Recent advances in endoscopic retrograde cholangiopancreatography in Billroth ll gastrectomy patients: A systematic review
2019-07-10TaeYoungParkTaeJunSong
Tae Young Park, Tae Jun Song
Abstract BACKGROUND Endoscopic retrograde cholangiopancreatography (ERCP) in patients with Billroth II gastrectomy has been considered a challenging procedure due to the surgically altered gastrointestinal anatomy. However, there has been a paucity of comparative studies regarding ERCP in Billroth II gastrectomy cases because of procedure-related morbidity and mortality and practical and ethical limitations.This systematic and comprehensive review was performed to obtain a recent perspective on ERCP in Billroth II gastrectomy patients.AIM To systematically review the literature regarding ERCP in Billroth II gastrectomy patients.METHODS A systematic review was performed on the literature published between May 1975 and January 2019. The following electronic databases were searched:PubMed, EMBASE, and Cochrane Library. The outcomes of successful afferent loop intubation and successful selective cannulation and occurrence of adverse events were assessed.RESULTS A total of 43 studies involving 2669 patients were included. The study designs were 36 (83.7%) retrospective cohort studies, 4 (9.3%) retrospective comparative studies, 2 (4.7%) prospective comparative studies, and 1 (2.3%) prospective cohort study. Of a total of 2669 patients, there were 1432 cases (55.6%) of sideviewing endoscopy, 664 (25.8%) cases of forward-viewing endoscopy, 171 (6.6%)cases of balloon-assisted enteroscopy, 169 (6.6%) cases of anterior obliqueviewing endoscopy, 64 (2.5%) cases of dual-lumen endoscopy, 31 (1.2%) cases of colonoscopy, and 14 (0.5%) cases of multiple bending endoscopy. The overall success rate of afferent loop intubation was 91.3% (2437/2669), and the overall success rate of selective cannulation was 87.9% (2346/2437). A total of 195 cases(7.3%) of adverse events occurred. The success rates of afferent loop intubation and the selective cannulation rate for each type of endoscopy were as follows:side-viewing endoscopy 98.2% and 95.3%; forward-viewing endoscopy 97.4%and 95.2%; balloon-assisted enteroscopy 95.4% and 97.5%; oblique-viewing endoscopy 94.1% and 97.5%; and dual-lumen endoscopy 82.8% and 100%,respectively. The rate of bowel perforation was slightly higher in side-viewing endoscopy (3.6%) and balloon-assisted enteroscopy (4.1%) compared with forward-viewing endoscopy (1.7%) and anterior oblique-viewing endoscopy(1.2%). Mortality only occurred in side-viewing endoscopy (n = 9, 0.6%).CONCLUSION The performance of ERCP in the Billroth II gastrectomy population has been improving with choice of various type of endoscope and sphincter management.More comparative studies are needed to determine the optimal strategy to perform safe and effective ERCP in Billroth II gastrectomy patients.
Key words: Endoscopic retrograde; Cholangiopancreatography; Therapeutic; Endoscope;Billroth II operation; Adverse event; Systematic review
INTRODUCTION
Billroth II gastrectomy commonly encounters a challenging surgically altered anatomy when performing endoscopic retrograde cholangiopancreatography (ERCP).The difficulties in performing ERCP in patients with Billroth II gastrectomy include the identification and intubation of the afferent loop, visualization of the papilla,selective cannulation of the desired biliary or pancreatic duct, and sphincter therapy due to the reverse direction of the papilla[1,2]. As a result, the safety and failure of ERCP have always been a major concern in Billroth II gastrectomy patients.
For successful and safe ERCP in Billroth II gastrectomy patients, there have been many choices for the selection of endoscopy other than conventional side-viewing endoscopy, such as forward-viewing endoscopy (with or without cap-fitting)[3,4],balloon-assisted enteroscopy (single-balloon or double-balloon)[5,6], anterior obliqueviewing endoscopy (with or without overtube-assisted)[7,8], dual-lumen endoscopy[9],and multiple bending endoscopy[10]; choices for sphincter therapy, such as endoscopic sphinc-terotomy (EST), endoscopic papillary balloon dilation (EPBD), and endoscopic papillary large balloon dilation (EPLBD)[11-13]; and choices for accessories, such as a needle knife (NK) and rotatable or dedicated inverted papillotome[14,15].
To date, there has been a paucity of comparative studies regarding ERCP in Billroth II gastrectomy cases because of procedure-related morbidity and mortality and practical and ethical limitations. To obtain a more recent perspective on ERCP in Billroth II gastrectomy, we systematically and comprehensively reviewed the literature regarding ERCP in Billroth II gastrectomy patients. In detail, the aims of our study were: (1) To assess the success rate of afferent loop intubation, the success rate of selective cannulation, and rate of adverse events in ERCP in Billroth II gastrectomy patients; (2) To assess these outcomes according to each type of endoscopy; (3) To assess clinical efficacy according to each type of sphincter management methods.
MATERIALS AND METHODS
Search strategy and study selection
This systematic review was conducted according to the PRISMA guidelines[16].Electronic databases, including MEDLINE (PubMed), EMBASE, and Cochrane Library, were searched for all studies published from May 1975 to January 2019. The search terms included “Billroth II gastrectomy” or “Billroth II operation,” or“gastrectomy” and “endoscopic retrograde cholangiopancreatography” or“endoscopic retrograde” combined with “cholangiopancreatography,” or “ERCP.”Two investigators (T.Y.P. and T.J.S.) independently performed the search of the electronic databases and assessed the eligibility of all the studies searched from the databases according to the predetermined selection criteria. Disagreements between evaluators were resolved through discussion.
Studies were included in the systematic review if they met all of the following criteria: (1) Relevant clinical studies of ERCP in patients with prior Billroth II gastrectomy; (2) Studies that enrolled at least 10 Billroth II gastrectomy patients; (3)Studies with full text available; (4) Studies with available information on the patient number, indications for the ERCP, type of endoscopy, type of sphincter therapy,success rate of afferent loop intubation, success rate of selective cannulation,occurrence of adverse events including bowel perforation, post-ERCP pancreatitis,bleeding, cardiopulmonary events and mortality; and (5) Studies written in English.Studies were excluded from the current review if they met any of the following criteria: (1) Irrelevancy to ERCP in Billroth II gastrectomy patients; (2) Fewer than ten patients; (3) Review, abstract only article, commentary, and letter; (4) Non-human study; and (5) Languages other than English.
Statistical analysis
The primary outcome was to assess the efficacy of ERCP in Billroth II gastrectomy patients by afferent loop intubation and the selective cannulation of the desired duct as well as the safety according to procedure-related adverse events, such as bowel perforation, post-ERCP pancreatitis, bleeding, cardiopulmonary events, and mortality. The secondary outcome was to compare the rate of afferent loop intubation,selective cannulation, and adverse events according each type of endoscope. The categorical variables were reported as the frequency with respective proportions(percentages). The pooled rate of outcome measures was calculated by dividing the percentage of patients or procedures from the included studies.
RESULTS
Literature search and identification of relevant studies
The flow diagram of the study identification, screening, eligibility, and inclusion process is shown in Figure 1. A total of 344 studies were identified through an electronic search of 3 databases and manual search of the relevant bibliographies. Of them, 79 duplicate studies were removed during the initial screening. Then, through a review of the titles and abstracts, 100 studies irrelevant to ERCP in Billroth II gastrectomy patients were excluded. After a thorough review of 265 relevant studies,222 studies were excluded from the systematic review. The reasons for study exclusion were as follows: Case report (n = 28), languages other than English (n = 26),fewer than 10 patients (n = 25), review (n = 15), abstract (n = 13), letter (n = 7),commentary (n = 6), and non-human study (n = 2). The remaining 43 studies were included in the final analysis.
Characteristics of the studies included in the final review
The characteristics of the 43 studies are listed in Table 1. The published year ranged from 1984 to 2018. Most of the studies were retrospective single-arm studies, and the most common indications for ERCP were common bile duct (CBD) stones and pancreaticobiliary malignancies. There were six studies that included more than 100 Billroth II gastrectomy patients and, among them, three studies[17-19]were published in recent years. The detailed characteristics of the recently published studies including more than 100 Billroth II gastrectomy cases are summarized in Table 2.
Results of the systematic review
The results of the current systematic review are shown in Table 3. Of the 43 included studies, there were 36 (83.7%) retrospective cohort studies, 4 (9.3%) retrospective comparative studies, 2 (4.7%) prospective comparative studies, and 1 (2.3%)prospective cohort study. There were 2669 identified patients in total. Conventional side-viewing endoscopy (n = 1432, 55.6%) and forward-viewing endoscopy with or without cap-fitting (n = 664, 25.8%) were the most frequently used types of endoscopy when performing ERCP in Billroth II gastrectomy patients. The other types of endoscopy that were used were balloon-assisted enteroscopy in 171 cases (6.6%),anterior oblique-viewing endoscopy in 169 cases (6.6%), dual-lumen endoscopy in 64 cases (2.5%), colonoscopy in 31 (1.2%), and multiple bending endoscopy in 14 cases(0.5%). The overall success rate of afferent loop intubation was 91.3% (2437/2669), and the overall success rate of selective cannulation was 87.9% (2346/2437). A total of 195 cases (7.3%) of adverse events occurred. These events were bowel perforations in 74 cases (2.8%), post-ERCP pancreatitis in 65 cases (2.4%), bleeding in 37 cases (1.4%),mortality in 9 cases (0.3%), cholangitis in 7 cases (0.1%), respiratory insufficiency in 1 case (0.04%), aspiration pneumonia in 1 case (0.04%), and cholecystitis in 1 case(0.04%). All the mortality cases (n = 9, 0.3%) occurred in procedures using conventional side-viewing endoscopy.
