Evaluation of clinical outcomes in an interdisciplinary abdominal pain clinic: A retrospective, exploratory review
2019-07-10AmandaDeacyCraigFriesenVincentStaggsJenniferSchurman
Amanda D Deacy, Craig A Friesen, Vincent S Staggs, Jennifer V Schurman
Abstract BACKGROUND Pediatric functional gastrointestinal disorders (FGIDs) are common and wellaccepted to be etiologically complex in terms of the contribution of biological,psychological, and social factors to symptom presentations. Nonetheless, despite its documented benefits, interdisciplinary treatment, designed to address all of these factors, for pediatric FGIDs remains rare. The current study hypothesized that the majority of pediatric patients seen in an interdisciplinary abdominal pain clinic (APC) would demonstrate clinical resolution of symptoms during the study period and that specific psychosocial variables would be significantly predictive of GI symptom improvement.AIM To evaluate outcomes with interdisciplinary treatment in pediatric patients with pain-related FGIDs and identify patient characteristics that predicted clinical outcomes.METHODS Participants were 392 children, ages 8-18 [M = 13.8; standard deviation (SD) =2.7], seen between August 1, 2013 and June 15, 2016 in an interdisciplinary APC housed within the Division of Gastroenterology in a medium-sized Midwestern children's hospital. To be eligible, patients had to be 8 years of age or older and have had abdominal pain for ≥ 8 wk at the time of initial evaluation. Medical and Commercial (CC BY-NC 4.0)license, which permits others to distribute, remix, adapt, build upon this work non-commercially,and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See:http://creativecommons.org/licen ses/by-nc/4.0/Manuscript source: Unsolicited manuscript Received: March 30, 2019 Peer-review started: April 1, 2019 First decision: May 9, 2019 Revised: May 21, 2019 Accepted: May 31, 2019 Article in press: June 2, 2019 Published online: June 28, 2019 P-Reviewer: Kakisaka Y, Shen J S-Editor: Yan JP L-Editor: A E-Editor: Zhang YL psychosocial data collected as part of standard of care were retrospectively reviewed and analyzed in the context of the observational study. Logistic regression was used to model odds of reporting vs never reporting improvement,as well as to differentiate rapid from slower improvers.RESULTS Nearly 70% of patients followed during the study period achieved resolution on at least one of the employed outcome indices. Among those who achieved resolution during follow up, 43% to 49% did so by the first follow up (i.e., within roughly 2 mo after initial evaluation and initiation of interdisciplinary treatment).Patient age, sleep, ease of relaxation, and depression all significantly predicted the likelihood of resolution. More specifically, the odds of clinical resolution were 14% to 16% lower per additional year of patient age (P < 0.001 to P = 0.016). The odds of resolution were 28% to 42% lower per 1-standard deviation (SD) increase on a pediatric sleep measure (P = 0.006 to P < 0.040). Additionally, odds of clinical resolution were 58% lower per 1-SD increase on parent-reported measure of depression (P = 0.006), and doubled in cases where parents agreed that their children found it easy to relax (P = 0.045). Furthermore, sleep predicted the rapidity of clinical resolution; that is, the odds of achieving resolution by the first follow up visit were 47% to 60% lower per 1-SD increase on the pediatric sleep measure (P = 0.002).CONCLUSION Outcomes for youth with FGIDs may be significantly improved by paying specific attention to sleep, ensuring adequate skills for relaxation, and screening of and referral for treatment of comorbid depression.
Key words: Pediatric functional gastrointestinal disorders; Integrated care; Behavioral health consultation; Treatment outcomes; Abdominal pain clinic
INTRODUCTION
Abdominal pain associated with pediatric functional gastrointestinal disorders(FGIDs) often interferes with daily activities[1], increases risk for psychological comorbidity[2,3], and decreases quality of life[4]. It is well accepted that FGIDs are multiply-determined; that is, there is no single and specific cause for the conditions.Instead, a host of biological, psychological and social contributors interact in complicated and varying ways to produce symptoms[5]. Historically, treatment for pediatric FGIDs has been conducted in a step-wise fashion, with referral for psychological work up and intervention occurring after the medical evaluation has been “negative” and/or medical treatment has been unsuccessful[6]. This approach has the potential to fragment care, and perhaps worse, follow through on referral for psychological services is known to be poor[7].
