande do Sul,Rehabilitation Division, Porto Alegre, Brazil
2 Hospital de Clínicas de Porto Alegre, Porto Alegre, Brazil
3 Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
Abstract
Key words: laughter therapy; endo the lium; flow-mediated dilation; functional capacity; blood biochemistry; quality of life
INTRODUCTION
Cardiovascular diseases are the leading cause of death worldwide, and lifestyle changes are seen as key to improving this scenario.1Cardiac rehabilitation is considered a class I intervention, which provides net benefit to overall health, and is strongly recommended by most guidelines.2Despite this, less than 30% of patients who have experienced a cardiovascular event in the United States are engaged in a supervised cardiac rehabilitation program, even when they are eligible for such non pharmacological therapeutic strategies.3Studies on this topic have been heterogeneous in terms of the type, duration,and intensity of physical training; in addition, they have not covered complementary modalities such as laughter therapy.4-7
The idea that laughter can produce positive health benefits has become increasingly popular both among health care providers and the general public.However, considering the multifaceted nature of the concepts of humor and “sense of humor,” their potential health benefits are difficult to characterize and measure.Researchers who have examined the humor-health dyad have conceptualized humor in different ways: as a personality trait, an emotional response, a mental process, or a therapeutic intervention.In this particular aspect,the concept of humor adopted also influences the design of research projects on the topic.8
Laughter is more than a visual and vocal behavior.It always involves a series of physiological changes, including skeletal muscle contractions, increased heart rate (secondary to catecholamine release), and hyperventilation, which promotes increased maximal breathing and, consequently, an increase in oxyhemoglobin saturation.9Studies have shown that laughter therapy can improve quality of life, psychological status, increase total lung capacity, and decrease pulmonary hyperinflation in patients with chronic obstructive pulmonary disease.10,11
Sugawara et al.12evaluated endothelial function (measured by flow-mediated dilation, FMD) in healthy adults who watched a 30-minute documentary or a comedy film session,and observed better results after the latter.However, to the best of our knowledge, no randomized controlled trial has been conducted to investigate the impact of laughter therapy in patients with stable coronary artery disease (CAD).
Laughter therapy is an inexpensive non pharmacological intervention that requires very little investment in time or infrastructure.There are few contraindications, the risk of side effects is very low, and it can be readily prescribed by health practitioners.In healthy individuals, laughter therapy seems to improve endothelial function, immune response, and even energy expenditure, and may have a cardioprotective effect.Thus, it seems appropriate to investigate the effects of this modality in patients with ischemic heart disease, aiming to evaluate its effectiveness for cardiovascular rehabilitation purposes.
Objectives
Research hypothesis
Viewing a comedy film sessions (intervention) would provide superior results to viewing documentary sessions (control)on endothelial function and functional capacity in patients with CAD.
Primary objectives
To compare the effect of 24 sessions of a comedy film and a neutral documentary on endothelial function and functional capacity in patients with CAD.
Secondary objectives
To compare the effect of 24 sessions of a comedy film and neutral documentary on inf l ammatory markers, biochemical parameters, and quality of life.
SUBJECTS AND METHODS
Study design
This is a randomized, parallel-design, examiner-blinded, controlled clinical trial.Thirty patients will be included (15 in each group).They will be recruited from the outpatient ischemic heart disease clinic of Hospital de Clínicas de Porto Alegre,an 800-bed university hospital in Porto Alegre, Southern Brazil.Endothelial function will be assessed by measurement of brachial-artery FMD at the noninvasive cardiology unit of Hospital de Clínicas de Porto Alegre.The study will be conducted from August 2013 to December 2019.The study protocol was approved by the Institutional Review Board of Hospital de Clínicas de Porto Alegre (protocol No.13-0124)on July 9, 2013 (Additional file 1).Written informed consent will be obtained from all patients before participation (Additional file 2).The trial protocol was registered in Clinical Trials.gov (identifier: NCT02824120) and adheres to the Standard Protocol Items: Recommendations for Interventional Trials(SPIRIT) guidance for protocol reporting13(Additional file 3).The current protocol version is 1.0.The schedule of enrollment, interventions, and assessments is presented in Table 1.

