Synchronous resection of esophageal cancer and other organ malignancies: A systematic review
2019-07-24DimitriosPapaconstantinouDiamantisTsilimigrasDimitriosMorisAdamantiosMichalinosAikateriniMastorakiEfstratiaMpailiNatashaHasemakiAnargyrosBakopoulosDimitriosFilippouDimitriosSchizas
Dimitrios Papaconstantinou, Diamantis I Tsilimigras, Dimitrios Moris, Adamantios Michalinos,Aikaterini Mastoraki, Efstratia Mpaili, Natasha Hasemaki, Anargyros Bakopoulos, Dimitrios Filippou,Dimitrios Schizas
Abstract BACKGROUND Neoplasms arising in the esophagus may coexist with other solid organ or gastrointestinal tract neoplasms in 6% to 15% of patients. Resection of both tumors synchronously or in a staged procedure provides the best chances for long-term survival. Synchronous resection of both esophageal and second primary malignancy may be feasible in a subset of patients; however, literature on this topic remains rather scarce.AIM To analyze the operative techniques employed in esophageal resections combined with gastric, pancreatic, lung, colorectal, kidney and liver resections and define postoperative outcomes in each case.METHODS We conducted a systematic review according to PRISMA guidelines. We searched the Medline database for cases of patients with esophageal tumors coexisting with a second primary tumor located in another organ that underwent synchronous resection of both neoplasms. All English language articles deemed eligible for inclusion were accessed in full text. Exclusion criteria included: (1)Hematological malignancies; (2) Head/neck/pharyngeal neoplasms; (3) Second primary neoplasms in the esophagus or the gastroesophageal junction; (4) Second primary neoplasms not surgically excised; and (5) Preclinical studies. Data regarding the operative strategy employed, perioperative outcomes and longterm outcomes were extracted and analyzed using descriptive statistics.RESULTS The systematic literature search yielded 23 eligible studies incorporating a total of 117 patients. Of these patients, 71% had a second primary neoplasm in the stomach. Those who underwent total gastrectomy had a reconstruction using either a colonic (n = 23) or a jejunal (n = 3) conduit while for those who underwent gastric preserving resections (i.e., non-anatomic/wedge/distal gastrectomies) a conventional gastric pull-up was employed. Likewise, in cases of patients who underwent esophagectomy combined with pancreaticoduodenectomy (15% of the cohort), the decision to preserve part of the stomach or not dictated the reconstruction method (whether by a gastric pullup or a colonic/jejunal limb). For the remaining patients with coexisting lung/colorectal/kidney/liver neoplasms (14% of the entire patient population)the types of resections and operative techniques employed were identical to those used when treating each malignancy separately.CONCLUSION Despite the poor quality of available evidence and the great interstudy heterogeneity, combined procedures may be feasible with acceptable safety and satisfactory oncologic outcomes on individual basis.
Key words: Esophagectomy; Esophageal neoplasm; Second primary; Multiple primary;Concurrent neoplasms; Management
INTRODUCTION
Esophageal cancer manifesting as either squamous cell carcinoma or adenocarcinoma affects more than 450000 people worldwide and shows an increasing incidence rate over the years[1-4]. Despite innovations in the surgical management of gastrointestinal tract (GI) malignancies, esophageal cancer prognosis remains dismal with 5-year survival rates ranging from 10% to 20%[1,5-7]. Surgery is the mainstay of treatment for esophageal cancer cases amenable to resection[8,9], and represents the best choice for“cure”[10]. Patients with esophageal cancer may present with simultaneous primary malignancies in other organs, such as the stomach, colon, pancreas, liver, kidney and lungs with an estimated incidence of approximately 6%-15%[11-15]. Evidence suggests that this phenomenon may be related to the shared risk factors between esophageal and other GI tract or solid organ malignancies[7,16,17]. Due to their aggressive biologic behavior[18], esophageal carcinomas usually determine survival in these particular patients.
Synchronous resection of both esophageal and second primary malignancy may be feasible in a subset of patients. Although isolated cases have been previously reported, the literature on this topic remains rather scarce. In that context, the objective of this study was to summarize and critically evaluate all available evidence regarding the safety and feasibility of synchronous resection of esophageal carcinoma manifesting simultaneously with another primary organ malignancy. Specifically, we sought to analyze the operative interventions and outcomes of patients undergoing such extensive procedures.
MATERIALS AND METHODS
Data source and literature screening
A systematic literature search was performed utilizing Medline/PubMed database until December 2018. This systematic review adhered to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The following MESH terms were used in various combinations along with Boolean operators (AND, OR, NOT): “Esophageal neoplasms”, “Neoplasms second primary”,“Esophagectomy”, “Neoplasms multiple primary”, “adenocarcinoma”, “squamous cell carcinoma”, “synchronous” and “surgery”. Two independent authors (DP, DS)meticulously searched for potentially eligible articles retrieved after applying the initial search algorithm. Disagreements were resolved by consensus with a third author (DIT). References of the included studies were manually assessed to detect any missing study.