Subgroup analysis
The subgroup analysis according to the type of endoscopy is summarized in Table 4.The success rates of afferent loop intubation by each type of endoscopy ranged from 82.8% to 98.2%. The success rates of selective cannulation ranged from 95.2% to 100%.The occurrence rate of adverse events by each type of endoscopy ranged from 3.6% to 7.9%. The rates of afferent loop intubation, selective cannulation, and adverse events were similar between side-viewing endoscopy and forward-viewing endoscopy,which are the most frequently used types of endoscopy in ERCP in patients with Billroth II gastrectomy. The rates of bowel perforation were slightly higher in sideviewing endoscopy (3.6%) and balloon-assisted enteroscopy (4.1%) compared with forward-viewing endoscopy (1.7%) and anterior oblique-viewing endoscopy (1.2%).Mortality only occurred in side-viewing endoscopy (n = 9, 0.6%).
The subgroup analysis by each type of sphincter management summarized in Table 5. The clinical success rates of achievement for the planned therapeutic goals according to the sphincter management ranged from 85.8% to 93.6%. The overall rate of adverse events according to the sphincter therapy ranged from 5.8% to 8.5%. The rate of bowel perforation ranged from 1.3% to 3.5%. The most cases of post-ERCP pancreatitis occurred in patients who underwent EPBD (6.5%). Most of the bleeding occurred in whom EST was used (EST, n = 25; EST+EPBD, n = 8; EPBLD, n = 3).
DISCUSSION
The gastric bypass surgery was first introduced in 1879 by Jules Emile Pean and 1880 by Ludwik Rydygier[20]. The gastrectomy with gastrojejunal anastomosis (Billroth II gastrectomy) is the most modern form of gastric bypass surgery, which was first performed in 1885 by Theodor Billroth[21]. Now, Billroth II gastrectomy has been widely used to treat gastric malignancy, refractory peptic ulcer disease with pyloric stenosis, or peptic ulcer perforation[22]. There are several types of Billroth II anastomosis according to reconstruction following partial gastrectomy such as antecolic or retrocolic, anisoperistaltic or isoperistaltic with or without Roux-en-Y anastomosis.
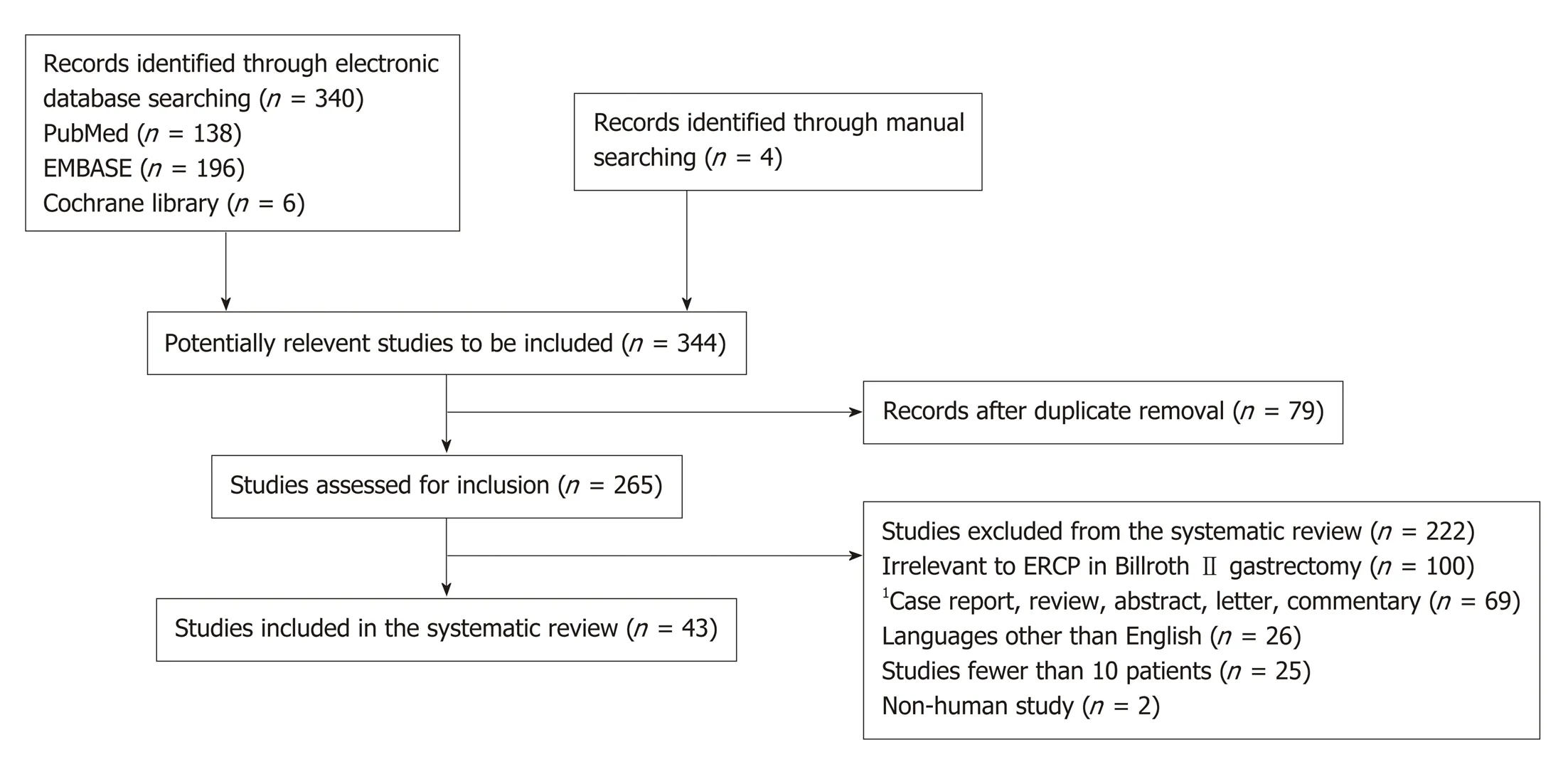
Figure 1 Flow diagram of the study.1Case report (n = 28), review (n = 15), abstract (n = 13), letter (n = 7), and commentary (n = 6).
ERCP in Billroth II gastrectomy patients is a challenging procedure. The difficulties in performing ERCP in Billroth II gastrectomy are selective intubation of the endoscope into the afferent loop due to the acute angulation of the remnant stomach and small bowel, identification of papilla behind the mucosal fold, selective cannulation of the desired pancreaticobiliary duct, and optimal sphincter therapy due to the inverted position[23]. Particularly, because of procedure-related morbidity and mortality, there has been a paucity of prospective controlled studies in this population, and the treatment strategy or instrument decision, including the choice of endoscope or sphincter therapy, has been determined according to the endoscopists'preference based on their education and experience.
Toward evening, when the sun was very low and its rays were no longer hot, the Tsar s daughter, Helen the Beautiful, went into the garden to walk with her nurse and the ladies-in-waiting of the Court. When she came near, suddenly the Gray Wolf leaped over the railing into the garden, seized her and ran off with her more swiftly than twenty horses. He ran to the open field, to the green oak tree where Tsarevitch Ivan was waiting, and set her down beside him. Helen the Beautiful had been greatly frightened, but dried her tears quickly when she saw the handsome youth.
The choice of endoscopy has always been a matter of controversy, and there is no consensus on the issues. Experienced endoscopists usually recommend using a conventional side-viewing endoscope because it has an elevator and a large working channel. However, a side-viewing endoscope has some limitations when used on Billroth II gastrectomy patients because of its limited visibility due to presenting a side view, rigidity and relatively large diameter of the scope. Therefore, in Billroth II gastrectomy patients, ERCP using a side-viewing endoscope may sometimes be difficult, and it may be associated with a risk of small bowel or an anastomosis site perforation, particularly for inexperienced endoscopists. By contrast, insertion of a forward-viewing endoscope may be relatively easy and safe, and various interventions can also be performed safely. Consequently, the use of a forwardviewing endoscope with or without cap-fitting has become more frequent and now is the second most common type of endoscope for ERCP in Billroth II gastrectomy patients despite its disadvantages, such as absence of an elevator, small working channel, and difficulty in obtaining an en face view of the papilla (Figures 2 and 3).
Recently, a meta-analysis[24]that focused on the efficacy and safety of forwardviewing endoscopy for ERCP in Billroth II gastrectomy compared with conventional side-viewing endoscopy was reported. The meta-analysis showed a higher success rate for afferent loop intubation in forward-viewing endoscopy (with or without capfitting) compared to that for conventional side-viewing endoscopy (90.3% vs 86.8%).Furthermore, the success rate of selective cannulation in cap-fitting forward-viewing endoscopy has been reported up to 93.7%. This result suggested that forward-viewing endoscopy with or without cap-fitting can be a potential alternative type of endoscopy for ERCP in Billroth II gastrectomy cases, particularly when conventional side-viewing endoscopy fails and balloon-assisted enteroscopy is unavailable. A forward-viewing endoscopy with or without cap-fitting could be the initial choice of endoscopy for an inexperienced endoscopist to minimize the risk of adverse events,such as bowel perforation. However, the studies included in this meta-analysis were non-comparative and had a retrospective design, and therefore, the applicability of their pooled estimate results to general practice might be limited.
