健脾止动汤联合耳穴贴压对儿童多发性抽动症的下丘脑-垂体-肾上腺轴激素、神经递质的影响
2019-09-10康碧陈宜
康碧 陈宜
摘要 目的:觀察健脾止动汤联合耳穴贴压治疗儿童多发性抽动症(TS)的疗效及对下丘脑-垂体-肾上腺轴(HPA轴)激素、神经递质的影响。方法:选取2016年1月至2017年3月成都市新都区中医医院收治的符合《美国精神疾病诊断统计手册》第4版TS诊断标准的患儿80例作为研究对象,按照随机数字表法分为对照组和观察组,每组40例,同期入组40例健康儿童作为健康对照组,对照组和观察组均口服氟哌啶醇片剂治疗,对照组再给予耳穴贴压治疗,观察组再给予耳穴贴压联合健脾止动汤治疗,对照组和观察组均治疗12周,治疗前、治疗后检测中枢神经递质如多巴胺(DA)、5-羟色胺(5-HT)、去甲肾上腺素(NE)、天门冬氨酸(ASP)、γ-氨基丁酸(GABA)和HPA轴相关激素皮质醇(COR)和促肾上腺皮质激素(ACTH),并与健康对照组比较,进行耶鲁综合抽动严重程度量表(TGTSS)评分,随访6个月,评估其临床疗效。结果:治疗前,对照组和观察组的多巴胺、NE、GABA明显低于健康对照组,差异有统计学意义(P<0.05),5-羟色胺、ASP明显高于健康对照组,差异有统计学意义(P<0.05);治疗后,对照组和观察组多巴胺、5-羟色胺、ASP均较治疗前明显降低,差异有统计学意义(P<0.05),NE、GABA均较治疗前明显升高,差异有统计学意义(P<0.05),且观察组治疗后多巴胺、5-羟色胺、ASP明显低于对照组,差异有统计学意义(P<0.05),NE、GABA明显高于对照组,差异有统计学意义(P<0.05)。治疗前对照组和观察组的COR、ACTH明显高于健康对照组,差异有统计学意义(P<0.05);对照组和观察组治疗后COR、ACTH均较治疗前明显降低,差异有统计学意义(P<0.05),且观察组治疗后COR、ACTH明显低于对照组,差异有统计学意义(P<0.05)。对照组和观察组治疗后运动抽动评分、发声抽动评分、抽动总分均较治疗前明显降低,差异有统计学意义(P<0.05),且观察组治疗后各项评分均明显低于对照组,差异有统计学意义(P<0.05)。对照组和观察组的临床总有效率分别为85%和97.5%,差异有统计学意义(P<0.05)。结论:TS的发病与中枢神经递质失衡及HPA轴功能亢进有关,健脾止动汤联合耳穴贴压治疗能够有效下调HPA轴水平,调节中枢神经递质失衡,协同提高临床治疗效果。
关键词 儿童多发性抽动症;健脾止动汤;耳穴贴压;中枢神经递质;下丘脑-垂体-肾上腺轴;神经递质;TGTSS评分;临床疗效
Abstract Objective:To observe the effect and the influence of Jianpi Zhidong Decoction combined with auricular point sticking on hypothalamic-pituitary-adrenal axis (HPA-axis) and neurotransmitter content of children with Tourette syndrome (TS). Methods:A total of 80 cases with TS who met the TS diagnostic criteria of the fourth edition of the American Psychiatric Diagnostic Manual were enrolled in this study, which were divided