One alternative to this model is the delivery of co-located medical and psychological care in the context of an interdisciplinary treatment team[8]. While the benefits of integrated care have been increasingly well documented in the pediatric health arena[9], interdisciplinary treatment remains the exception, rather than the standard, in the care of pediatric FGID patients. In this study, we sought to add to the small, but growing literature on the efficacy of interdisciplinary treatment for pediatric FGIDs in an outpatient tertiary care setting. We evaluated clinical resolution as measured by change in pain and its associated interference, as well as healthrelated quality of life. Further, we sought to identify patient characteristics that served as predictors of clinical resolution. We hypothesized that the majority of pediatric patients seen in an interdisciplinary abdominal pain clinic (APC) would demonstrate clinical resolution of symptoms during the study period and that specific psychosocial variables would be significantly predictive of GI symptom improvement.
MATERIALS AND METHODS
Participants
Participants were 392 children, ages 8-18 (M = 13.8; SD = 2.7), seen for initial evaluation (IE) between August 1, 2013 and June 15, 2016 in an interdisciplinary APC(Table 1).
Study design
Data collected as part of the APC standard of care were retrospectively reviewed and analyzed for the purposes of this investigation, a process approved by the institutional review board. Fifty-three patients (13.7%) were seen for an IE only. This group of patients was generally similar to those who returned for clinic follow up(Table 2). Two statistically significant differences, however, did arise. Patients who attended at least one follow up visit reported at IE that they were less likely to sacrifice important life goals or values in the service of managing pain [Activity Engagement on the Chronic Pain Acceptance Questionnaire-Adolescent, CPAQ-A; t =2.46 (380), P = 0.014] than those who attended the IE only. Additionally, females,compared to males, were disproportionately represented among the patients who attended at least one clinic follow up [χ2 (1) = 5.26, P < 0.022]. All subsequent reported analyses include only patients who attended at least one follow up visit. The number of follow up visits ranged from 1-15 [median = 3; interquartile range (IQR) 2-6]. The median time between the IE and first follow up was 1.7 mo (IQR 1.4-2.2, range 0.5-22.8); the median time between IE and second follow up was 4.2 mo (IQR 3.2-5.7,range 1.3-33.1).
Procedure
The APC is an interdisciplinary clinic housed within the Division of Gastroenterology in a medium-sized Midwestern children's hospital in the United States. Patients eligible for care in the APC must be 8 years of age or older and have had abdominal pain for ≥ 8 wk. The APC is staffed by two pediatric gastro-enterologists, two advanced practice nurses (APNs), a social worker, two licensed psychologists, one certified biofeedback clinician, and four full-time nurses. A pediatric gastroenterologist and a psychologist jointly conduct the IEs, with both professionals reviewing pre-visit questionnaires and medical history, participating in the development of a treatment plan, and overseeing the in-person clinic visit. Follow up appointments are typically staffed by an APN and a psychologist. For a more in-depth description of the clinic model and typical treatments, see Schurman and Friesen[10].
As part of standard care in the APC, patients and their caregivers complete a battery of assessment measures. An abbreviated battery is collected at all subsequent follow ups, which are scheduled naturalistically as dictated by clinical need. For patients seen during the study period, all clinical information obtained during the IE and subsequent follow up visits was extracted for analyses.
Measures
Primary outcomes: Outcome variables were chosen based on PedIMMPACT consensus recommendations[11], and include aspects of the chronic pain itself, as well as physical, emotional, and role functioning. (1) Pediatric Quality of Life Inventory,Version 4.0[12](PedsQL 4.0) is a 23-item measure of health-related quality of life.Physical, Emotional, Social, and School Functioning domain scores and a Total Score can be calculated. Standard scores range from 0 (worst) to 100 (best), and a score of 76 has been established as a critical clinical cutoff[13]. We defined self-reported resolution as a PedsQL Self-Report Total ≥ 76 and parent-reported resolution as a PedsQL Parent-Report Total score ≥ 76; (2) Global Improvement Score (GRF) is a categorical,composite rating designed to capture change in pain and functioning since last visit.Patients are assigned a score of 1 to 5, where 1 = Worse, 2 = Same, 3 = Better (but not meeting criteria for 4 or 5), 4 = Better (symptoms nearly gone or minimal, no interference), and 5 = Better (symptoms gone, no interference). For the purposes of the current study, scores of 4 and 5 were taken to indicate clinical resolution.