Inclusion/exclusion criteria and outcomes of interest
Studies were considered eligible if all of the following criteria were met: (1) Data reported on patients with primary esophageal cancer concurrent with a second primary neoplasm originating from an organ other than the esophagus; (2) Both neoplasms were treated with surgical excision. Exclusion criteria included: (1)Hematological malignancies; (2) Head/neck/pharyngeal neoplasms; (3) Second primary neoplasms in the esophagus or the gastroesophageal junction; (4) Second primary neoplasms not surgically excised; (5) Preclinical; and (6) Non-English studies.In case of overlapping population, only the latest or the most informative studies were included in the final analysis. The main outcomes of interest were the surgical strategy employed in the management of both esophageal and concurrent primary non-esophageal neoplasms as well as the related postoperative outcomes. Descriptive statistics are employed for data presentation.
Definitions
During pooled data assessment, we used the following definitions: (1) Transthoracic esophagectomy (TTE) incorporates all esophagectomy procedures employing a thoracotomy (namely Transthoracic Two-field Esophagectomy and Transthoracic Three-field Esophagectomy); (2) Non-anatomic gastric resection refers to gastric preserving gastrectomy other than total/subtotal/distal gastrectomy; (3) Anterior resection refers to resection of either the sigmoid colon or the upper part of the rectum.
RESULTS
Study and patient characteristics
The flowchart of the search strategy is depicted in Figure 1. In brief, the initial search yielded 417 results of which a total of 24 studies met the aforementioned inclusion/exclusion criteria[19-42]and thus were included in the analysis. Eligible studies were published between 1994 and 2015. Among them, 6 were single center retrospective studies[19,21,26,36,38,39], while the remaining 18 were case reports or caseseries[20,22-25,27-35,37,40-42]. A total of 117 patients with esophageal malignancies coexistingwith other primary malignancies were identified. Patient demographics were reported on 44 patients, of which, 37 (84%) were reported to be males and 7 (16%)females. The mean patient age was 59.1 years. Data on the location and histology of the esophageal tumors as well as the coexisting primary tumors are presented in Table 1.
Coexisting primary malignancies
Stomach: A total of 85 patients (71% of the entire cohort) had concurrent neoplasms of the esophagus and the stomach. Histology of gastric cancer yielded adenocarcinomas in 75 patients and gastrointestinal stromal tumors (GISTs) in the remaining 10 patients. Regarding the type of esophagectomy employed, 83 patients underwent a TTE, one patient underwent a transhiatal esophagectomy (THE) while another one underwent esophagectomy via a thoracoabdominal approach. In the same patient group, 26 total gastrectomies were reported, followed by a reconstruction using either a colonic conduit (n = 23) or a jejunal (n = 3) limb. The remaining 59 patients underwent gastrectomies that preserved part of the stomach, such as non-anatomic gastric resections (n = 53), distal gastric resection (n = 2) or underwent tumor excision by endoscopic submucosal dissection (n = 4). In each of these patients the stomach was utilized as a conduit for restoration of gastrointestinal continuity after esophagectomy. Preoperative diagnosis of the second primary neoplasm was available in 91% of the patients. A single minor (Clavien-Dindo II) anastomotic leak was observed; however, 4 cases of perioperative mortality were encountered (Table 2). A two-stage procedure was employed in one patient. During the follow-up period,43 deaths were recorded (Table 3), of which 35 were attributed to esophageal cancer recurrence and 8 to gastric carcinoma recurrence. Median patient follow-up (as reported in 5 out of 8 total studies) was 15 mo.
Pancreas/ampulla of Vater:A total of 6 patients (5% of the entire cohort) presented with a second primary malignancy in the pancreas or ampullary region. Four cases of pancreatic or ampullary adenocarcinomas were documented, while the remaining two cases consisted of a neuroendocrine carcinoma and a small cell carcinoma. In this subgroup of patients (Table 2), treatment consisted of 4 TTEs and 2 THEs.Furthermore, 4 patients underwent a pancreaticoduodenectomy (Whipple's procedure) followed by restitution of gastrointestinal continuity using either a colonic(n = 2) conduit or a jejunal (n = 2) limb. The remaining 2 patients received a pylorus preserving pancreaticoduodenectomy with subsequent reconstruction by means of an esophagogastrostomy (n = 1) or a colonic conduit (n = 1). There was one case of an esophageal anastomotic leak and one Grade B (according to the ISGPS definition)pancreatic fistula with no reported perioperative deaths. A two-stage procedure was employed in two patients. Preoperative diagnosis of the pancreatic and periampullary tumors was available in all cases. Follow-up monitoring of these patients was available in 4 out of 6 studies and was significant for a single death due to recurrent ampullary neoplasia (Table 3). Median follow-up was reported to be 12.5 mo.