Table 1: Schedule of enrollment, interventions, and assessments
Inclusion criteria
· Age over 18 years
· Diagnosis of CAD established by cardiac catheterization,with a 50% lesion in at least one epicardial vessel (if the patient has a history of acute coronary syndrome or has undergone coronary revascularization, the event should have occurred more than 6 months before enrollment)
· Patients classified as low risk according to the Cardiopulmonary and Metabolic Rehabilitation Guideline14(functional capacity≥ 5 METs, absence of myocardial ischemia at rest or on cardiopulmonary exercise testing, adequate blood pressure response to exertion and ability to self-monitor the intensity of exercise)
· Availability to attend the Hospital de Clínicas de Porto Alegre clinic twice a week
· Fitness to enter an exercise-based cardiac rehabilitation program
Exclusion criteria
· Involvement in another clinical trial
· Presence of autoimmune disease
· Oral anticoagulant therapy
· Mechanical or biological valve replacement for valvular heart disease
· Presence of pacemaker or implantable cardioverter/defibrillator
· Left bundle branch block on 12-lead electrocardiogram
· Severe pulmonary disease
· Major depression or bipolar disorder
· Chronic atrial fibrillation
· Left ventricular dysfunction (left ventricular ejection fraction < 45%)
· Active infection or malignancy (other than basal cell carcinoma)
· Chronic renal failure
· Illiteracy
· Inability to understand the informed consent form
Informed consent
The project was submitted to the Research Ethics Committee of Hospital de Clínicas de Porto Alegre for consideration.Authorization for subsequent use of obtained data will be requested from all patients involved in the study through the informed consent form.Confidentiality will be ensured according to the applicable legislation.Any questions will be thoroughly answered and discussed.The principal investigator will prospectively monitor any complications arising from the study intervention.The study will be discontinued if any serious side effects resulting from the intervention are identified.
Recruitment and study protocol
First contact with the patients will be established in the outpatient CAD clinic.Eligible patients will be informed of the study and invited to participate; those who accept will be tested by a blinded assessor and randomly allocated to one of the groups.A flow diagram of patient recruitment is shown in Figure 1.

Figure 1: Proposed trial design.
Randomization and blinding
Group allocation will be determined by a random-numbers table generated in IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA), and distributed at a 1:1 ratio between the intervention and control groups.The generated codes will be distributed into sequentially numbered, sealed brown envelopes.The investigator in charge of randomization will not participate in the other data collection stages.Outcome assessors will be blinded to group allocation.
Baseline measures
Primary and secondary outcomes will be assessed at baseline,after provision of written informed consent but before allocation to one of the study groups.At the end of the 24 sessions,the subject will be evaluated again.
Endothelial function (assessed by brachial artery FMD measurement), functional capacity (assessed by peak oxygen consumption [VO2peak] on cardiopulmonary exercise testing),a broad panel of inf l ammatory markers in blood (high-sensitivity C-reactive protein, tumor necrosis factor-alpha, vascular cell adhesion molecule 1, intercellular adhesion molecule 1,interleukin-6, interleukin-10), biochemical parameters (total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides, cortisol, glucose, complete blood count, potassium, renin, thyroid-stimulating hormone, and troponin T), and quality of life will be measured.
Intervention
Patients will perform two 30-minute weekly stretching sessions for 2 months (two sessions per week, for a total 24 sessions).The exercises will be of mild to moderate intensity (modified Borg scale 3-6).After each stretching class, participants will watch a 30-minute film, selected according to group allocation.Brief l y, after randomization, patients who are allocated to the comedy film group will receive a list of several comedy television series, and are asked to choose those they find most amusing.Episodes of these series will then be shown as the intervention after each stretching session.Conversely, individuals allocated to the control group will watch a 30-minute neutral documentary (defined as one that does not cause exacerbated emotions of sadness or joy), selected by the investigators, after each stretching session.
Before and after each session, appropriate scales will be used to evaluate the participants’ mood.
The intervention will take place at the Department of Physical Medicine and Rehabilitation of Hospital de Clínicas de Porto Alegre.Staff physical educators will serve as instructors for the stretching sessions, according to the protocol described in Table 2.