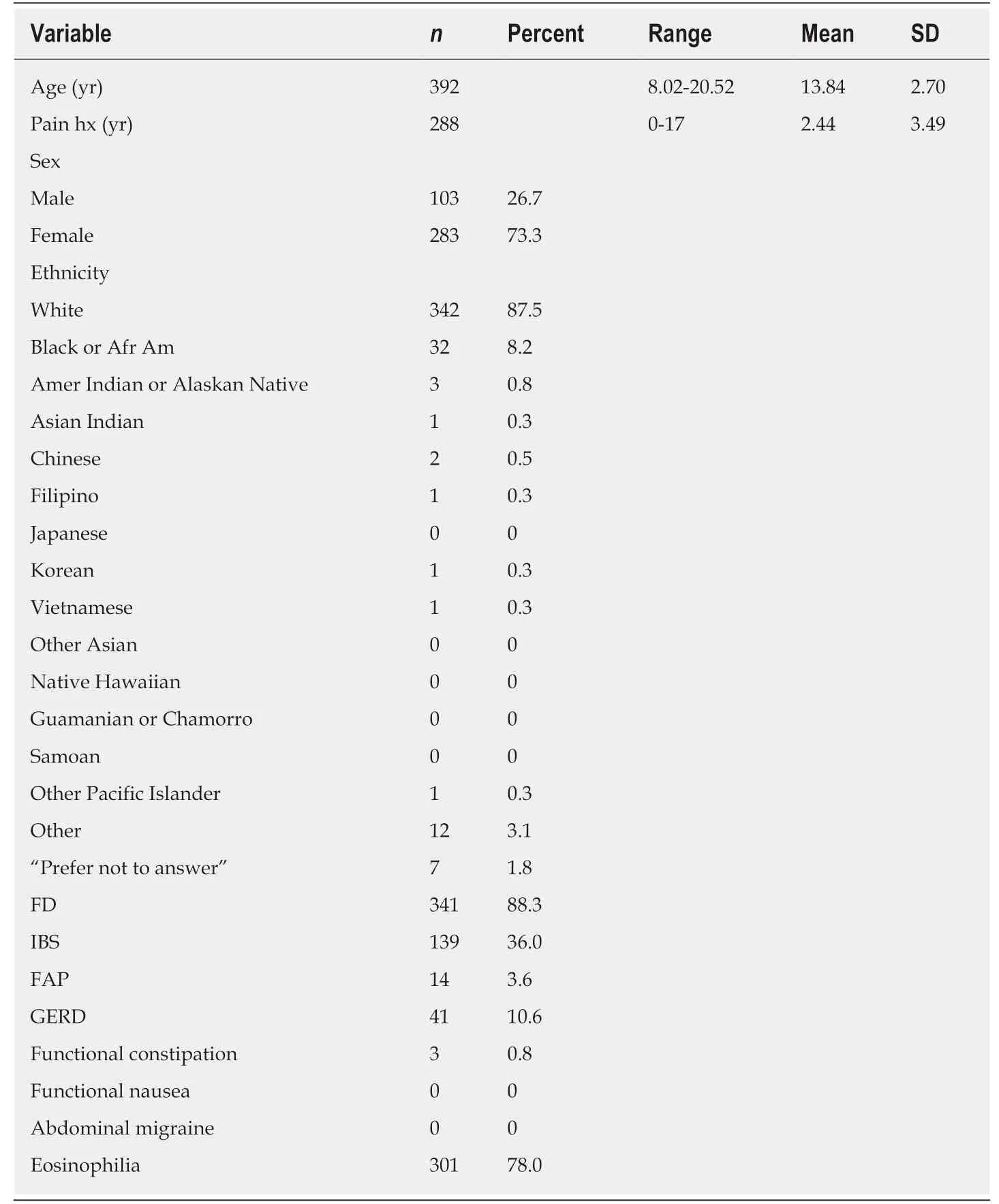
Table 1 Participant characteristics at initial evaluation
Predictors of outcome:Predictor variables considered relevant and meaningful[11]were selected from among those available in our assessment battery. Additionally, we chose two predictors (i.e., presence of eosinophilia and participation in biofeedbackassisted relaxation training between IE and first follow up) unique to the assessment and intervention strategy in the APC.