Lung: A total of 18 patients (15% of the entire cohort) were preoperatively diagnosed with a second primary malignancy of the lung. All patients were treated with a TTE.In addition, lung directed therapies consisted of lobectomies (n = 12), segmentectomies (n = 2), bilobectomies (n = 2) and pneumonectomy (n = 1). A two-stage procedure was employed in two patients. There was one recorded case of postoperative mortality and two anastomotic leaks (Table 2). A median follow-up period of 10 mo is specified for 3 patients, while a cumulative 11% 5-year survival rate was reported for 12 patients.
Colon/rectum:Only two patients (1% of the analytic cohort) had a second primary colorectal malignancy. The surgical approach for these cases was a TTE combined with sigmoidectomy (n = 1) and an unspecified esophagectomy, combined with an anterior rectal resection (n = 1). A two-stage procedure was employed in one patient.The diagnosis of both malignancies was made preoperatively in both patients. After a median follow-up period of 9 mo both patients were reported to be in good health with no signs of disease recurrence.
Kidney:A total of 5 patients (5% of the analytic cohort) had a kidney neoplasm coexisting with an esophageal cancer. Radical nephrectomy (n = 3) combined with either a THE (n = 1) or a TTE (n = 4) were employed; preoperative diagnosis was available in every case. Two cases of postoperative anastomotic leak were described in these studies (Table 2). A two-stage procedure was employed in one patient. Followup data were available for 3 patients, which revealed no deaths or recurrences after a median 34 mo.
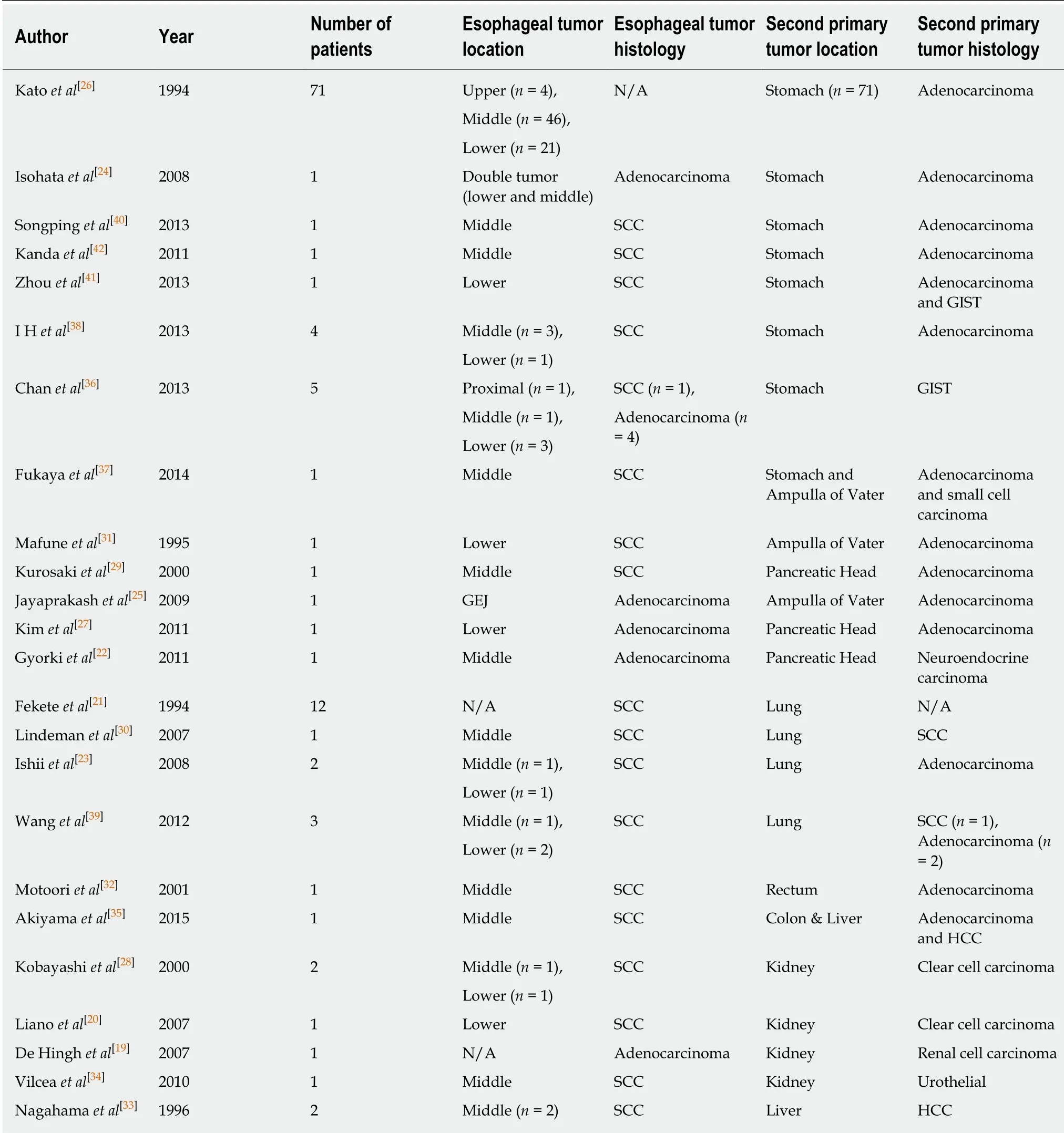
Table 1 Summary of included studies
Liver:Three patients (2% of the entire cohort) had esophageal carcinoma concurrent with hepatocellular carcinoma. These patients underwent TTE, combined with either a posterior sectionectomy (n = 2) or a liver segmentectomy (n = 1). No anastomotic leaks or postoperative mortality was reported; diagnoses of concurrent malignancies were made preoperatively (Table 2). A two-stage procedure was employed in a single patient. A median follow-up period of 17 mo was reported with one case of death due to recurrence of esophageal carcinoma (Table 3).