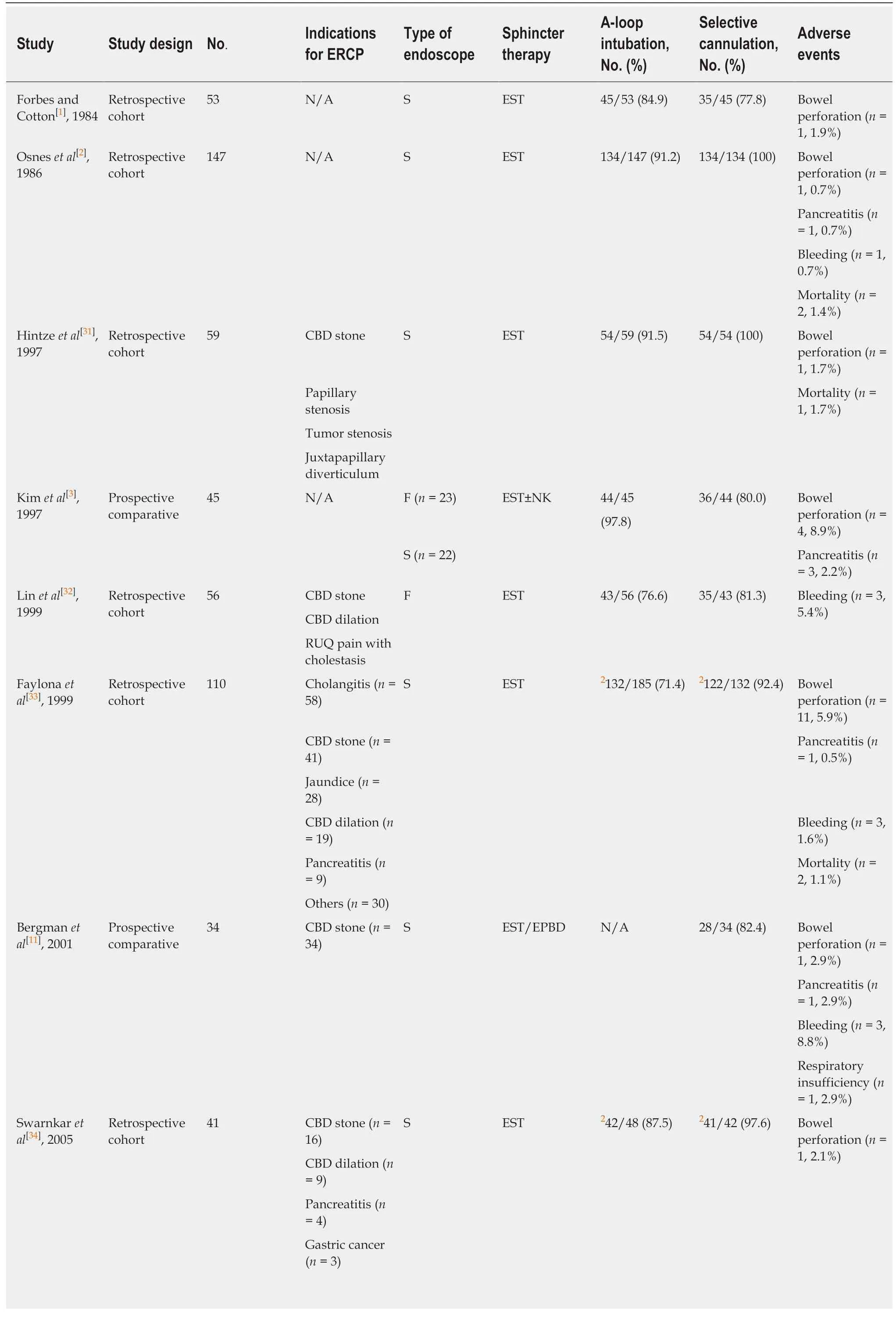
Table 1 Characteristics of the 43 studies included in the systematic review
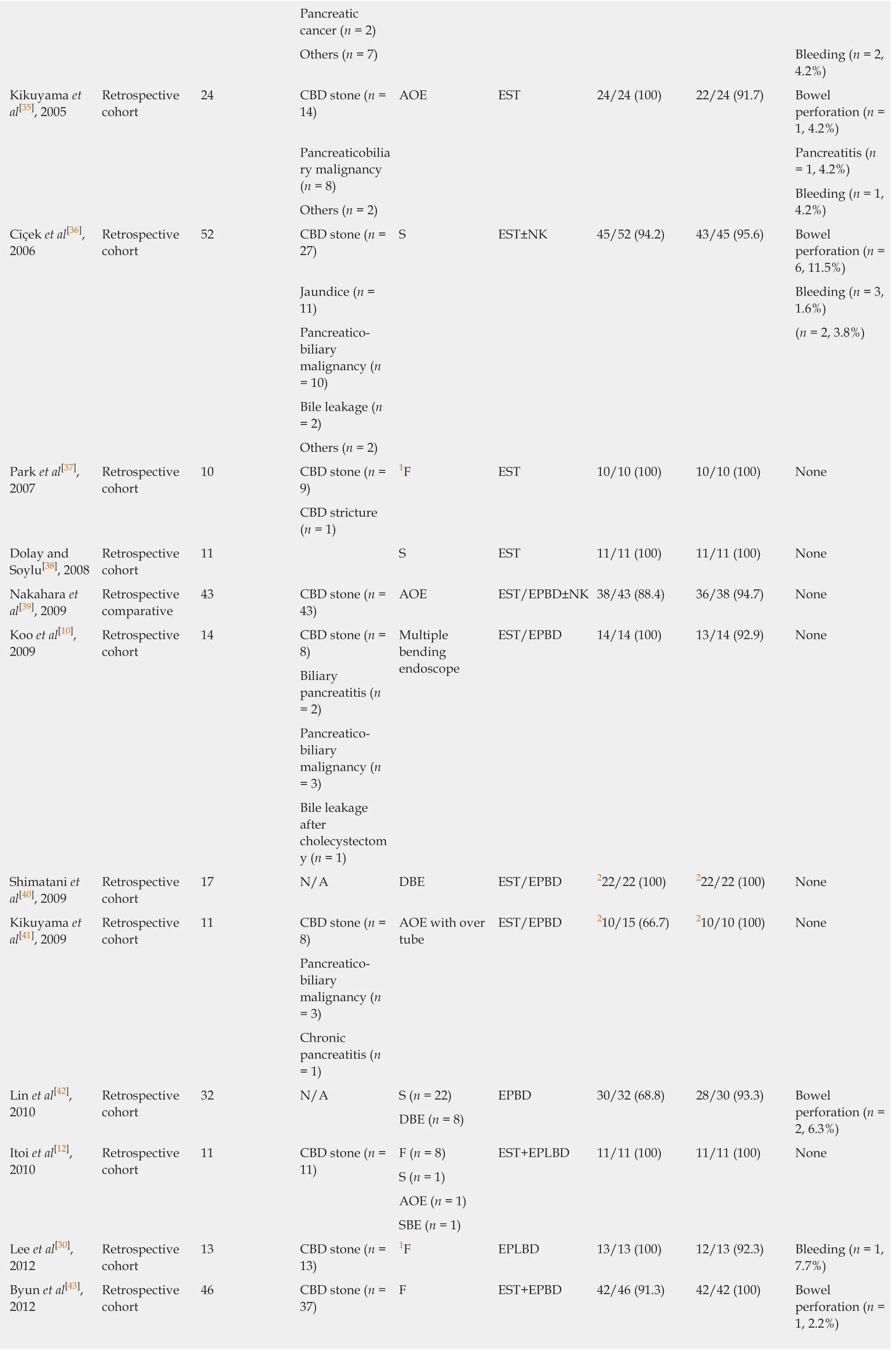
Pancreatic cancer (n = 2)Others (n = 7) Bleeding (n = 2,4.2%)Kikuyama et al[35], 2005 Retrospective cohort 24 CBD stone (n =14)AOE EST 24/24 (100) 22/24 (91.7) Bowel perforation (n =1, 4.2%)Pancreaticobilia ry malignancy(n = 8)Pancreatitis (n= 1, 4.2%)Bleeding (n = 1,4.2%)Others (n = 2)Ciçek et al[36],2006 Retrospective cohort 52 CBD stone (n =27)S EST±NK 45/52 (94.2) 43/45 (95.6) Bowel perforation (n =6, 11.5%)Jaundice (n =11)Bleeding (n = 3,1.6%)Pancreaticobiliary malignancy (n= 10)(n = 2, 3.8%)Bile leakage (n= 2)Others (n = 2)Park et al[37],2007 Retrospective cohort 10 CBD stone (n =9)1F EST 10/10 (100) 10/10 (100) None CBD stricture(n = 1)Dolay and Soylu[38], 2008 Retrospective cohort 11 S EST 11/11 (100) 11/11 (100) None Nakahara et al[39], 2009 Retrospective comparative 43 CBD stone (n =43)AOE EST/EPBD±NK38/43 (88.4) 36/38 (94.7) None Koo et al[10],2009 Retrospective cohort 14 CBD stone (n =8)Multiple bending endoscope EST/EPBD 14/14 (100) 13/14 (92.9) None Biliary pancreatitis (n= 2)Pancreaticobiliary malignancy (n= 3)Bile leakage after cholecystectom y (n = 1)Shimatani et al[40], 2009 Retrospective cohort 17 N/A DBE EST/EPBD 222/22 (100) 222/22 (100) None Kikuyama et al[41], 2009 Retrospective cohort 11 CBD stone (n =8)AOE with over tube EST/EPBD 210/15 (66.7) 210/10 (100) None Pancreaticobiliary malignancy (n= 3)Chronic pancreatitis (n= 1)Lin et al[42],2010 Retrospective cohort 32 N/A S (n = 22) EPBD 30/32 (68.8) 28/30 (93.3) Bowel perforation (n =2, 6.3%)DBE (n = 8)Itoi et al[12],2010 Retrospective cohort 11 CBD stone (n =11)F (n = 8) EST+EPLBD 11/11 (100) 11/11 (100) None S (n = 1)AOE (n = 1)SBE (n = 1)Lee et al[30],2012 Retrospective cohort 13 CBD stone (n =13)1F EPLBD 13/13 (100) 12/13 (92.3) Bleeding (n = 1,7.7%)Byun et al[43],2012 Retrospective cohort 46 CBD stone (n =37)F EST+EPBD 42/46 (91.3) 42/42 (100) Bowel perforation (n =1, 2.2%)