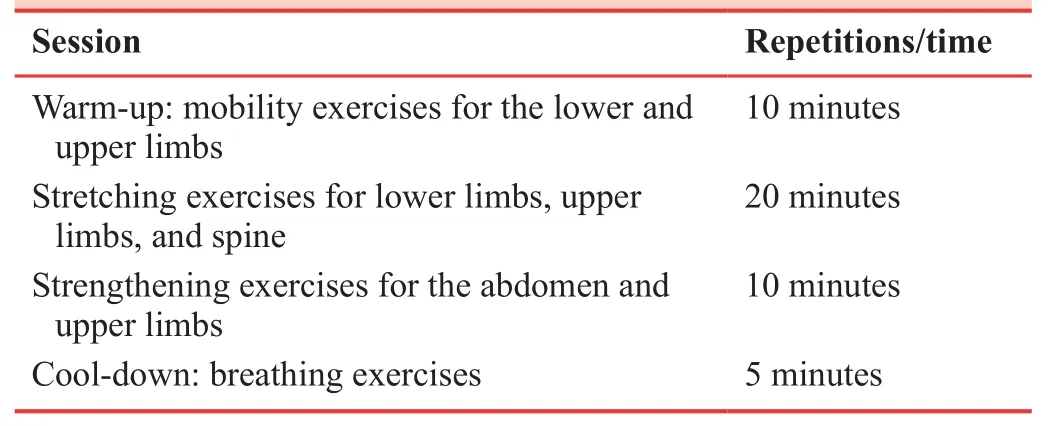
Table 2: Activities performed in stretching classes
At the start of each exercise session, blood pressure and resting heart rate will be measured.Blood pressure will also be measured immediately after training and at 3 minutes of recovery.Participants will be allowed to relax in the seated position for at least 3 to 5 minutes before blood pressure measurements.The arm will be stretched, aligned with the mid-sternum, and supported.A properly sized cuff will be wrapped around the arm and attached to an aneroid sphygmomanometer, and blood pressure measured by the auscultation method as described elsewhere.15At least two blood pressure measurements will be obtained in the sitting position, 1 to 2 minutes apart; additional measurements will be obtained if the first two are markedly discrepant.
Heart rate will be monitored before, during, and up to 3 minutes after exertion with a Polar Fitness FS1 heart rate monitor (Polar, Finland).The physical educators who will guide the exercise sessions are trained in basic life support.All sessions will be supervised by a multidisciplinary team consisting of an attending physician, an assistant physician, a physical educator, and a psychologist.
All patients will be advised to seek immediate care at the Emergency Department of Hospital de Clínicas de Porto Alegre if any untoward event occurs during the study period.They will also carry identification cards bearing their name,medical record number, and guidance for immediate transfer to the Emergency Department of Hospital de Clínicas de Porto Alegre if they are taken to any other medical facility in the city of Porto Alegre or neighboring municipalities.
Outcome measures
The primary outcome measures are endothelial function and functional capacity; the secondary outcomes include a complete lipid profile, a wide-ranging panel of markers on inf l ammation, routine blood tests, and quality of life assessment.A detailed description is provided in the “Baseline measures”section above.
Measurement of main variables
Endothelial function
Noninvasive measurements of endothelial function will be obtained by FMD of the brachial artery using two-dimensional ultrasound equipment.FMD measurement will be performed in accordance with published guidelines.16Brief l y, the examination will start after 15 minutes of rest in a temperature-controlled room, with the patient supine and arms in a comfortable position.Any vasodilation medication will be discontinued at least 4 hours before the examination, if possible.Individuals will also be advised to refrain from exercising, drinking caffeine, and smoking for at least 4 hours before the examination.