DISCUSSION
Coexisting primary neoplasms of the esophagus and other organs present a unique oncologic challenge that complicates surgical decision-making due to the lack of practice guidelines. Suzuki et al[43]postulated that synchronous resection of such neoplasms does indeed provide a benefit to survival but despite this initial report,evidence regarding the management of such patients remains rather scarce, as yet.The current study is important because we sought to critically evaluate the existing literature on the surgical approaches and operative outcomes of patients diagnosed with synchronous primary neoplasms. By employing a systematic search of the literature, we identified a total of 117 patients with concurrent neoplasms in the stomach, pancreas, ampulla of Vater, lung, colon/rectum, kidney and liver.Collectively, the data suggested that synchronous resection was safe, feasible and associated with low perioperative mortality (stomach: 4/84, lung: 1/18, pancreas: 0/6,colon/rectum: 0/2, kidney: 0/5, liver: 0/3). In addition, long-term outcomes of such patients were shown to be determined by the natural history of the esophageal malignancy when synchronous gastric, lung, colorectal, renal and liver cancers were encountered. In contrast, pancreatic cancer may be the main determinant of patient long-term survival when presenting simultaneously with esophageal carcinomas.

Figure 1 Flow chart of studies selection.
The majority of the patient pools (72%) had a second primary neoplasm located in the stomach which was histologically defined as adenocarcinoma in 75 cases and as GIST in 10 cases. A TTE combined with total gastrectomy was performed in 26 patients[26,37]. Gastrointestinal reconstruction for these patients was performed using either a colonic conduit (n = 23)[26,37]or a jejunal limb (n = 3)[26]. No anastomotic leaks were reported for these patients, however one patient died in the postoperative period[26]due to unspecified complications. These procedures, although complex,present a viable solution with acceptable long-term outcomes in cases where the stomach in its entirety needs be removed[44,45]. It should be noted that these procedures, in addition to being technically demanding for the surgeon, exert a substantial impact on the physiology of the patient. To overcome this obstacle, nonanatomic gastric resections (i.e., partial or wedge resections) combined with either a transthoracic (n = 57) or a transhiatal (n = 1) esophagectomy were usually employed[24,26,36,41], followed by a reconstruction utilizing a conventional gastric pullup. Interestingly, the 46 patients presented in the study by Kato et al[26]underwent gastric preserving gastrectomies despite the probability of a compromised oncologic outcome. In the same study, a comparison of surgical outcomes between patients undergoing total gastrectomy versus patients undergoing a gastric preserving procedure seemed to favor the gastric preserving group, while maintaining comparable long-term survival outcomes between the two groups[26]. Nevertheless,the patient baseline tumor characteristics differed significantly between the compared groups and consequently the results of this study should be interpreted with caution.Three further studies[38,40,42]presented outcomes of patients treated with either distal gastrectomy[40,42]or endoscopic mucosal dissection of early gastric cancer[38]. Both approaches were safe and sufficient from an oncologic perspective for the specific subsets of patients in which they were applied. Finally, six patients were diagnosed
with GISTs removed by means of a gastric wedge resection, a procedure that is considered sufficient for these particular neoplasms, taking into account their low malignant potential[36,41]. When a total gastrectomy is mandated, both the colon and the jejunum should be considered reasonable choices for reconstruction, however the surgical team needs to weigh the oncologic advantages against any possible impediment on the patient's long term quality of life[44,46,47].