Pancreaticobiliary malignancy (n= 5)Pancreatitis (n= 1, 2.2%)Benign biliary stricture (n = 4)Choi et al[44],2012 Retrospective comparative 26 CBD stone (n =26)S (n = 13) EST±EPBD 26/26 (100) 26/26 (100) None F (n = 13)Kianicka et al[45], 2012 Retrospective cohort 120 Cholestasis (n =100)F EST 109/120 (90.8) 109/120 (90.8) Bowel perforation (n =1, 0.8%)Biliary pancreatitis (n= 12)Pancreatitis (n= 2, 1.7%)Acute cholangitis (n =6)Bleeding (n = 2,1.7%)Bile leakage (n= 2)Osoegawa et al[27], 2012 Retrospective cohort 15 N/A DBE EST/EPBD±NK218/19 (94.7) 216/18 (88.9) Bowel perforation (n =1, 0.5%)Sen-Yo et al[46],2012 Retrospective comparative 65 CBD stone (n =38)AOE EST/EPBD±NK60/65 (92.3) 60/60 (100) Bowel perforation (n =1, 1.5%)Pancreaticobiliary malignancy (n= 17)Pancreatitis (n= 3, 4.6%)Cholangitis (n =2, 3.0%)Other malignancy (n= 2)Chronic pancreatitis (n= 2)Bile leakage (n= 2)Others (n = 4)Jang et al[47],2013 Retrospective cohort 40 CBD stones (n =40)S EPLBD±NK 40/40 (100) 40/40 (100) Pancreatitis (n= 2, 5.0%)Yao et al[9],2013 Retrospective cohort 46 CBD stone (n =38)Dual-lumen gastroscope EST/EPBD 38/46 (82.6) 38/38 (100) None Biliary stricture(n = 3)Pancreaticobiliary malignancy (n= 5)Kawamura et al[48], 2013 Retrospective comparative 65 CBD stone (n =49)F (n = 56) N/A 61/65 (93.8) 51/61 (83.6) Bowel perforation (n =2, 3.1%)Pancreaticobiliary malignancy (n= 26)S (n = 2) Pancreatitis (n= 4, 6.2%)SBE (n = 3)Others (n = 4) Bleeding (n = 1,1.5%)Benign biliary stricture (n = 1)Kim et al[49],2014 Retrospective cohort 30 CBD stone (n =30)S EPLBD±EST 30/30 (100) 30/30 (100) Pancreatitis (n= 2, 6.7%)Bleeding (n = 2,6.7%)Iwai et al[50],2014 Retrospective comparative 19 N/A SBE N/A 18/19 (95) 18/18 (100) None Cheng et al[51],2015 Retrospective cohort 77 CBD stone (n =77)DBE EPLBD/EPBD±NK 73/77 (95) 67/73 (92) Bowel perforation (n =3, 3.8%)
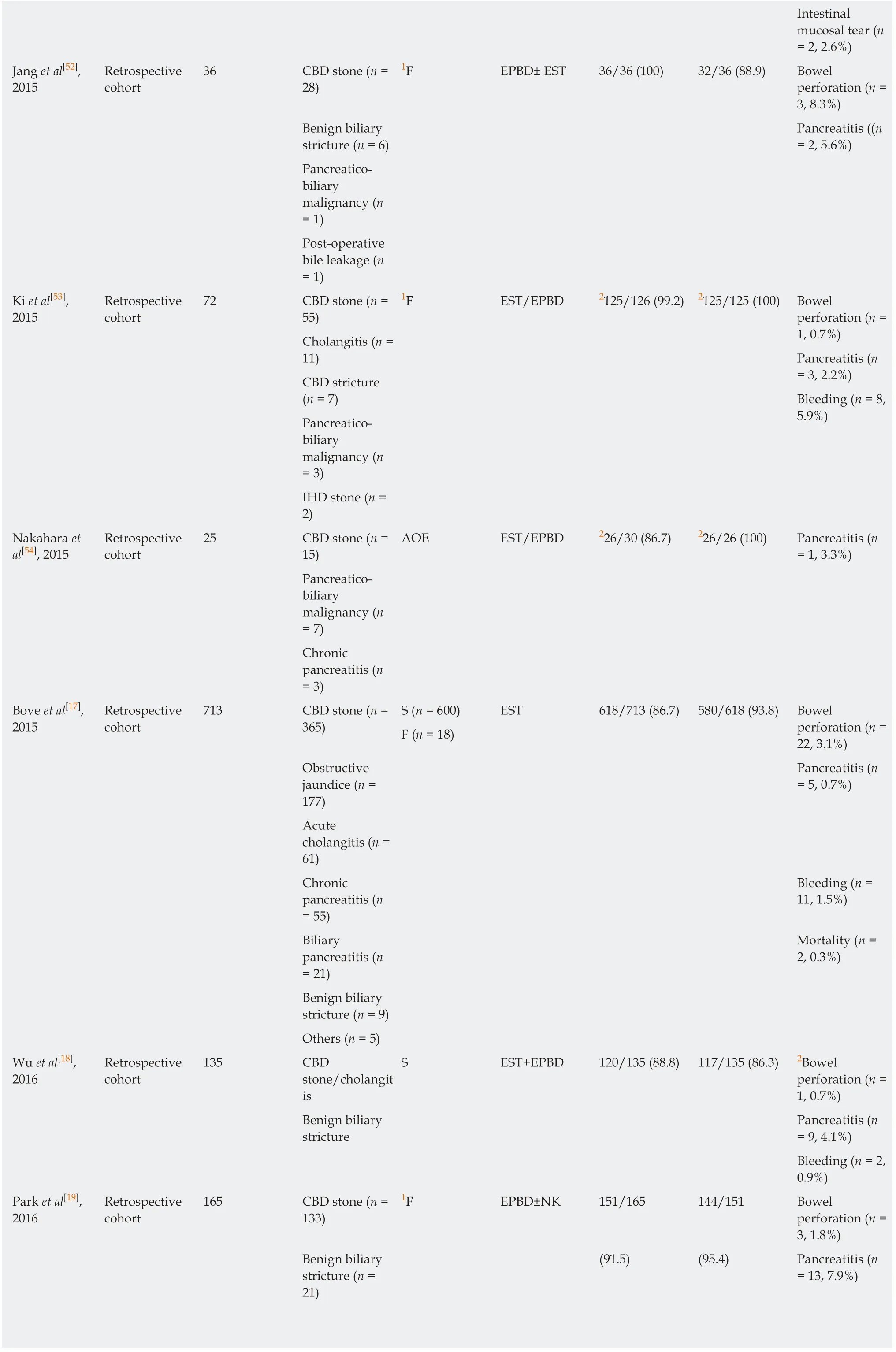
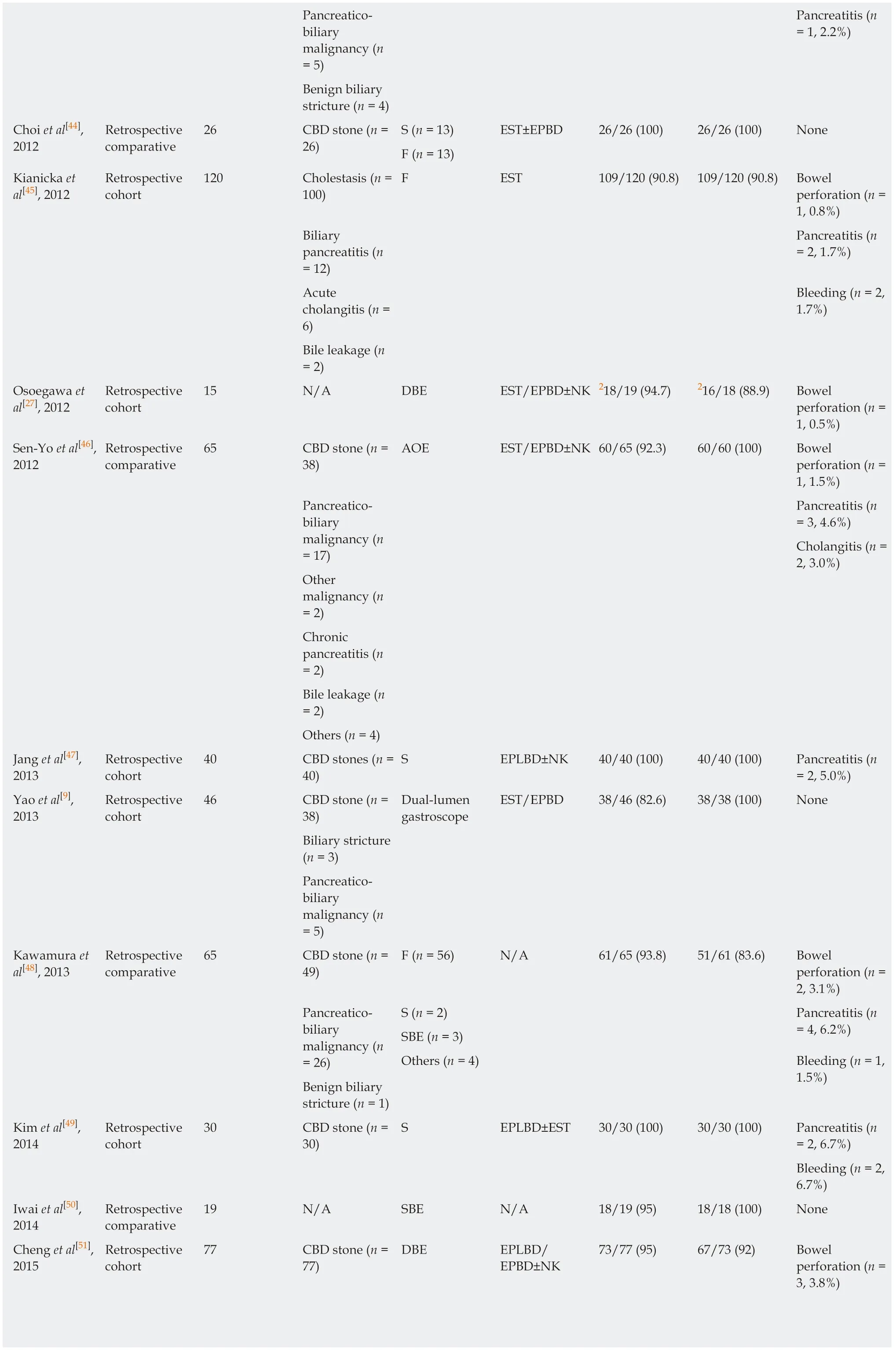