(1) Patient age; (2) The Behavior Assessment System for Children, Version 3[14](BASC-3) is a measure of parent- and self-reported adaptive and problem behaviors of youth. T-scores in emotional, behavioral, and social domains are produced and identified as in the normal, at-risk, or clinical range; (3) The Sleep Disturbances Scale for Children[15](SDSC) is a 27-item inventory designed to categorize sleep problems in children. The SDSC produces a Total Score and five subscale scores, disorders of initiating and maintaining sleep, sleep breathing disorders, disorders of arousal,sleep-wake transition disorders, disorders of excessive somnolence, and sleep hyperhidrosis; (4) The Illness Behavior Encouragement Scale[16](IBES) is a 12-item measure that assesses the various ways that parents respond to their children's abdominal pain. Higher scores indicate greater engagement in illness-encouraging behaviors; subscale scores for attention and privileges and release from responsibility[17]are calculated; (5) The CPAQ-A[18]is a 20-item measure of adolescents'acceptance of pain, with higher scores indicating greater pain acceptance. The measure produces two subscales, Pain Willingness (i.e., a recognition that attempts to avoid or control pain are often unproductive) and Activity Engagement (i.e., the pursuit of valued activities regardless of pain); (6) Upset/Relax. Participants and their parents responded with True or False to the following: “I (my child) get (gets) upset too easily” and “It is easy for me (my child) to relax”; (7) School attendance. Patients'school experience in the 4 wk prior to a follow up visit were coded as: Full-time, on a modified schedule, or not in school; (8) Biofeedback-assisted relaxation training. We recorded endorsement of biofeedback training in the 4 weeks prior to patients' first follow up visit; (9) Eosinophilia. The presence and location of eosinophilia on endoscopy and colonoscopy were determined by pathology in conjunction with an additional read of biopsies by the physician co-director of the APC (CF).
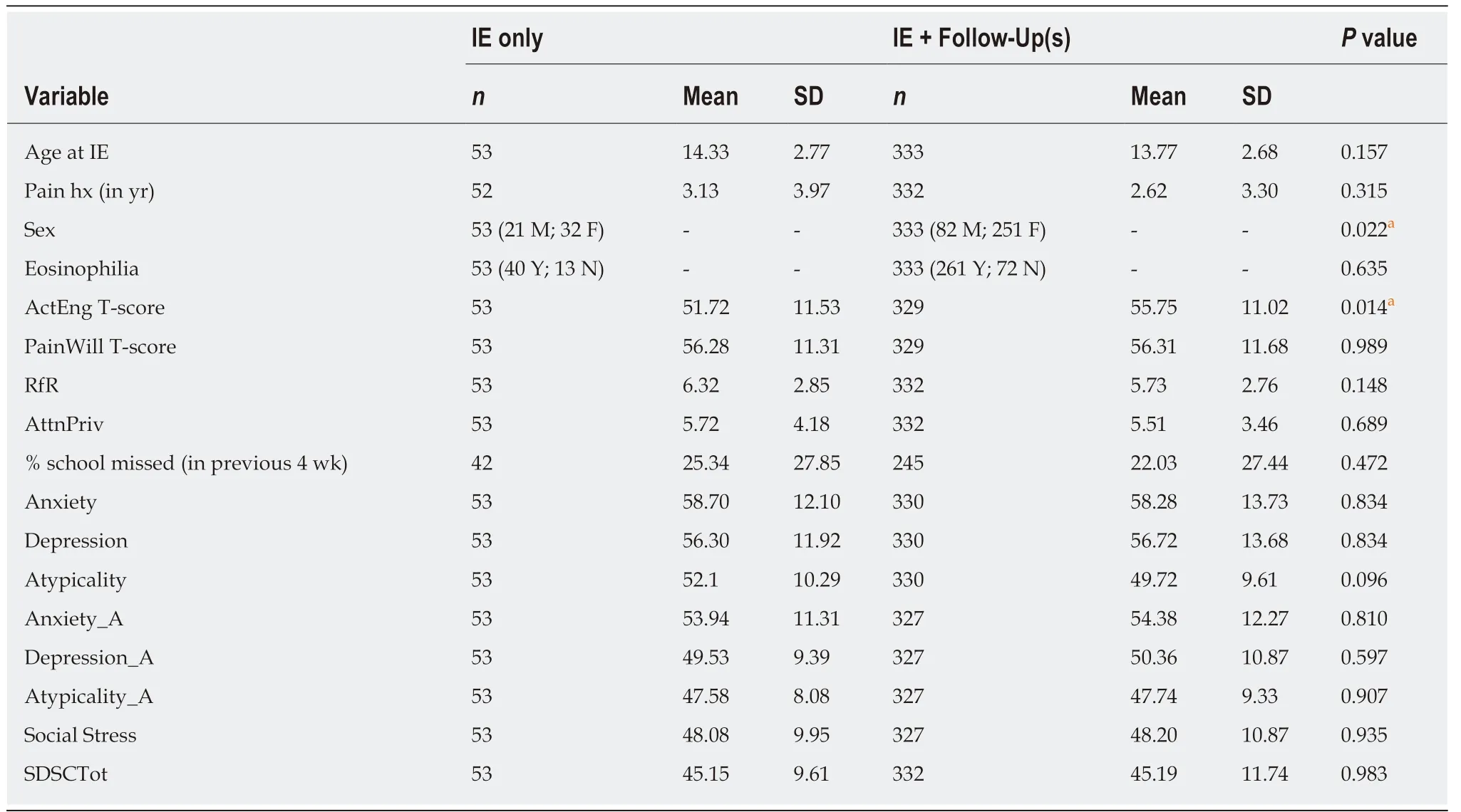
Table 2 Baseline comparison of initial evaluation only vs initial evaluation + follow-up patients
Statistical modeling
Using the LOGISTIC Procedure in SAS 9.4, we modeled odds of achieving, at any follow up visit, clinical resolution as defined by GRF score of 4 or 5 as a function of patient age, total years since onset of pain, school status, parent and patient responses to the Upset/Relax questions, SDSC Total score, CPAQ-A subscale scores, IBES subscale scores, various BASC Self-and Parent-Reported subscales, biofeedback prior to first follow up visit, and presence of eosinophilia. We fit two additional logistic regression models to examine odds of achieving the PedsQL cutoff score at a follow up visit as functions of these same predictors. In these models, the analysis was limited to those not already at or above the cutoff score on the PedsQL measure of interest at IE.