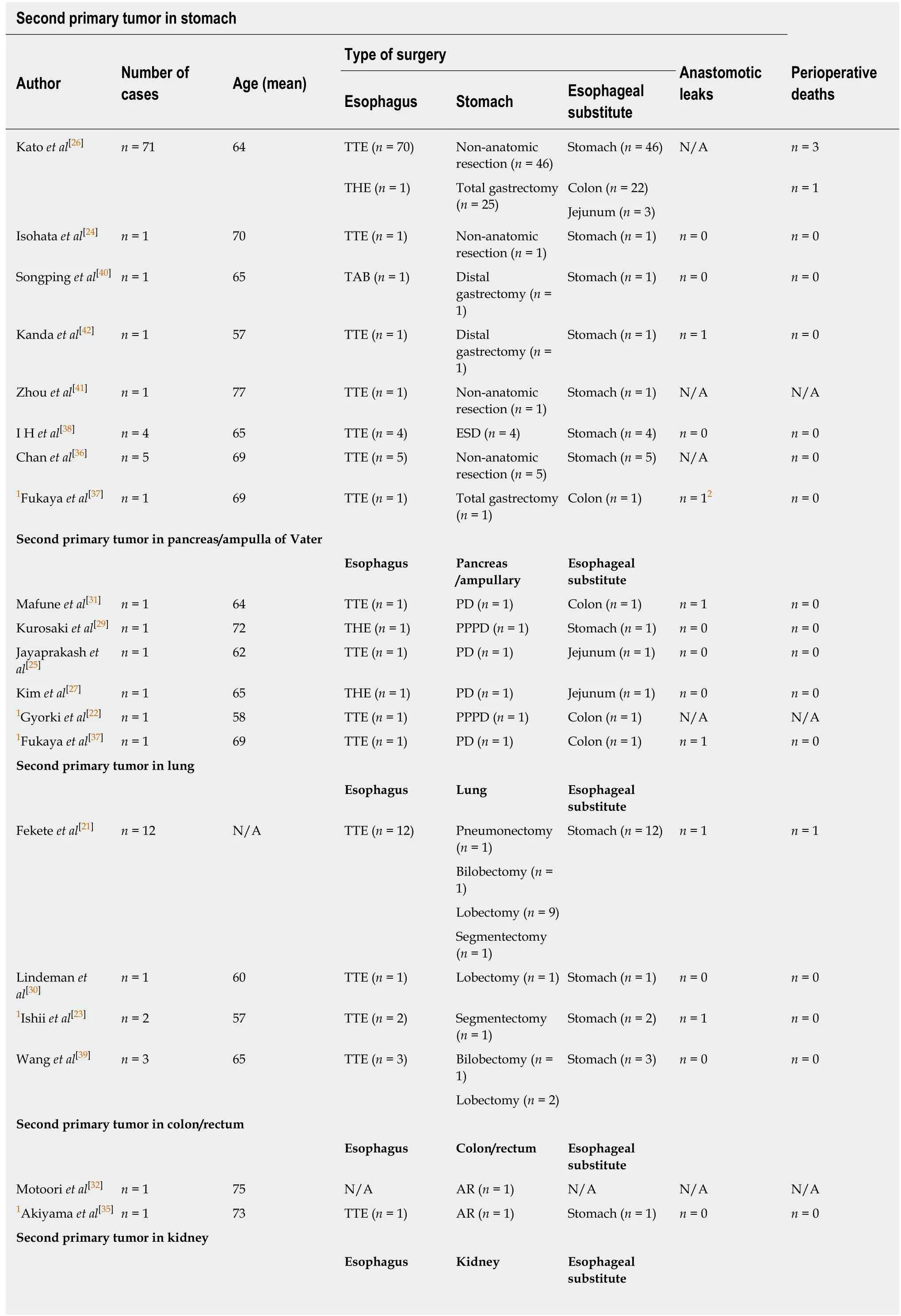
Table 2 Characteristics of patients undergoing simultaneous resection of esophageal and other organ neoplasms
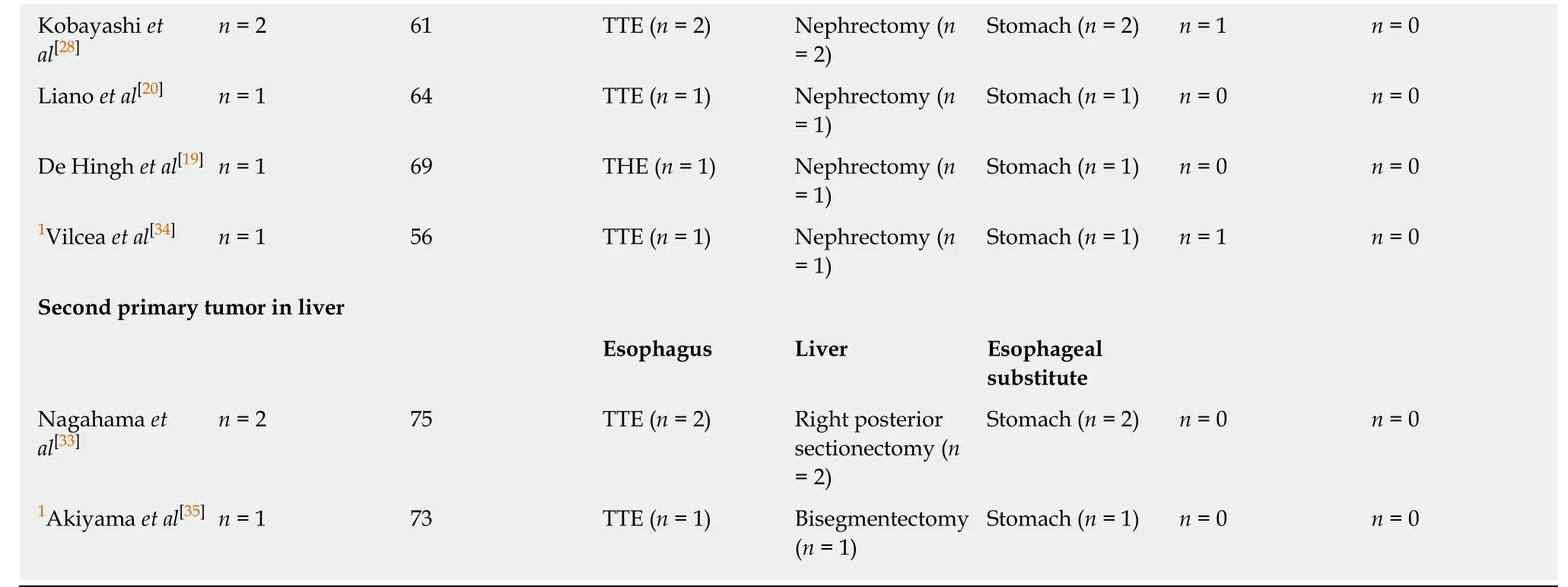
1Patients undergoing a two-stage procedure;2Anastomotic leak from pancreaticojejunal anastomosis. TTE: Transthoracic esophagectomy; THE: Transhiatal esophagectomy; TAB: Thoracoabdominal esophagectomy; PD: Pancreaticoduodenectomy; PPPD: Pylorus preserving pancreaticoduodenectomy; AR: Anterior resection; ESD: Endoscopic submucosal dissection.
Regarding the six patients that were diagnosed with simultaneous esophageal and pancreatic or ampullary malignancies, the choice of esophageal substitute depended on two factors; the need for total gastrectomy (as is the case with concomitant gastric tumors)[37]and the preservation or not of an adequate blood supply to the remnant stomach. Specifically, the preservation of the gastroduodenal artery and its gastroepiploic tributaries is a prerequisite for utilizing the stomach as an esophageal substitute[29]. When the gastroduodenal artery was sacrificed, reconstruction with either a colonic conduit[22,31]or a jejunum limb[25,27]was deemed reasonable, in a similar fashion as in cases of simultaneous esophageal and gastric resections. No patient deaths were reported, although two anastomotic leaks were identified, one from a pancreaticojejunal anastomosis[37]and one from a case in which colonic interposition was used for reconstruction[31].
Eighteen patients were identified having esophageal and lung primary malignancies. For these patients, a transthoracic approach was mandatory in order to address both tumors simultaneously. The choice of side for the thoracotomy was dictated by the side of the lung neoplasia (no bilateral thoracotomies were reported)and gastrointestinal restitution was performed using a gastric conduit. According to the presented data, a left thoracic approach (instead of the standard right thoracotomy), combined with a cervical and abdominal incision might be adequate for excising both concurrent neoplasms and their respective lymphatic basins[39].Despite the extensive dissection taking place in the thoracic cavity, only one case of a perioperative death[21]and two cases of anastomotic leaks[21,23]were encountered (Table 2). For the remaining 11 patients with concurrent esophageal and colorectal/kidney/liver neoplasms, the operative technique employed was identical to the one used when treating each malignancy separately. Perioperative mortality was equally low to the previously discussed subgroups of patients, with no deaths being reported and two anastomotic leaks occurring in patients undergoing simultaneous esophagectomy and nephrectomy[28,34].