Intestinal mucosal tear (n= 2, 2.6%)Jang et al[52],2015 Retrospective cohort 36 CBD stone (n =28)1F EPBD± EST 36/36 (100) 32/36 (88.9) Bowel perforation (n =3, 8.3%)Benign biliary stricture (n = 6)Pancreatitis ((n= 2, 5.6%)Pancreaticobiliary malignancy (n= 1)Post-operative bile leakage (n= 1)Ki et al[53],2015 Retrospective cohort 72 CBD stone (n =55)1F EST/EPBD 2125/126 (99.2) 2125/125 (100) Bowel perforation (n =1, 0.7%)Cholangitis (n =11)CBD stricture(n = 7)Pancreaticobiliary malignancy (n= 3)IHD stone (n =2)Pancreatitis (n= 3, 2.2%)Bleeding (n = 8,5.9%)Nakahara et al[54], 2015 Retrospective cohort 25 CBD stone (n =15)AOE EST/EPBD 226/30 (86.7) 226/26 (100) Pancreatitis (n= 1, 3.3%)Pancreaticobiliary malignancy (n= 7)Chronic pancreatitis (n= 3)Bove et al[17],2015 Retrospective cohort 713 CBD stone (n =365)S (n = 600) EST 618/713 (86.7) 580/618 (93.8) Bowel perforation (n =22, 3.1%)F (n = 18)Obstructive jaundice (n =177)Pancreatitis (n= 5, 0.7%)Acute cholangitis (n =61)Chronic pancreatitis (n= 55)Bleeding (n =11, 1.5%)Biliary pancreatitis (n= 21)Mortality (n =2, 0.3%)Benign biliary stricture (n = 9)Others (n = 5)Wu et al[18],2016 Retrospective cohort 135 CBD stone/cholangit is S EST+EPBD 120/135 (88.8) 117/135 (86.3) 2Bowel perforation (n =1, 0.7%)Benign biliary stricture Pancreatitis (n= 9, 4.1%)Bleeding (n = 2,0.9%)Park et al[19],2016 Retrospective cohort 165 CBD stone (n =133)1F EPBD±NK 151/165 144/151 Bowel perforation (n =3, 1.8%)Benign biliary stricture (n =21)(91.5) (95.4) Pancreatitis (n= 13, 7.9%)
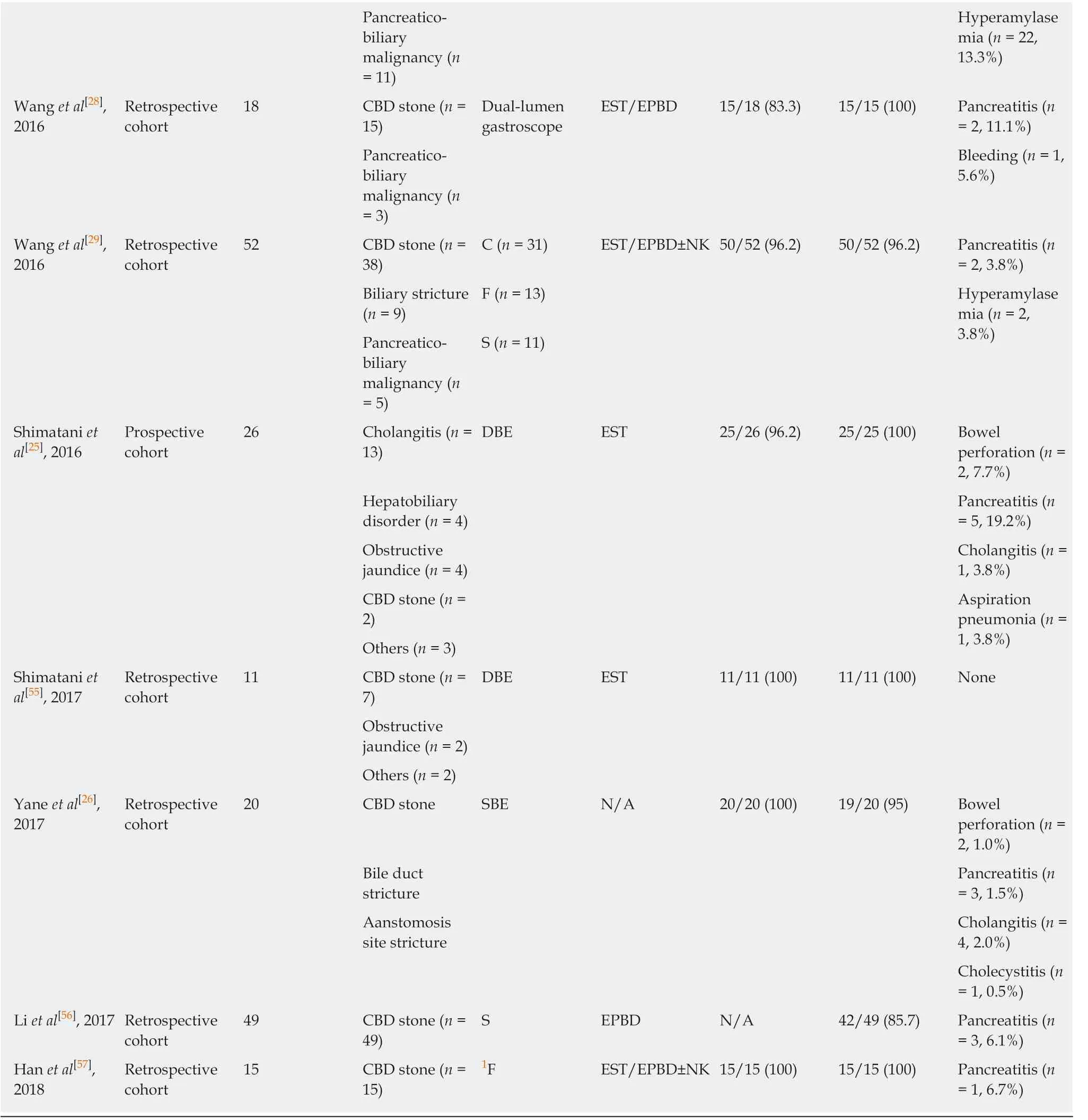
1Cap-fitted forward-viewing endoscope;2The data are per procedure, not per patient. A-loop: Afferent loop; ERCP: Endoscopic retrograde cholangiopancreatography; N/A: Not available; RUQ:Right upper quadrant; EST: Endoscopic sphincterotomy; NK: Needle knife; EPBD: Endoscopic papillary balloon dilation; EPLBD: Endoscopic papillary large balloon dilation; CBD: Common bile duct; IHD: Intrahepatic duct; F: Forward-viewing endoscope; S: Side-viewing endoscope; C: Colonoscope; SBE:Single-balloon enteroscope; DBE: Double-balloon enteroscope; AOE: Anterior oblique-viewing endoscope.