into observation group and control group with 40 cases were in each group according to random number table. Another 40 healthy cases were enrolled in the study as healthy control group. Observation group and control group were treated with haloperidol tablets. Observation group was treated with auricular point sticking, and control group was treated with Jianpi Zhidong Decoction combined with auricular point sticking. Both groups had been treated for 12 weeks. The central nervous system (CNS) neurotransmitter such as dopamine (DA), 5-hydroxytryptamine (5-HT) norepinephrine (NE), aspartate (ASP),γ-aminobutyric acid (GABA) and HPA-related hormone such as cortisol (COR) and adrenocorticotropic hormone (ATCH) were detected before and after treatment, which were compared with the healthy control group. Yale comprehensive twitch severity scale (TGTSS) score were calculated. All the cases had been followed at least 6 months, and then the clinical efficacy was assessed. Results:Before treatment, the DA, NE and GABA levels in the observation group and the control group were significantly lower than those in healthy control group. The difference was statistically significant (P<0.05). 5-HT and ASP levels in 2 groups were significantly higher than those in healthy control group. The difference was statistically significant (P<0.05). After treatment, the DA, 5-HT, ASP levels in observation group and control group were significantly lower than those before treatment. The difference was statistically significant (P<0.05). NE and GABA levels were significantly higher than those before treatment. The difference was statistically significant (P<0.05). DA, 5-HT, and ASP levels in the observation group were significantly lower than those in the control group. The difference was statistically significant (P<0.05). NE, GABA levels of observation group were significantly higher than that of control group. The difference was statistically significant (P<0.05). Before treatment, COR and ACTH levels in observation group and control group were significantly higher than those in healthy control group. The difference was statistically significant (P<0.05). After treatment, COR and ACTH levels in the observation group and the control group were significantly lower than those in healthy control group. The difference was statistically significant (P<0.05). COR and ACTH levels in the observation group was significantly lower than the control group. The difference was statistically significant (P<0.05). The movement and vocalization tics and tics total scores of the observation group and the control group were significantly decreased after treatment. The difference was statistically significant (P<0.05). The scores in the observation group were significantly lower than those in control group after treatment. The difference was statistically significant (P<0.05). The total clinical effective rates in control group and observation group were 85% and 97.5% respectively. The difference was statistically significant (P<0.05). Conclusion:The attack of TS is related to central