In order to mitigate the detrimental consequences of a long operative procedure and decrease the devastating consequences of a potential anastomotic leak, several authors opted for a two-staged operative procedure in which GI restitution was accomplished several days after the initial excision stage[22,23,34,35,37]. Establishing the diagnosis of concurrent second primary malignancies before esophageal surgery was possible for the majority of treated patients in our study (113 patients, 96% of the patient pool) thus facilitating the preoperative planning of a combined procedure.Lastly, a major concern when performing simultaneous combined procedures for malignancies is the oncologic long-term outcome. Long term follow-up was available in 16 studies[20,23-26,28-33,35-38,42](Table 3). In the subgroup of patients with identified gastric second primary neoplasms, out of a total of 85 patients, 34 patients died of esophageal cancer recurrence while 8 died of second primary neoplasm recurrence. The observed lower mortality due to gastric neoplasm recurrences is in part due to the inclusion of GISTs in the analysis. Despite this fact, individual studies demonstrate that esophageal neoplasms are associated with a higher malignant potential than gastric neoplasms[26,36,43], which is often translated to death before gastric cancer relapses.Pooled analysis of the 4 patients with pancreatic and ampullary tumors revealed one case of death from ampullary cancer recurrence, with no deaths attributed to esophageal cancer recurrence. Similarly, esophageal cancer recurrence was the primary cause of death in one of three patients with concurrent neoplasms of the esophagus and liver. No mortality from recurrences was observed in the patients with second primaries found in the lungs, colon/rectum or kidneys.
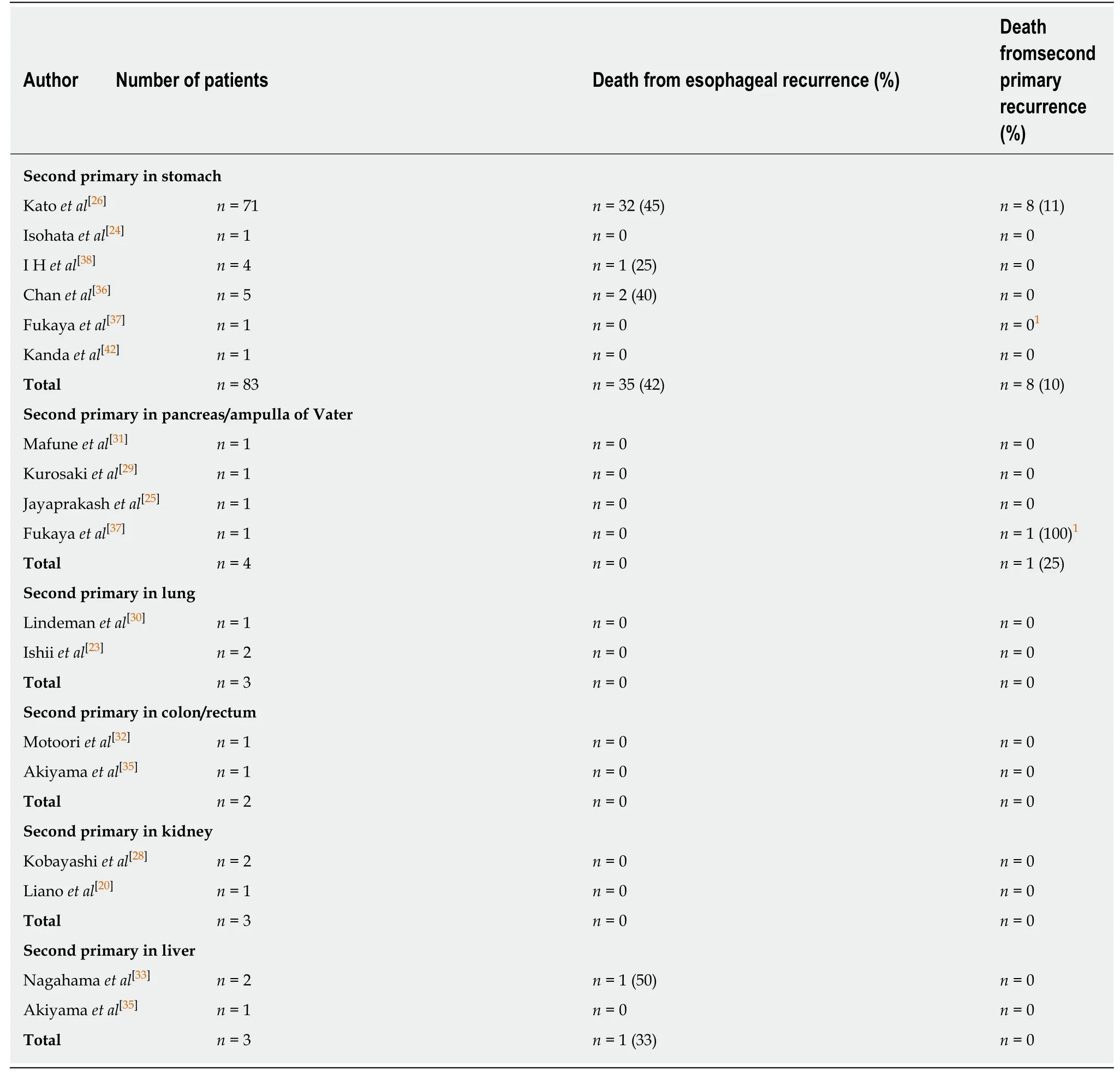
Table 3 Postoperative deaths from tumor recurrences (Follow-up period ranged from 8 mo to 7 years)
Utilization of pre-operative and post-operative chemotherapy and radiotherapy was poorly defined in the included studies. Nonetheless, given the aggressive nature of esophageal cancers[43], such patients should be treated in a multidisciplinary setting.The current study had several limitations. First, the small study sample prevents us from drawing accurate and reproducible conclusions regarding the oncologic outcomes of these patients. Second, the considerable interstudy heterogeneity, the inconsistently reported oncologic and surgical outcomes and tumor staging present major limitations in the generalizability of the included results.