As an introduction to balloon-assisted endoscopy, the double-balloon enteroscope or single-balloon enteroscope have been increasingly used to perform ERCP in surgically altered anatomy, including Billroth II gastrectomy[5,6]. The success rates of ERCP in Billroth II gastrectomy cases by balloon-assisted enteroscopy have been reported from 95.0% to 100%, and seem to be comparable with those of conventional side-viewing endoscopy or forward-viewing endoscopy[25,26]. Balloon-assisted enteroscope has significant benefit to overcome the sharp curve of the anastomosis site and advance much deeper into the small intestine than conventional side-viewing endoscope or forward-viewing endoscope[5,27]. However, ERCP by balloon-assisted enteroscopy is technically demanding and requires expertise and specialized equipments. Balloon-assisted enteroscope is also forward-viewing instrument, which has disadvantages of difficulty in obtaining an en face view of the papilla. Therefore, a head to head comparison of outcomes between different types of endoscopy with a randomized controlled trial (RCT) is needed in the future.
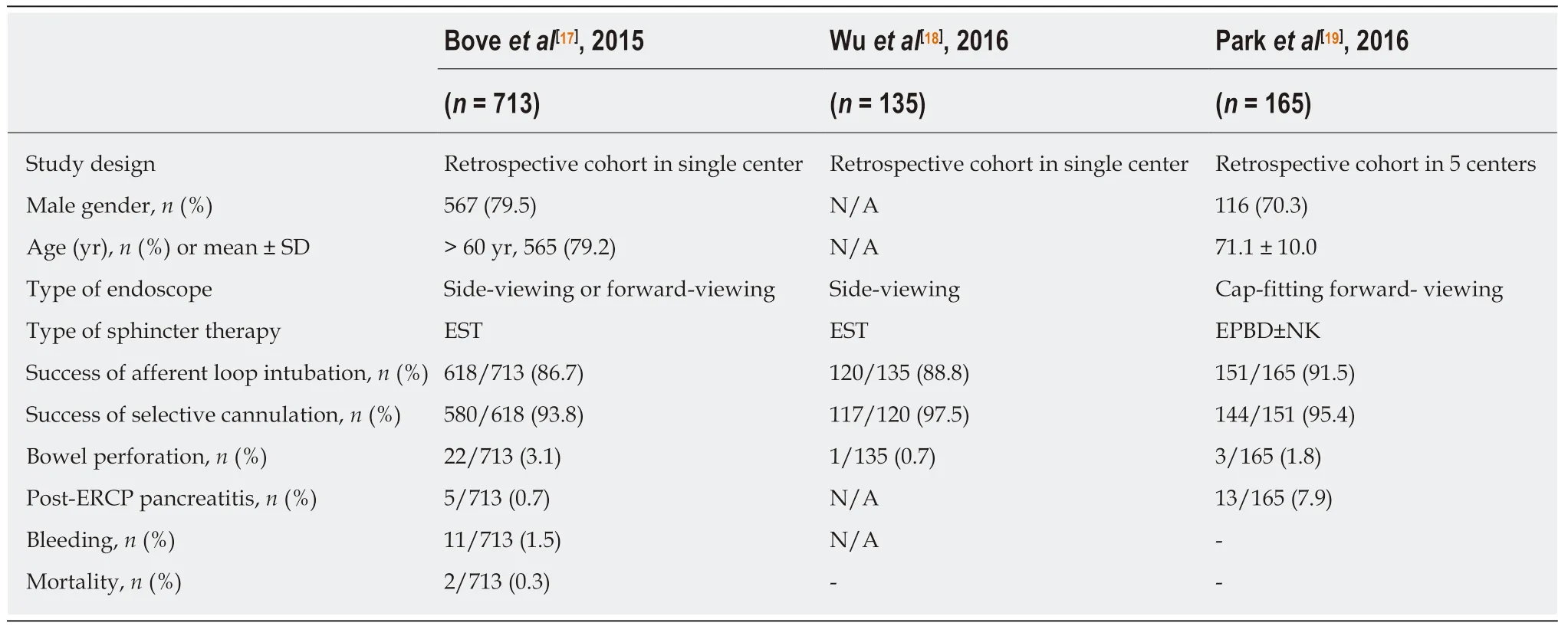
Table 2 Detailed characteristics of the most recently published studies with more than 100 patients
Recently, the advent of new types of endoscopes, such as a dual lumen or multiple bending endoscope, has allowed successful afferent loop intubation and selective cannulation[10,28]. The use of dual lumen endoscope has potential advantage that the cooperation of two instruments through different channels can facilitate papillary cannulation in cases with difficult anatomy such as periampullary diverticulum and surgical altered anatomy. Unfortunately, the success rate of these procedures is not significantly higher than that of conventional side-viewing endoscopy, easily available forward-viewing endoscopy or standard colonoscopy (dual lumen endoscope, 82.8%; multiple bending endoscope, 92.9% vs conventional side-viewing endoscopy, 93.8%-97.5%; forward-viewing endoscopy, 95.4%; standard colonoscopy,96.2%)[9,10,17-19,28,29]. Until now, there has been no large-scale retrospective cohort study or prospective comparative study. Therefore, the new types of endoscopes are practically and economically limited for widespread use.
Another issue, the choice of sphincter therapy, has also been a matter of debate regarding ERCP with Billroth II gastrectomy patients. Traditionally, the performance of sphincterotomy in Billroth II cases is difficult due to its revere position of the biliary and pancreatic duct. The difficulty of sphincterotomy in optimal direction is associated with the risk of bowel perforation or bleeding. So, there have been continued considerable efforts to perform effective and safe sphincter therapy.Dedicated sphincterotomes for Billroth II anatomy such as inverted sphincterotome or S-shaped sphincterotome have been developed and widely used. Recently, the use of EPBD for sphincter management in Billroth II patients has been on the increase. EPBD is particularly useful in ERCP with a forward-viewing endoscope since sphincterotomy may be difficult with this scope which does not have an elevator.Furthermore, in cases with large CBD stones, application of EPLBD can help to efficiently remove these stones in Billroth II gastrectomy cases[12,30]. Therefore, the increasing use of balloon dilator has been the general trend in sphincter therapy in recent years.
This study has potential limitations that should be discussed. First, in this study, it is not sufficiently and clearly described a recent trend toward a better outcome with novel technologies in ERCP in Billroth II gastrectomy patients. Because most of studies regarding novel technologies were case report, case series, and animal study,they were excluded from current systematic review. This point is major limitation of current study. Second, the studies included in the current systematic review were retrospective, observatory publications from more than 30 years with heterogenous indications for ERCP. The performance bias of ERCP according to the endoscopist's experience and technique and operative consideration, including the duration and type of Billroth II operation (antecolic or retrocolic, anisoperitacltic or isoperistaltic),were not described. The older studies can lead to bias because there are the difference of the technological advance such as endoscopic instruments and skill, overall knowledge and experience of endoscopists in performing ERCP of Billroth II gastrectomy patients between the past and the present.
In summary, conventional side-viewing endoscopy remains the most commonly used type of endoscopy for ERCP in Billroth II gastrectomy cases. Forward-viewing endoscopy has been increasingly used to perform ERCP in Billroth II gastrectomy cases because of its advantages, including easy availability and good visual field, as well as the additional advantage of the transparent cap being fitted to the distal end of the endoscope. In recent years, new types of endoscopy, including balloon-assisted enteroscopy, anterior oblique-viewing endoscopy, dual-lumen endoscopy, and multiple bending endoscopy, have been introduced and performed with ERCP safely and effectively. There have also been various types of sphincter therapy applied,including EST, EPBD, and EPLBD, with or without precutting by NK, and the use of diverse types of accessories. As considerable efforts of worldwide investigators have been applied for safe and effective ERCP in this population, the success rate of the procedure and occurrence of adverse events have been improving. In addition, a RCT is required to evaluate the optimal type of endoscopy and sphincter therapy for ERCP in Billroth II gastrectomy patients in the future.