nervous system imbalance and hyperactivity of HPA axis. Jianpi Zhidong Decoction combined with auricular point sticking can effectively reduce the level of HPA axis, regulate the imbalance of CNS neurotransmitter and improve the clinical therapeutic effects.
Key Words Childhood Tourette syndrome; Jianpi Zhidong Decoction; Auricular point sticking; CNS neurotransmitter; HPA axis; Neurotransmitter; TGTSS score; Clinical efficacy
中图分类号:R289.5文献标识码:Adoi:10.3969/j.issn.1673-7202.2019.06.036
多发性抽动症(Tourette Syndrome,TS)是儿童期常见的慢性神经精神障碍性疾病,以多发、无节律的运动性抽动和(或)发声性抽动为主要特征,且多存在注意力缺陷多动障碍、强迫障碍、情绪障碍等共患病,不管是在社会功能方面还是非社会功能方面都存在缺陷,对患儿学习、生活、社会交往造成极大危害[1]。TS的病因与发病机制尚未完全清楚,其病变部位有可能涉及皮质-纹状体-丘脑-皮质环路中的多个部位,该环路中存在多巴胺、5-羟色胺、肾上腺素、γ-氨基丁酸等中枢神经系统神经递质的分泌与代谢紊乱[2]。近年研究显示,下丘脑-垂体-肾上腺(HPA)轴功能紊乱是许多神经精神类疾病发生的病理生理学机制,也与TS关系密切[3]。西医治疗以多巴胺D受体阻滞剂为主,氟哌啶醇就是其中代表药物之一,虽能短时间改善或缓解患儿抽动症状,但服药时间长,停药后易复发,且不良反应较大[4]。耳穴疗法能够从整体调整,全面改善身体功能状态,广泛应用于临床各科疾病治疗。TS归属为中医的“慢惊风”“肝风风痰”“郁证”等范畴,实为脾虚肝亢、肝脾失调引发的情志疾患,从肝脾论治是TS治疗的关键,宜采用扶土抑木,健脾平肝的方法治疗[5]。本研究观察健脾止动汤联合耳穴贴压治疗儿童TS的疗效,探讨其对HPA轴相关激素、神经递质的影响,揭示其作用机制。现报道如下。
1 资料与方法
1.1 一般资料 选取2016年1月至2017年3月成都市新都区中医医院收治的符合《美国精神疾病诊断统计手册》第4版TS诊断标准的患儿80例作为研究对象,按照随机数字表法分为对照组和观察组,每组40例,对照组中男34例,女6例;年龄6~14岁,平均年龄(7.6±1.2)岁;病程12~66个月;平均病程(30.4±18.6)个月。观察组中男35例,女5例;年龄5~14岁,平均年龄(7.5±1.0)岁;病程14~70个月;平均病程(31.2±15.8)个月。同期入组40例健康儿童作为健康对照组,其中男35例,女5例;年龄6~14岁,平均年龄(7.8±1.1)岁,3组一般资料比较,差异无统计学意义(P>0.05),具有可比性。
1.2 诊断标准 具备主症(眨眼、摇头、耸肩、口出异声、口出秽语、咧嘴、鼓肚、甩臂、踢腿)至少1项与次症(神疲倦怠、性情急躁易怒、冲动任性、夜寐易惊、夜卧少眠、面色萎黄、食欲不振、大便溏薄)至少2项,结合舌脉,即可诊断。
1.3 纳入标准 1)符合《美国精神疾病诊断统计手册》第4版TS诊断标准;2)参照《中医儿科常见病诊疗指南》辨证为脾虚肝亢证;3)患儿监护人知情同意。