In conclusion, data from this systematic review suggested that synchronous resection of esophageal and other primary solid organ malignancy was safe,technically feasible and was associated with acceptable perioperative mortality rates,on individual basis. However, emphasis should be given to the poor quality of the available evidence and the several important limitations of the included studies.Future, well-designed, larger cohort studies will be critical in identifying the optimal therapeutic strategy for patients with synchronous esophageal and organ malignancies.
ARTICLE HIGHLIGHTS
Research background
Esophageal cancer is well known for its lethality and poor prognosis when treated with modalities other than surgery. Esophageal cancer shares many risk factors with other gastrointestinal tract and solid organ neoplasms, a fact which explains why the malignancies may coexist with other tumors of the stomach, colon, liver, pancreas, lung and kidney. This phenomenon is both rare and underreported and when encountered by a treating physician it creates confusion and uncertainty as to what treatment course should be employed, given the lack of relevant practice guidelines. In the present study, by employing a systematic literature review protocol, we sought to elucidate the role of surgical therapy is these patients, the operative techniques applicable in each case and the perioperative and postoperative outcomes that are to be expected.
Reasearch motivation
Summing all available studies concerning patients with coexisting neoplasms of the esophagus and other organs will hopefuly guide patient care and emphasize the need of better and more accurate reporting of such patients.
Research objectives
To identify the operative approaches utilized when synchronously treating neoplasms of the esophagus and the stomach/pancreas/lung/colon/rectum/liver/kidney, their perioperative safety and postoperative outcomes.
Reaseach methods
We systematically reviewed all existing literature for studies including patients with esophageal cancer and a second primary neoplasm. Studies that included patients who exhibited a second primary neoplasm in an organ other than the head and neck region were included in the analysis. Afterwards, we extracted information pertaining to the intricacies of the operative technique employed, anastomotic leaks, perioperative deaths and neoplasm recurrences.
Research results
A total of 23 eligible studies were identified incorporating 117 patients. Eighty five patients had a second primary neoplassm in the stomach and underwent a total gastrectomy (n = 26) with subsequent reconstruction using a colonic (n = 23) or a jejunal (n = 3) conduit or a gastric preserving resection (n = 59) in which a gastric pull-up was used for reconstruction. One anastomotic leak and 4 deaths were recorded in this patient group, whilst follow-up revealed 35 esophageal cancer recurrences and 8 gastric cancer recurrences. Patients that underwent a combined esophagectomy and whipple procedure (n = 6) were reconstructed either by means of a gastric pull-up (n = 1) or a colon/jejunum conduit (n = 5), with 2 anastomotic leaks recorded and no perioperative deaths. Two cases of pancreatic/ampullary carcinoma recurrence were encountered during follow-up. Finaly, the remaining patients (n = 26) with second primary neoplasms in the lung, colon/rectum, kidney and liver had resections identical to those employed in treating each of these neoplasms seperately. Four anastomotic leaks and one case of perioperative mortality were reported. Follow-up was notable only for one case of esophageal cancer recurrence.
Research conclusions
The present systematic review supports the safety, efficacy and applicability of combined resections, although the poor quality of included studies limits the strength and generalizability of the results.
Research perspectives
Patients with concurrent esophageal and second primary organ neoplasms are a unique category of patients whose survival depends on quick and decisive surgical action. The lack of surgical and oncologic guidelines is therefore a major impediment in treating these unlucky patients.Better reporting of surgical outcomes in a uniform manner may pave the way for future reseach that will eventually help establish clear-cut clinical protocols and optimize therapeutic strategies.
杂志排行

World Journal of Gastroenterology的其它文章
- Diuretic window hypothesis in cirrhosis: Changing the point of view
- Fluoroquinolones for the treatment of latent Mycobacterium tuberculosis infection in liver transplantation
- Reactivation of hepatitis B virus infection in patients with hemolymphoproliferative diseases, and its prevention
- Current status of endoscopic retrograde cholangiopancreatography in patients with surgically altered anatomy
- Choledochal cysts: Similarities and differences between Asian and Western countries
- Gastro-duodenal disease in Africa: Literature review and clinical data from Accra, Ghana