In a series of secondary analyses, we examined predictors of rapid resolution among those achieving resolution according to GRF and self- and parent-reported PedsQL criteria. In these, we defined resolution as “rapid” if patients achieved resolution by the 1stfollow up appointment and “slow” if it occurred by the 2ndfollow up or anytime thereafter. Given the reduced sample size for these rapid resolution models, we retained only predictors with P < 0.10 from the previous corresponding(Y/N) resolution models in order to limit the number of predictors per case. All analyses were conducted and reviewed by a biomedical statistician (VS).
RESULTS
Overall resolution
On the outcome of GRF, 56% of patients reported resolution (i.e., no pain or pain that was nearly gone to minimal with no associated interference) during follow up.Twenty-eight percent reported resolution by the first follow up visit, another 13% by the second follow up visit, and an additional 15% thereafter. Excluding those patients already at or above the clinical cutoff at their IE, 48% of patients, per parents, achieved or exceeded the PedsQL clinical cut off Total score during follow up. Twenty-one percent reported resolution by the first follow up visit, another 15% by the second follow up visit, and an additional 12% thereafter. On the self-report PedsQL, 40% of patients achieved or exceeded the clinical cutoff overall; 17% reported resolution by the first follow up, another 10% by the second follow up, and an additional 13%thereafter.
Predictors of resolution
Results from the following logistic regression models are summarized in Tables 3-5.Patient age was a significant predictor of resolution on all outcome variables. The odds of resolution according to GRF [odds ratio (OR) = 0.81 (0.73, 0.90), P < 0.001] and reaching the parent-reported PedsQL cutoff [OR = 0.85 (0.74, 0.96), P = 0.014] and selfreported PedsQL cutoff [OR = 0.86 (0.75, 0.97), P = 0.016] were 14% to 19% lower per additional year of age. Sleep also was a significant predictor of resolution. The odds of resolution per the GRF [OR = 0.72 (0.53, 0.98), P < 0.040] and reaching the parentreported PedsQL criterion [OR = 0.58 (0.39, 0.85), P = 0.006] were 28% and 42% lower,respectively, per 1-SD increase in the SDSC Total Score. Parent-reported mental health/behavioral concerns were, likewise, predictive of patients achieving resolution. Specifically, the odds of achieving resolution on the self-reported PedsQL variable were 58% lower per 1-SD increase in parent-reported Depression [OR = 0.42(0.22, 0.76), P = 0.006]. Additionally, parents who agreed, “It is easy for my child to relax,” had twice the odds [OR = 2.00 (1.02, 3.96), P = 0.045] of reporting resolution at follow up according to the parent-reported PedsQL. The odds of achieving resolution according to GRF also were predicted by patients' self-reported Pain Willingness [OR= 0.62 (0.46, 0.82), P = 0.001]; surprisingly, the odds of resolution were 38% lower per 1-SD increase in Pain Willingness on the CPAQ-A. Also unexpected, the odds of reaching the parent-reported PedsQL criterion [OR = 2.80 (1.26, 6.43), P = 0.013] and self-reported PedsQL criterion [OR = 2.46 (1.09, 5.75), P = 0.033] were well over twice as high for those patients whose parents agreed, “My child gets upset too easily”.