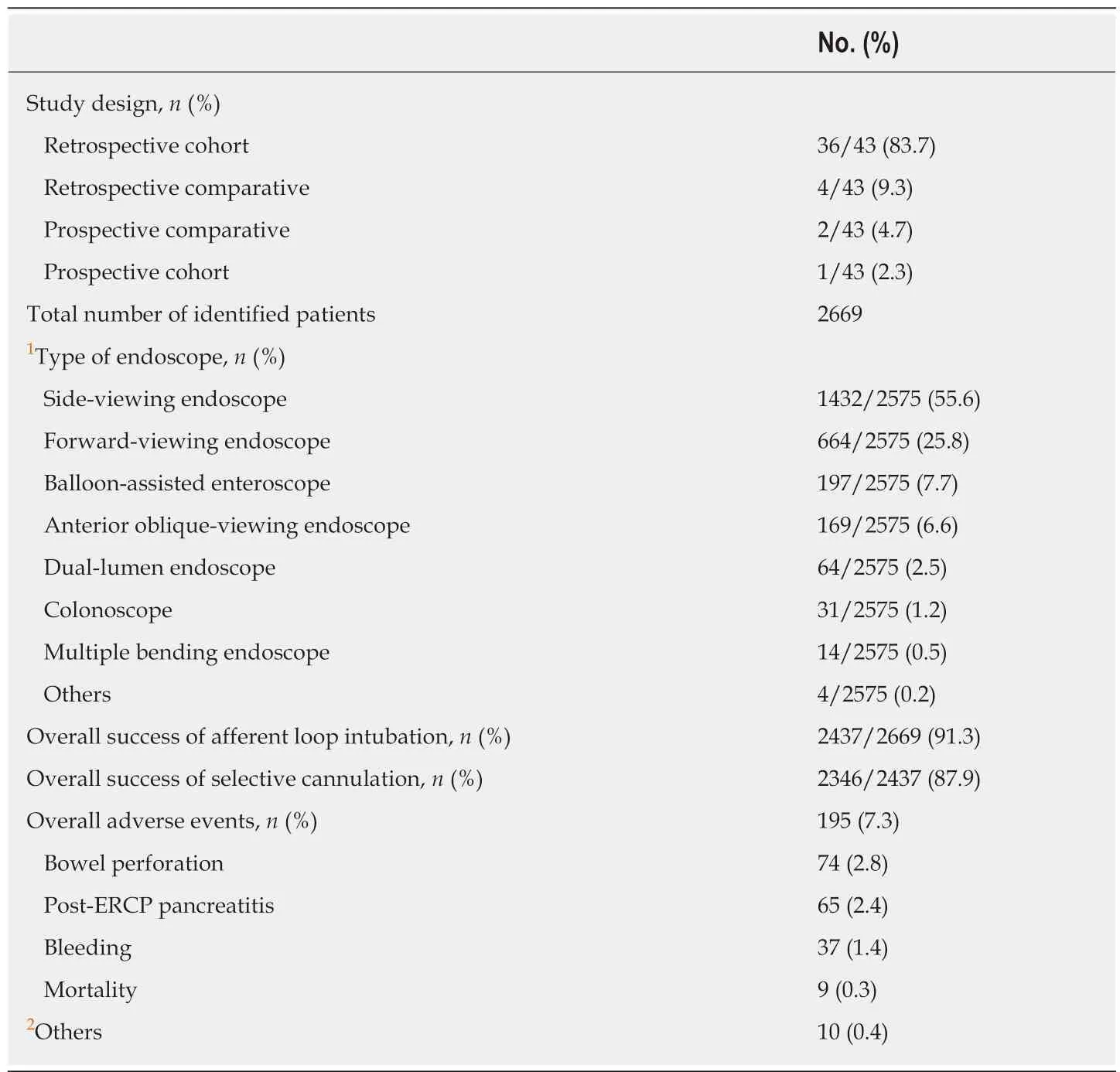
Table 3 Results of the systematic review
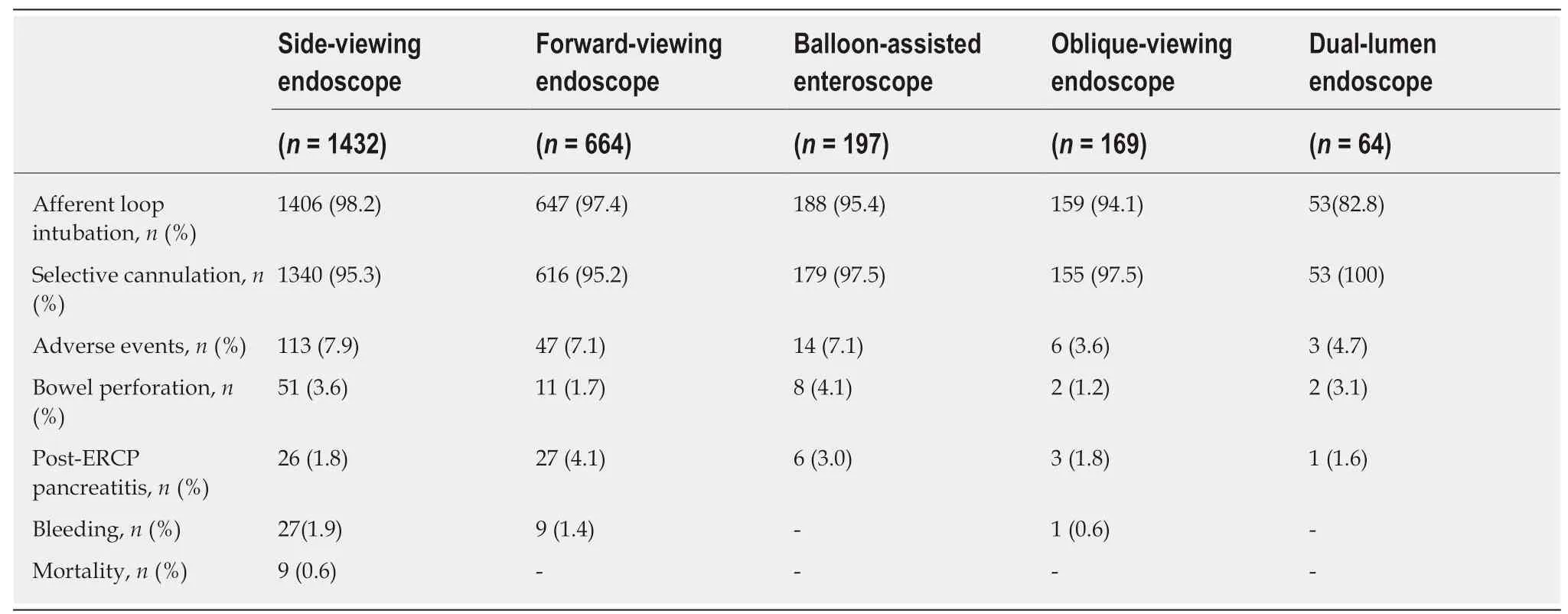
Table 4 Subgroup analysis according to the type of endoscope
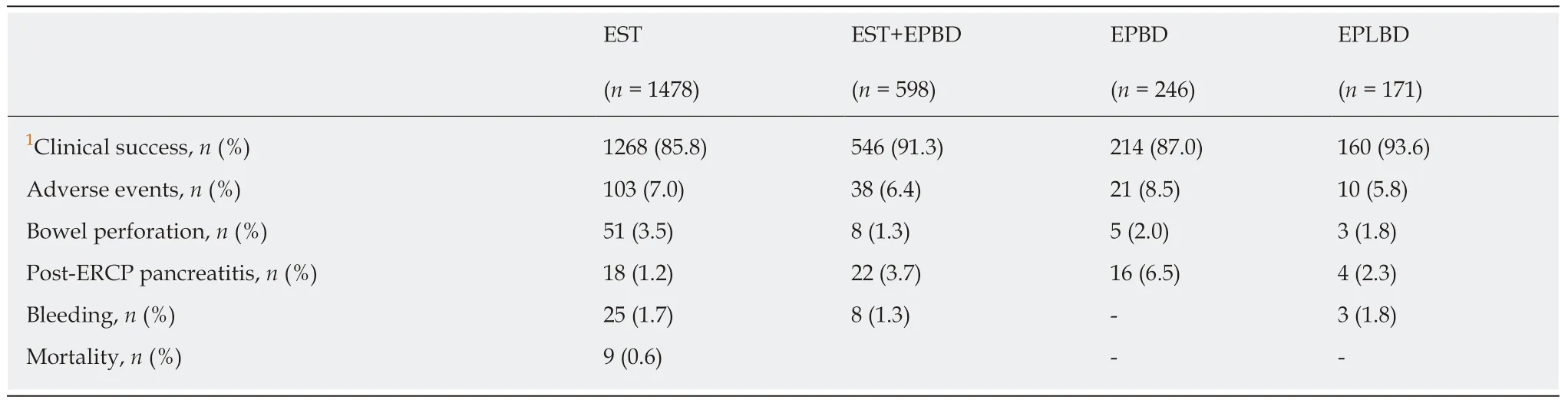
Table 5 Subgroup analysis according to the sphincter management methods
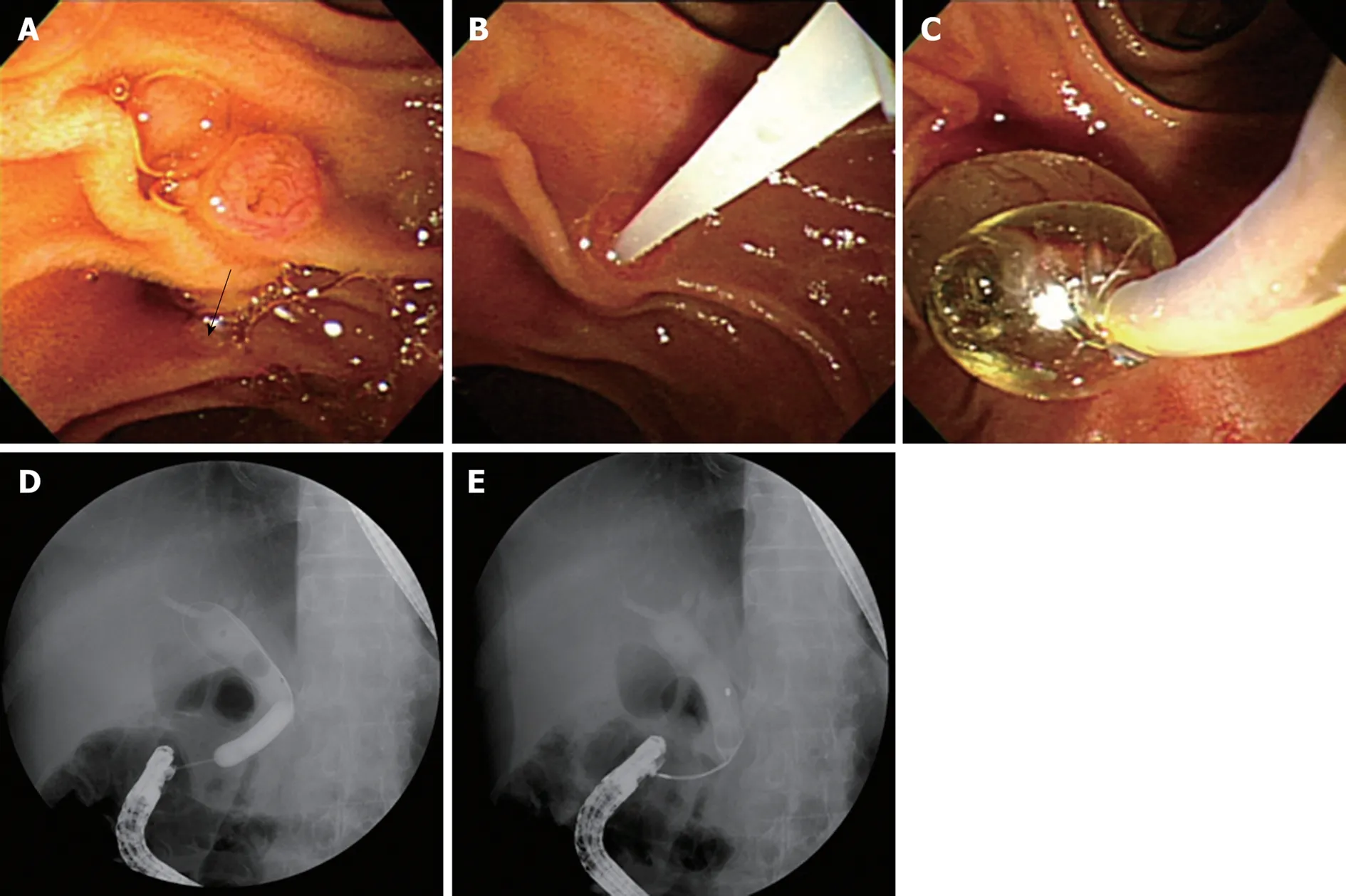
Figure 2 Side-viewing endoscopy. A: Naïve papilla; En face view can be obtained with ease. The direction of bile duct is reversed (arrow); B: Selective cannulation can be achieved with assistance of elevator; C: Sphincter management with papillary balloon dilation; endoscopic view; D: Sphincter management with papillary balloon dilation; fluoroscopic view; E: Common bile duct stone was removed by basket.