Functional capacity
Cardiopulmonary exercise testing with expired gas analysis will be performed on a treadmill (Inbramed KT 10200, Inbramed, Porto Alegre, Brazil, speed 0-16 km/h [0-10 mph],grade 0-26%).A ramp protocol will be used, with a starting speed of 2.4 km/h and a starting grade of 2%; speed will be increased every 20 seconds in 0.1- or 0.2-km/h increments,and grade, every 60 seconds in 0.1-0.2% increments.The objective is to achieve fatigue within 8 to 12 minutes (mean,10 minutes).During the pretest phase, participants will walk for 1 to 3 minutes at a gentle pace to adapt to the treadmill.Heart rate will be monitored with a 12-lead electrocardiograph(Nihon Kohden Corporation, Tokyo, Japan), with electrode placement as described by Mason and Lika.17
Blood chemistry and biomarkers of inflammation
Total cholesterol, low-density lipoprotein cholesterol, highdensity lipoprotein cholesterol, cortisol, glucose, complete blood count, potassium, high-sensitivity C-reactive protein,renin, thyroid-stimulating hormone, triglycerides, troponin T,tumor necrosis factor-alpha, vascular cell adhesion molecule 1, intercellular adhesion molecule 1, interleukin-6, and interleukin-10 will be measured in blood samples.
Part of each blood sample will be taken immediately to the Hospital de Clínicas de Porto Alegre laboratory for analysis of lipid profile and blood sugar.The other part will be centrifuged at 4°C and 2879 ×gfor 10 minutes in an ALC PK 120 R centrifuge (ALC International, Milan, Italy) and the serum will be frozen at -80°C in labeled Eppendorf tubes for quantization of inf l ammatory biomarkers.
Quality of life
The 36-Item Short-Form Health Survey generic questionnaire will be used to assess quality of life on eight domains: vitality,physical functional capacity, pain, general health perception,physical role functioning, social role functioning, emotional role functioning, and mental health.The 36-Item Short-Form Health Survey scores range from 0 to 100 for each parameter.18
Sample size calculation
As there are no previous studies in this specific area of knowledge, our calculation was based on an experiment by Miller et al.,19who enrolled healthy subjects and compared the effect of mental stress versus laughter therapy on endothelial function.For a statistical power of 95%, an alpha error rate of 5%, and an absolute difference of 2.6 (1.9%) in FMD between groups,we calculated a total sample of 24 patients.Considering 20%attrition in the overall sample, 30 subjects (n= 15/group) will need to be enrolled.
Data management and monitoring
Due to minimal risks associated with the interventions and short duration of the trial, no Data Monitoring Committee will be established, nor will interim analyses be performed.
Statistical analysis
Data will be entered and coded into a Microsoft Excel 14.7.7 spreadsheet (Microsoft Corporation, Redmond, WA, USA).Categorical variables will be presented as absolute frequencies and percentages.Continuous variables with normal distribution will be expressed as mean and standard deviation, and those without normal distribution, as median and interquartile range.The chi-square test will be used to analyze categorical variables.For within-group comparison of quantitative variables before and after the intervention, Student’st-test for paired samples (for normally distributed variables) and the Wilcoxon test (for non-normally distributed variables) will be used.Between-group comparisons of changes in outcome variables will be done by analysis of covariance, using baseline values to adjust for later results.The Kruskal-Wallis test will be used to verify the assumption of normality.
The level of significance will be set at 5% (two-tailed) for all tests.All data will be analyzed in IBM SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA), by the intention-to-treat method.
DISCUSSION
To the best of our knowledge, this will be the first study to evaluate the effect of laughter therapy in adults with CAD.This experiment will provide an opportunity to evaluate the effect of this type of therapy in these patients in a routine clinical practice setting.