Predictors of “Rapid” vs “Slow” resolution
Sleep, again, was determined to be a significant pr edictor of rapidity of clinical resolution among those achieving resolution. The odds of achieving resolution according to GRF [OR = 0.53 (0.35, 0.78), P = 0.002] or reaching the parent-reported QL cutoff [OR = 0.40 (0.22, 0.69), P = 0.002] by the first visit were 47% to 60% lower per 1-SD increase in SDSC Total Score.
DISCUSSION
Nearly 70% of patients followed during the study period achieved resolution on at least one of the employed outcome indices. Among those who achieved resolution during follow up, 43% to 49% did so by the first follow up (i.e., within roughly 2 mo after IE and initiation of interdisciplinary treatment). In general, younger patient age,fewer sleep problems, minimal depression, and reported ease of relaxing at the time of IE significantly predicted patients' clinical resolution. Likewise, better sleep predicted patients' propensity to improve quickly.
Overall, our results are consistent with previous findings. Depression in children with pain-related FGIDs is known to be associated with increased severity of abdominal pain and disability[19-21]. Furthermore, evidence suggests that children with both chronic abdominal pain and depression are at risk for continuation of their pain as well as psychiatric disorders in adulthood[22,23]. These findings, taken together with our own, provide support to the notion that down mood complicates clinical recovery from GI symptoms and improvement in quality of life in the short-term and, quite likely, in the long-term. Likewise, sleep has been routinely identified as an important factor in pain outcomes for children and adolescents. Specific evidence suggests that:(1) Children and adolescents with pain are likely to experience sleep disturbance; (2)poor sleep in youth with chronic pain is predictive of more pain as well as of impairments in functioning, including quality of life; and (3) intervention with sleep improves pain outcomes and vice versa[24]. Our data uniquely extend the current literature by suggesting that, not only do fewer sleep problems predict clinical resolution and quality of life overall, they predict patients' tendency to report improvement quickly. Recent data also indicate that symptoms of anxiety and depression mediate these pain-sleep relationships[25]. Third, pediatric patients with FGIDs often are referred to one of several ancillary