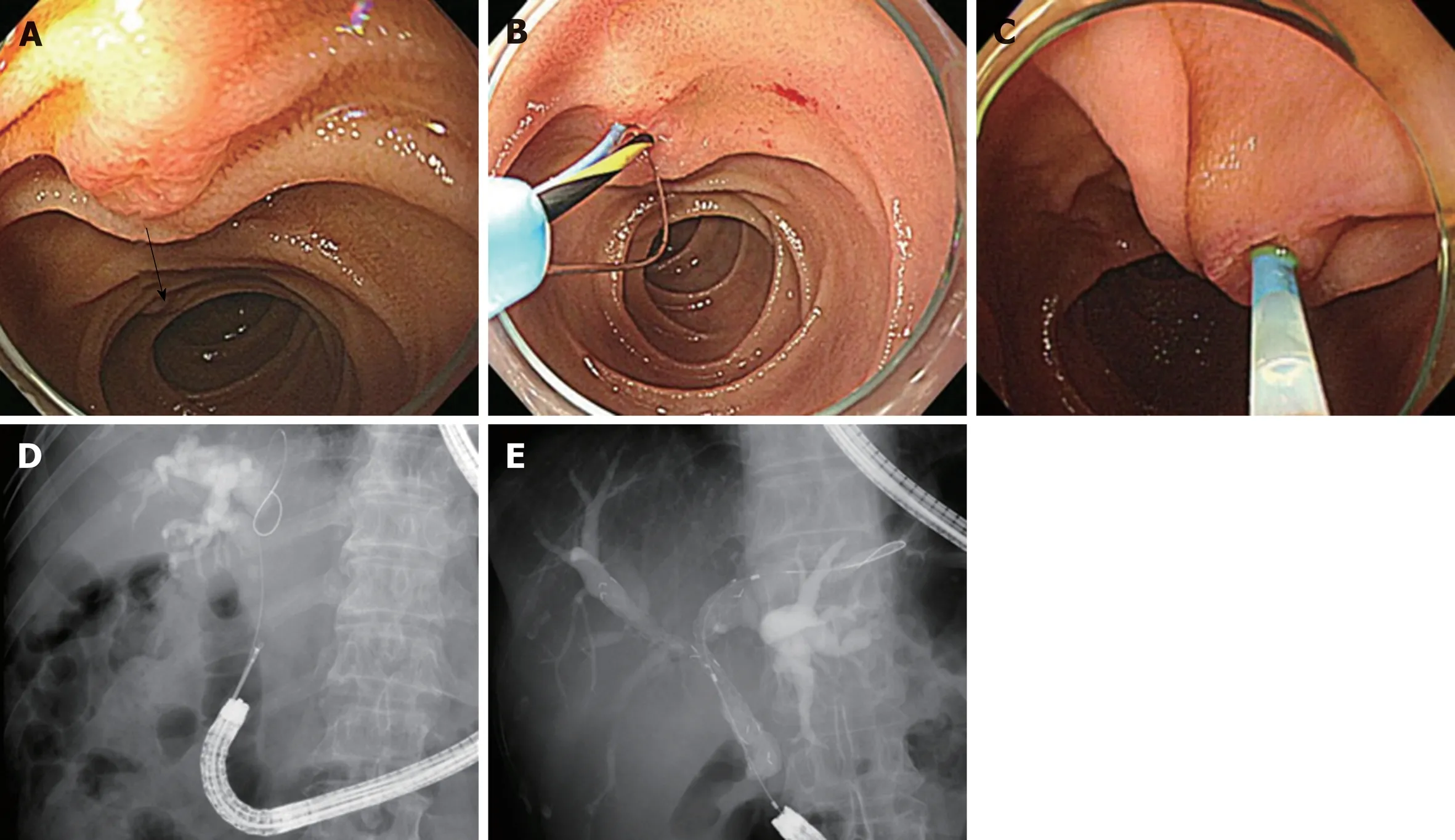
Figure 3 Cap-fitting forward-viewing endoscopy. A: Naïve papilla; It is difficult to obtain en face view. The direction of bile duct is reversed (arrow); B: Gastroscope of 7 o'clock position working channel; Sphincter management with inverted sphincterotome; C: Pediatric colonoscope of 5 o'clock position working channel; D:Endobiliary biopsy was performed in distal common bile duct stricture; E: Bilateral uncovered metal stents were inserted in the malignant hilar stricture.
ARTICLE HIGHLIGHTS
Research background
Endoscopic retrograde cholangiopancreatography (ERCP) in patients who have a Billroth II gastrectomy has been considered a difficult procedure due to the surgically altered anatomy. The difficulties of ERCP in patients with Billroth II gastrectomy include the intubation of the afferent loop, visualization of the papilla, selective cannulation of the bile duct, and optimal sphincter management due to the reverse direction of the papilla. To perform safe and effective ERCP in Billroth II gastrectomy cases, considerable efforts have been put in several ways including the choice of endoscope and sphincter management. However, there has been a paucity of
Research motivation
At present, comparative studies on the efficacy and safety of ERCP in Billroth II gastrectomy cases are lacking because of practical and ethical limitations due to procedure-related morbidity and mortality. This systematic and comprehensive review was performed to obtain a recent perspective on ERCP in Billroth II gastrectomy patients.
Research objectives
The main objective of the study was to assess the efficacy and safety of ERCP in Billroth II gastrectomy patients. In detail, the assessment of success rate of afferent loop intubation and selective cannulation, and rate of adverse events including bowel perforation, post-ERCP pancreatitis, bleeding, cardiopulmonary events, and mortality was performed. In addition, the assessment of these outcomes according to each type of endoscopy and sphincter management methods was performed.
Research methods
A systematic review was performed on the literatures that evaluated the outcomes of ERCP in Billroth II gastrectomy patients. Electronic databases were searched, including PubMed,EMBASE, and Cochrane Library. The outcomes of afferent loop intubation and selective cannulation, and occurrence of adverse events were assessed.
Research results
A total of 43 studies involving 2669 patients were included. The overall success rate of afferent loop intubation was 91.3% (2437/2669), and the overall success rate of selective cannulation was 87.9% (2346/2437). A total of 195 cases (7.3%) of adverse events occurred. Bowel perforations occurred in 74 cases (2.8%), post-ERCP pancreatitis in 65 cases (2.4%), bleeding in 37 cases (1.4%),mortality in 9 cases (0.3%).
Research conclusions
This systematic review showed that the performance of ERCP in the Billroth II gastrectomy patients has been improving with choice of endoscope and sphincter management. To determine the optimal method to perform safe and effective ERCP in Billroth II gastrectomy patients, more comparative studies are needed in the future.
Research perspectives
The success of ERCP in Billroth II gastrectomy has been improving with technical advance.Future research is needed to explore the optimal approach in performance of ERCP in Billroth II gastrectomy cases.
杂志排行
World Journal of Gastroenterology的其它文章
- Immunotherapy for hepatocelluiar carcinoma:Current and futrure
- Application of Big Data analysis in gastrointestinal research
- Biomarkers and subtypes of deranged lipid mettabolism in non-alcohlic fatty liver disease
- Imaging biomarkers for the treatment of esophageal cancer
- Development and in vitro study of a bi=specific magnetic resonance imaging molecular probe for hepatocellular carcinoma
- Effect of NLRC5 on activation and reversion of hepatic stellate cells by regulating the nuclear factor-κB signaling pathway