Laughter is a unique human response to humorous stimuli.It is also believed to act as a coping mechanism to reduce stress;it improves self-esteem and reduces psychological symptoms related to negative events.20,21In addition to these notable psychological benefits, laughter has physical repercussions,with possible gains attributed to reduction of muscle tension,enhanced oxygenation, and increased cardiac work.22Growing research in the field of laughter therapy is based on the assumption that these physiological changes can be beneficial to the cardiovascular system.23
Many advances have been made in determining the impact of endothelial function on the prognosis and rehabilitation of individuals with CAD.Despite the relevant finding that FMD of the brachial artery is an important marker in atherosclerosis;studies on its prognostic value are quite recent.Endothelial response is emerging as a prospective addition to the armamentarium for individual risk assessment and, perhaps, even as a potential therapeutic target.24
Within this context, laughter has been shown to inf l uence endothelial function.Sugawara et al.determined the effects of mirthful laughter (i.e., that elicited as a genuine response to a humorous stimulus) on endothelial function and central artery compliance.12In a crossover trial design,17apparently healthy adults (age 23 to 42 years) watched 30 minutes of a comedy film (intervention) or a documentary (control) on separate days.Ischemia-induced FMD of the brachial artery(measured by mode B ultrasonography) increased signif icantly after watching the comedy (17%) and decreased after watching the documentary (-15%).Carotid artery compliance(measured by simultaneous carotid ultrasound and applanation tonometry) increased 10% immediately after watching the comedy, returning to baseline within 24 hours.These changes were significantly associated with baseline FMD (r= 0.63).Conversely, exposure to the documentary did not affect carotid compliance.The authors concluded that mirthful laughter elicited by comic films has a beneficial impact on vascular function.12
Similar findings were reported by Vlachopoulus et al., who investigated the effects of film-elicited laughter on arterial stiffness.In their study,18healthy subjects watched three different films at random: a stressful film, a comedy, and a placebo in which nothing was projected.Comedy reduced pulse-wave velocity and arterial stiffness.23Miller et al.19compared FMD in 20 healthy subjects during 15 to 30 minutes of laughterinducing films and stress-inducing films.FMD was found to increase 22% after watching a comedy and reduce 47% after watching a stressful film.
Given the high prevalence and ominous mortality of cardiovascular diseases, we believe there is an important need to investigate the benefits of laughter therapy; a simple, safe,and inexpensive therapeutic alternative that, in addition toimproving quality of life, may exert a positive inf l uence on physiological and biochemical parameters in patients with stable CAD.
TRIAL STATUS
The current protocol version is 1.0.Patient recruitment will end in December 2019.Analysis of the primary outcome measure will be completed in December 2019.
Additional files
Additional file 1: Ethical approval documentation.
Additional file 2: Model consent form.
Additional file 3: SPIRIT checklist.
Author contributions
All authors contributed to the conception, design, literature search,and critical review of the manuscript for important intellectual content.All authors gave final approval for publication.
Conflicts of interest
None declared.
Financial support
This study was supported by Funding for Research and Events from the Hospital de Clínicas de Porto Alegre (FIPE-HCPA).
Institutional review board statement
The study protocol was approved by the Institutional Review Board of Hospital de Clínicas de Porto Alegre (protocol No.13-0124) on July 9, 2013.
Declaration of patient consent
The authors certify that they will obtain all appropriate consent from participant.In the forms the patients will give their consent for their images and other clinical information to be reported in the journal.The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity forms.
Reporting statement
This study followed the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT) guidance for protocol reporting.
Biostatistics statement
A staff statistician at Hospital de Clínicas de Porto Alegre reviewed the statistical methods of this study.
Copyright license agreement
The Copyright License Agreement has been signed by the first author before publication.
Data sharing statement
Anonymized individual data will be available immediately after study publication upon request from those who wish to access the data for 5 years.If anonymized data is provided, it should be done so after proposals to rstein@cardiol.br.Raw data will be stored in a locked cabinet at the Hospital de Clínicas de Porto Alegre for this time period before being destroyed.Personal results will also be available to participants upon request.If requested, study protocols and outputs of statistical analysis will be available.
Plagiarism check
Checked twice by iThenticate.
Peer review
Externally peer reviewed.
Open access statement
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-Share Alike 4.0 License, which allows others to remix, tweak, and build upon the work non-commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
杂志排行
Clinical Trials in Degenerative Diseases的其它文章
- Relationship between low vitamin D status and extra-skeletal diseases: a systematic review on effects of prophylaxis with vitamin D
- Tanreqing injection with ambroxol hydrochloride for heart failure and pulmonary infection in senile degenerative heart disease: a randomized controlled trial
- Clinical progress of cell therapy in treating age-related macular degeneration
- Role of trace mineral in periodontal health: a review
- CTDD call for papers