1.4 排除标准 1)入组前2周仍有使用治疗TS的其他药物;2)非TS所致的抽动症状;3)合并严重的心、肝、肾、造血系统疾病者;4)无神经系统疾病史。
1.5 脱落与剔除标准 1)出现严重不良反应;2)未能完成研究方案规定疗程。
1.6 治疗方法 对照组和观察组患儿均口服氟哌
啶醇片剂治疗,初始剂量为0.25 mg/次,3次/d,1周后逐渐增加至2 mg/次,3次/d,对照组再给予耳穴贴压治疗,分别取穴神门、胃、肾、肝、交感、皮質下穴等部位,使用无菌脱敏胶布将王不留行籽贴于上述诸穴,以患儿感觉酸麻胀痛为度,固定妥当,保留1周,每天每穴各按揉3次,耳穴贴压4次为1个疗程,治疗3个疗程,观察组再给予耳穴贴压联合健脾止动汤治疗,耳穴贴压同对照组,同时口服健脾止动汤,组方由太子参、白术、钩藤、当归、白芍、茯苓各10 g,防风、川芎、半夏、陈皮、防风各6 g,龙胆草3 g,每日1剂,早晚分服,2组均治疗12周。
1.7 观察指标 1)3组入组对象均入院时取空腹状态下取静脉血3 mL,进行中枢神经递质多巴胺(DA)、5-羟色胺(5-HT)、去甲肾上腺素(NE)、天门冬氨酸(ASP)、γ-氨基丁酸(GABA)和HPA轴相关激素皮质醇(COR)和促肾上腺皮质激素(ACTH)检测;2)对照组和观察组患儿治疗12周后再次检测中枢神经递质和HPA轴相关激素;3)对照组和观察组患儿治疗前及治疗12周后进行耶鲁综合抽动严重程度量表(TGTSS)评分[6]。
1.8 疗效判定标准 对照组和观察组患儿治疗结束后随访6个月,评估其临床疗效[7],分为显效、好转、无效,总有效率=显效例数+好转例数/总例数×100%。
1.9 统计学方法 采用SPSS 19.O统计软件进行数据分析,计量资料以均数±标准差(±s)表示,多组间比较采用单因素方差分析,两两比较用LSD检验,组内治疗前后采用配对资料t检验,计数资料以率表示,进行χ2检验,以P<0.05为差异有统计学意义。
2 结果
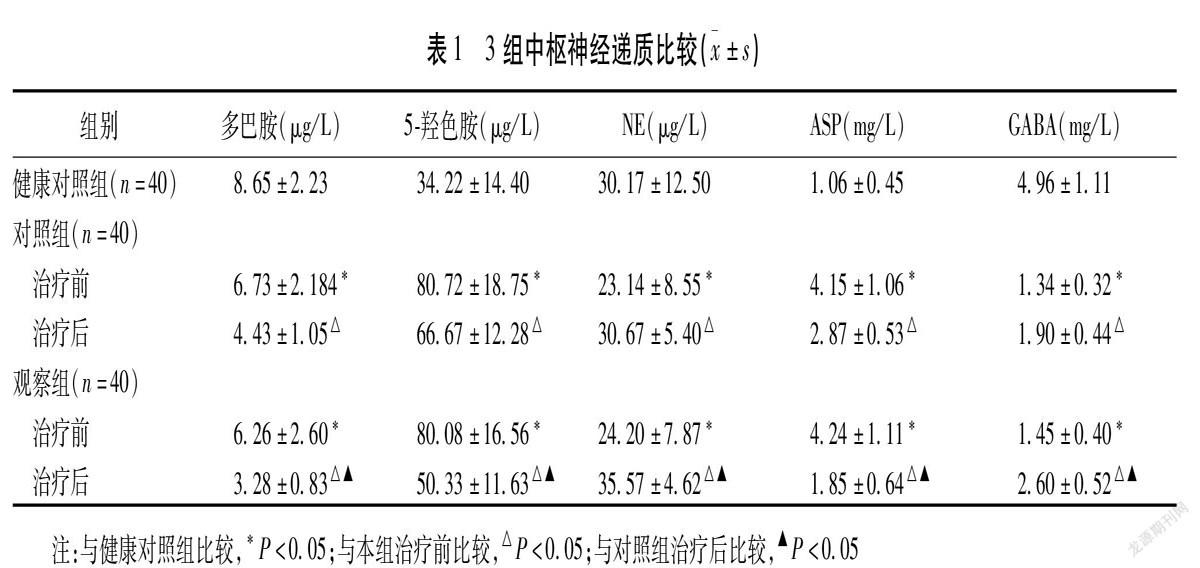
2.1 3组中枢神经递质比较 治疗前对照组和观察组的多巴胺、NE、GABA明显低于健康对照组,差异有统计学意义(P<0.05),5-羟色胺、ASP明显高于健康对照组,差异有统计学意义(P<0.05);对照组和观察组治疗后多巴胺、5-羟色胺、ASP均较治疗前明显降低,差异有统计学意义(P<0.05),NE、GABA均较治疗前明显升高,差异有统计学意义(P<0.05),且观察组治疗后多巴胺、5-羟色胺、ASP明显低于对照组,差异有统计学意义(P<0.05),NE、GABA明显高于对照组,差异有统计学意义(P<0.05)。见表1。
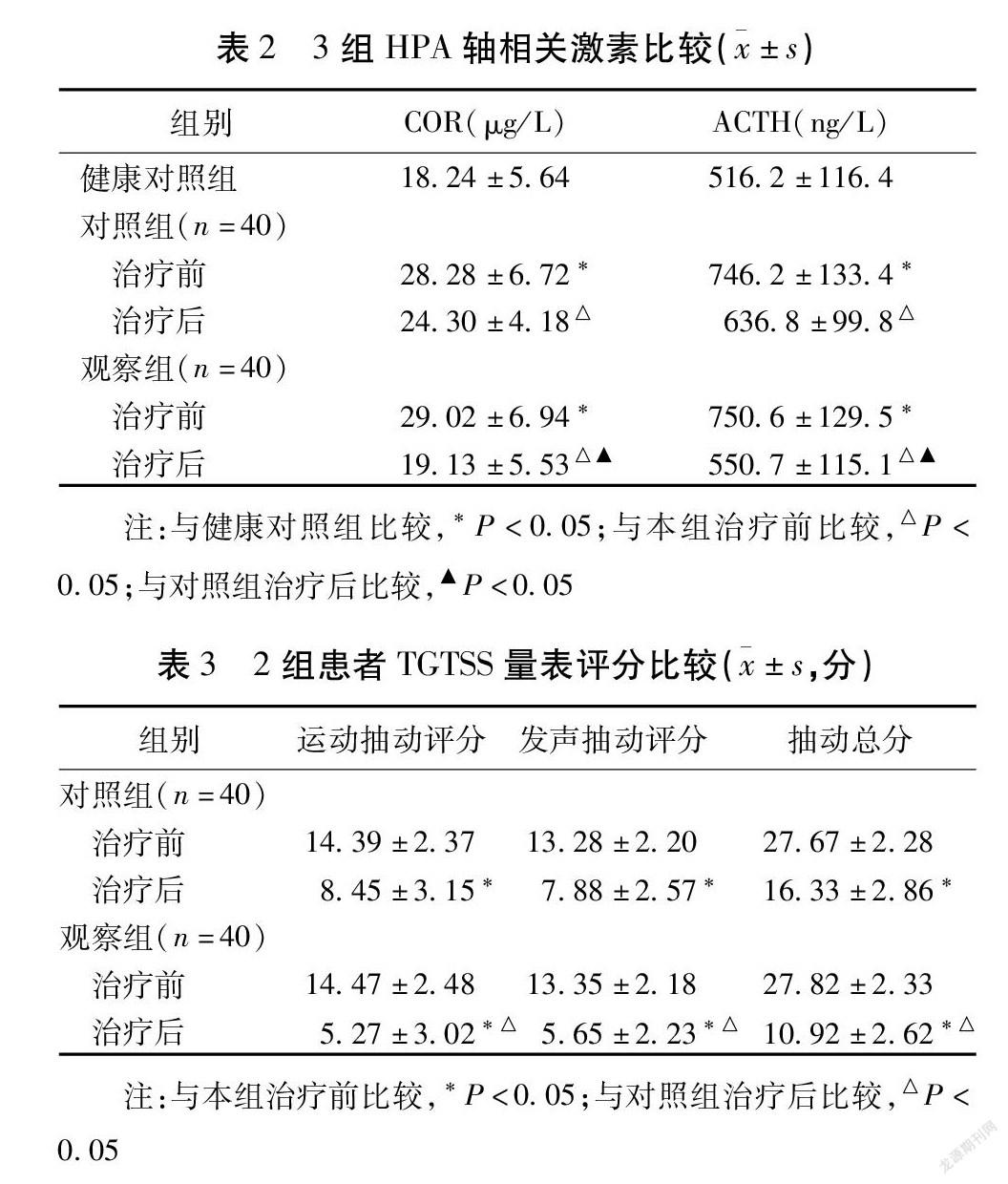
2.2 3组HPA轴相关激素比较 治疗前对照组和观察组的COR、ACTH明显高于健康对照组,差异有统计学意义(P<0.05);对照组和观察组治疗后COR、ACTH均较治疗前明显降低,差异有统计学意义(P<0.05),且观察组治疗后COR、ACTH明显低于对照组,差异有统计学意义(P<0.05)。见表2。
2.3 2组患者TGTSS量表评分比较 对照组和观察组治疗后运动抽动评分、发声抽动评分、抽动总分均较治疗前明显降低,差异有统计学意义(P<0.05),且观察组治疗后各项评分均明显低于对照组,差异有统计学意义(P<0.05)。见表3。
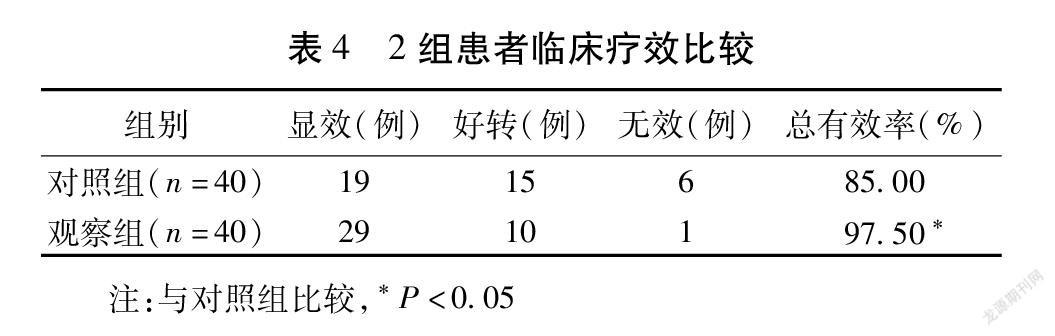
2.4 2组患者临床疗效比较 对照组和观察组的临床总有效率分别为85.00%、97.50%,差异有统计学意义,差异有统计学意义(P<0.05)。见表4。