services with the most, albeit still limited, empirical support-cognitive-behavioral therapy hypnotherapy, and biofeedback[26,27]with the goal of alleviating physical symptoms, via general stress management and coping skills training. As such, it is reasonable that children who inherently possess these skills for relaxation and general coping at the outset of treatment for their FGID are more likely to experience clinical resolution of their symptoms.
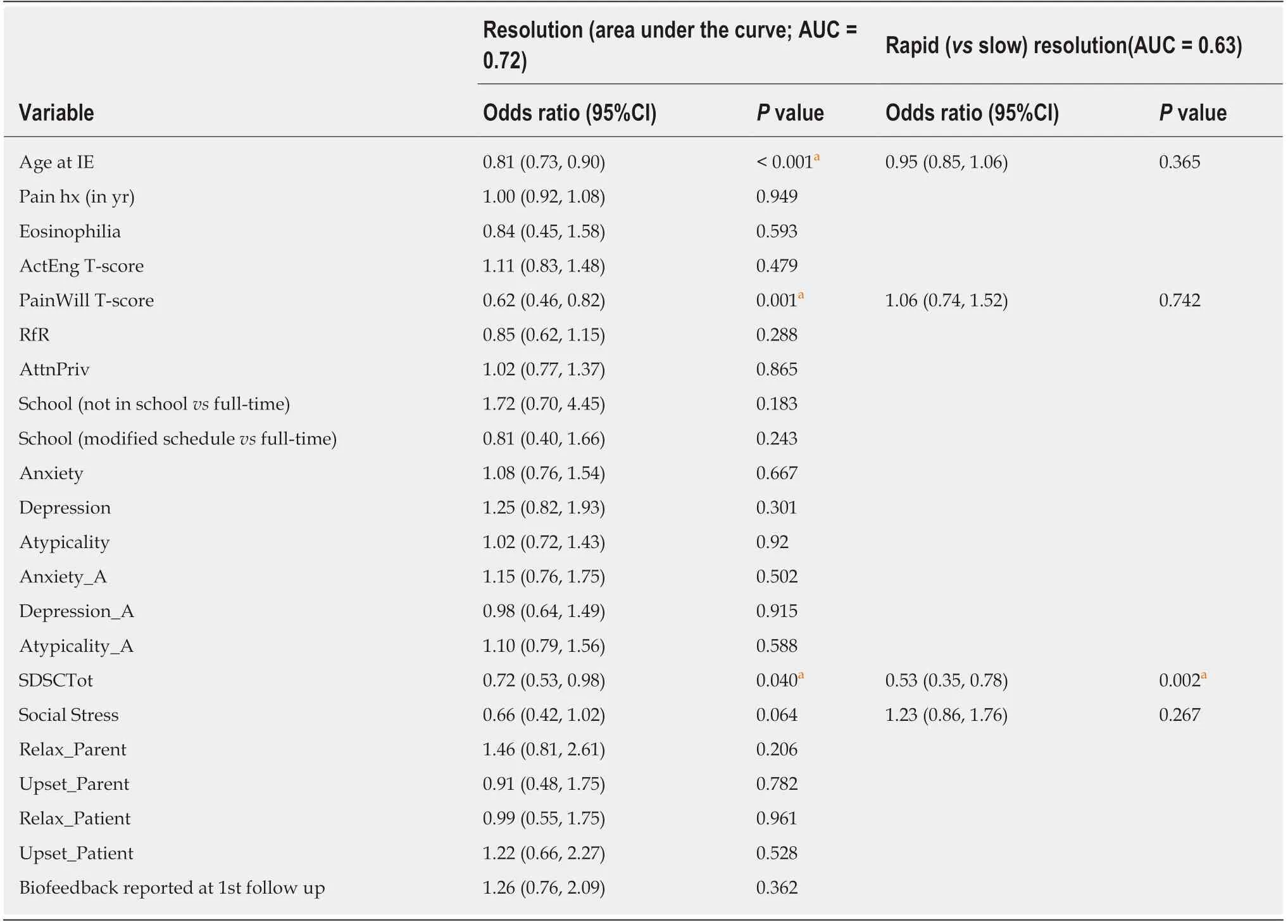
Table 3 Logistic regression results for clinical resolution and rapid clinical resolution on global improvement score
Contrary to our expectation, higher levels Pain Willingness reported at IE did not predict resolution during the follow up period according to our outcome, GRF.Similar to passive coping strategies, an exclusive focus on elimination of pain as the top priority - that is, an (un) “willingness” to experience pain and regular attempts to avoid or control it - is associated with more depression, anxiety, and functional disability in children and adolescents with chronic pain[18]. As such, we anticipated that patients with greater pain willingness at the outset would be more, rather than less, likely to achieve resolution. McCracken et al. also reported, however, that while greater acceptance of pain (which includes pain willingness) was associated with less distress and disability, it was not correlated with lower pain intensity. It is possible and even expected, then, that because resolution according to GRF required positive changes in both pain and disability or functioning, higher pain willingness may not universally predict improvement on this variable.
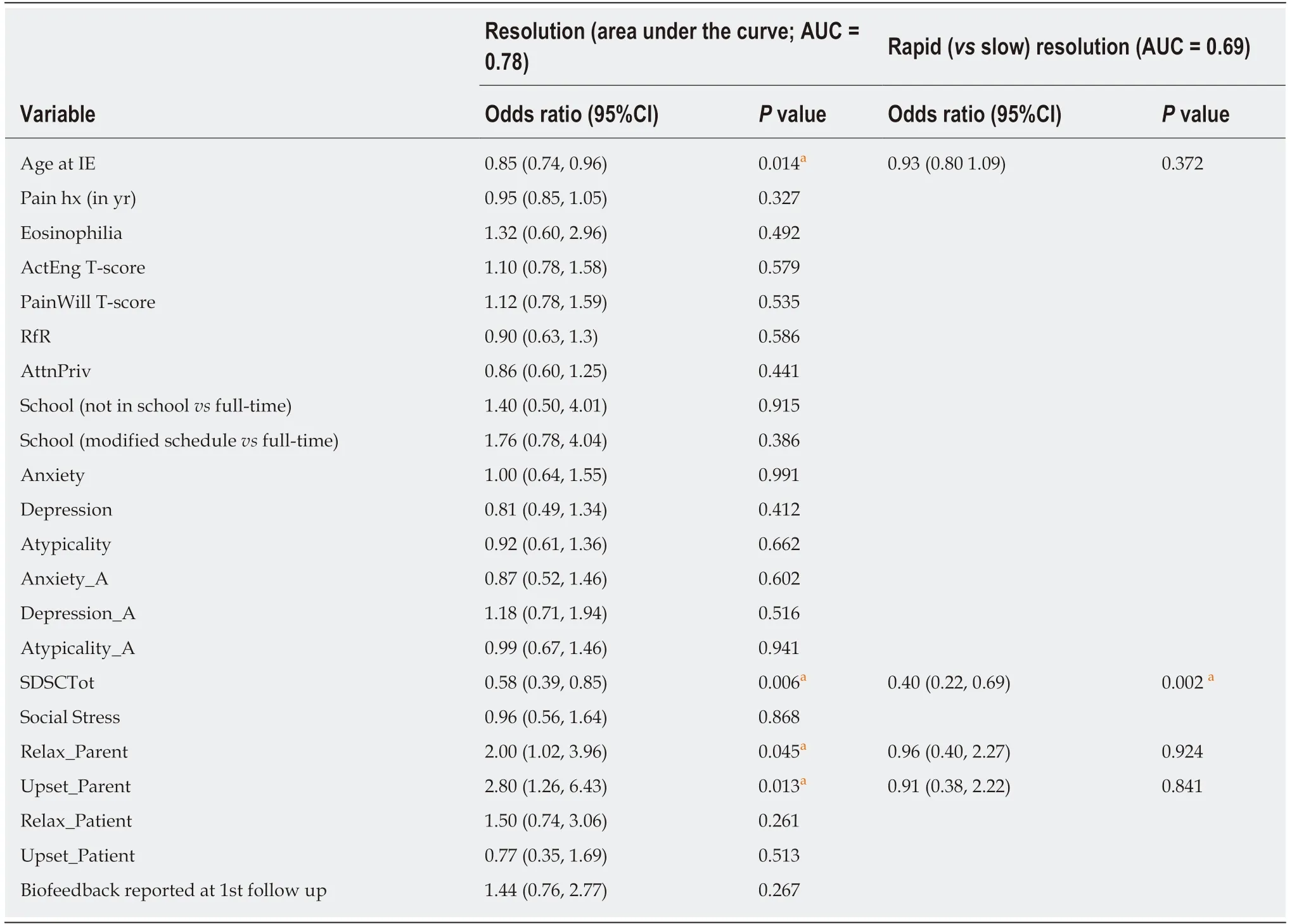
Table 4 Logistic regression results for parent-reported pediatric quality of life inventory resolution (score ≥ 76) and rapid resolution
What the above data suggest is the unequivocal necessity of medical and psychosocial screening, along with combined medical and behavioral intervention,from the outset for pediatric patients with FGIDs. In the APC, we provide broad psychosocial screening as part of the medical history taking and include focused intervention during both IE and follow up visits on sleep hygiene and general stress management. Additionally, we provide targeted behavioral health coaching on topics such as coping, behavioral activation, parenting, medication adherence, and obtaining school support, as well as make recommendations for psychological and psychiatric intervention outside the setting of the APC. This manner of practice is in stark contrast to the typical step-wise intervention (i.e., medical followed by psychological assessment and intervention) that characterizes the bulk of gastroenterology practice at present[6].