3 讨论
多发性抽动症是儿童期常见的慢性神经精神障碍性疾病,其发病率的发病率较高,为0.15%~1.10%,男孩高于女孩[8],具有病程长、变化多、易反复、共存病较多的特点,且发病率呈逐年上升趋势,临床治疗难度高,难治性病例增多,对患儿的身心健康造成极大影响,故TS及其共患病成为儿科研究的难点和热点,逐渐引起人们的重视。
近年来,随着对TS研究的深入,除了与遗传因素有关外,还与神经递质失衡因素、病理因素、精神心理因素或环境因素等存在相关,其中多种中枢神经递质异常在发病过程中起着重要作用,如多巴胺、5-羟色胺、去甲肾上腺素、γ-氨基丁酸等递质异常[9-11],进而出现神经功能障碍。研究表明,TS患儿的多巴胺、去甲肾上腺素明显高于正常对照组[12],因而,二者可能参与TS的发病过程,多巴胺受体阻滞剂也成为西医治疗小儿多发性抽动症常用的药物。5-羟色胺是调节中枢神经系统功能的重要神经递质,具有多种生理功能,是仅次于多巴胺的单胺类神经递质,与情绪和冲动控制紧密相关,TS患儿存在5-羟色胺功能失调,表现为5-羟色胺神经元缺陷或受体的高敏感性[13],临床常见TS患儿常伴随强迫症,这与其5-羟色胺转运体的结合能力下降有关。氨基酸类神经递质分为兴奋性氨基酸和抑制性氨基酸,ASP为兴奋性氨基酸,GABA为抑制性氨基酸,兴奋性氨基酸增高或抑制性氨基酸降低可导致TS发生[14]。本研究结果显示,治疗前对照组和观察组的多巴胺、NE、GABA明显低于健康对照组,5-羟色胺、ASP明显高于健康对照组,提示TS的发病与中枢神经递质失衡有关。
下丘脑-垂体-肾上腺皮质(HPA)轴是迄今为止最重要的应激内分泌轴,在应激条件下HPA轴分泌的CRH增加,促进ACTH释放,不仅能作用于肾上腺的作用,引起糖皮质激素增加,同时还能对脑神经元直接起着神经传递、神经调整、神经激素等作用,进而对高级神经活动、精神行为如注意力、学习、记忆产生影响,同时对自发活动、情绪等均具有显著的影响[15],HPA轴功能紊乱是诸多神经精神障碍性疾病共同的病理生理学机制。研究显示,TS患儿血浆中COR、ACTH水平明显高于健康儿童,HPA轴功能亢进是患儿抽动加剧的危险因素[16-17]。本研究结果显示,治疗前对照组和观察组的COR、ACTH明显高于健康对照组,提示TS的发病与HPA轴功能亢进有关,与相关研究相似[18]。
中医药对于治疗小儿多发性抽动症具有悠久的历史,临床疗效显著,且安全性良好。健脾止动汤是四君子汤和泻青丸的合用方,全方由太子参、白术、钩藤、当归、白芍、茯苓、防风、川芎、半夏、陈皮、防风、龙胆草组成,可共奏扶土抑木功效。健脾止动汤对TS神经递质及HPA轴功能的影响研究多以动物为研究对象[19-21],而以患儿作为研究对象的研究较少。本研究结果显示,对照组和观察组治疗后多巴胺、5-羟色胺、ASP、COR、ACTH均较治疗前明显降低,NE、GABA均较治疗前明显升高,且观察组治疗后多巴胺、5-羟色胺、ASP、COR、ACTH明显低于对照组,NE、GABA明显高于对照组,提示在耳穴贴压治疗的基础上再加用健脾止动能够下调HPA轴功能,调节中枢神经递质失衡,恢复兴奋性和抑制性神经递质的失衡,达到改善运动抽动及发声抽动,提高临床治疗效果。
综上所述,TS的发病与中枢神经递质失衡及HPA轴功能亢进有关,健脾止动汤联合耳穴贴压治疗能够有效下调HPA轴功能,调节中枢神经递质失衡,协同提高临床治疗效果。
参考文献
[1]赵荣香,罗尧竞.多发性抽动症患儿预后影响因素研究分析[J].中华急诊医学杂志,2017,26(9):1089-1091.
[2]万朋,金清华.多巴胺及其受体在中枢神经系统的作用研究进展[J].武汉大学学报:医学版,2017,38(1):169-172.
[3]崔霞,于文静,张雯,等.健脾止动汤对多发性抽动症儿童HPA轴功能的影响[J].现代中医临床,2016,23(6):17-20.
[4]王敏建,陈黎明,蒋国庆.利培酮与氟哌啶醇治疗儿童抽动障碍的对照研究[J].临床精神医学杂志,2018,28(1):42-44.
[5]陈自佳,王素梅.健脾止动汤治疗儿童脾虚肝亢型多发性抽动症的安全性评价[J].北京中医药,2016,35(7):681-683.
[6]候转转,许世兵.针刺配合耳尖放血治疗小儿多发性抽动症2则[J].浙江中西医结合杂志,2016,26(4):374-376.
[7]李艷,张帆,陆超元,等.平抽方治疗儿童多发性抽动症的临床疗效研究[J].河北中医药学报,2015,30(4):4-6.
[8]钱泽全.中西医结合治疗小儿多发性抽动症80例[J].浙江中医杂志,2015,50(5):375.
[9]张璠,郑宏,马丙祥,等.六味地黄丸对多发性抽动症模型大鼠行为及脑多巴胺水平的影响[J].中医学报,2017,32(6):981-984.
[10]高汉媛,王维红,李小芹,等.菖蒲郁金汤对多发性抽动症模型大鼠单胺类神经递质的影响[J].中药药理与临床,2017,33(3):135-138.
[11]杨传楹.羚羊角胶囊联合硫必利治疗儿童多发性抽动症的临床研究[J].现代药物与临床,2018,33(5):1207-1211.
[12]于文静,白雪,张雯,等.健脾止动汤对多发性抽动症患儿神经递质的影响[J].中华中医药杂志,2015,30(5):1757-1761.
[13]姚阳,刘坤,杨宇,等.异钩藤碱对多发性抽动症模型大鼠头部抽动行为与脑内单胺递质水平的影响[J].中华行为医学与脑科学杂志,2016,25(1):29-33.
[14]王雅璇.健脾止动汤对TS模型大鼠纹状体EAAT_2表达的影响[D].北京:北京中医药大学,2016.
[15]Kapoor A,Petropoulos S,Matthews SG.Fetal programming of hypothalamic-pituitary-adrenal(HPA)axis function and behavior by synthetic glucocorticoids[J].Brain Res Rev,2008,57(2):586-595.
[16]Corbett BA,Mendoza SP,Baym CL,et al.Examining cortisol rhythmicity and responsivity to stress in children with Tourette syndrome[J].Psychoneuroendocrinology,2008,33(6):810-820.
[17]Hoekstra PJ,Dietrich A,Edwards MJ,et al.Environmental factors in Tourette syndrome[J].Neurosci Biobehav Rev,2013,37(6):1040-1049.
[18]Buse J,Kirschbaum C,Leckman JF,et al.The Modulating Role of Stress in the Onset and Course of Tourette′s Syndrome:A Review[J].Behav Modif,2014,38(2):184-216.
[19]王道涵,王素梅,趙荣华,等.多发性抽动症大鼠皮质及纹状体强啡肽表达特点及健脾止动汤干预作用[J].北京中医药大学学报,2017,40(3):188-192.
[20]丁一芸.健脾止动汤对脾虚肝旺型TS共患ADHD的临床研究[D].北京:北京中医药大学,2015.
[21]张雯,王素梅,王道涵,等.健脾止动汤对多发性抽动症模型小鼠抽动行为及纹状体内氨基酸递质的影响[J].中华行为医学与脑科学杂志,2013,22(8):700-703.
(2018-05-30收稿 责任编辑:杨觉雄)