The current study possesses a number of strengths. The results presented are the product of naturalistic data collection as part of standard of care in an interdisciplinary specialty clinic. Collecting data in this way allows for early identification of patient factors that can complicate the treatment course of pediatric FGIDs, thereby allowing for proactive intervention. Based on our findings, this is likely to include:intensive targeting of older children and teens to bolster their clinical outcomes (and mitigate the impact of their older age on their tendency to less readily experience clinical resolution), consistent attention paid to sleep quality and quantity during clinic visits, offering of training in specific relaxation training methods, and repeated screening and referral for pediatric and adolescent depression. Second, data collection at each and every visit allows provider teams to be clinically nimble and adapt to changes in patients' presentations more quickly than would be possible without this information. Finally, repeated data collection at naturalistic time points during provides ample statistical power for modeling complex clinical questions whose answers reflect the real-world waxing and waning of symptoms and associated circumstances, thereby decreasing the chance of missing naturally occurring symptomatic variability.
These strengths notwithstanding, the study possesses limitations worth mention.To start, the retrospective, uncontrolled nature of the study design does not allow casual inferences to be made about the specific impact of our interdisciplinary,standard of care intervention. Second, given the number of predictors included (and,thus, hypotheses reported) in our analyses, statistical significance should be interpreted with caution. We report p-values not as arbiters of clinical importance, but as aids in identifying effects that are unlikely to be attributable solely to chance.Finally, and perhaps most important, because data were collected naturalistically and not at predetermined time points, the interpretation of “missing” data becomes complicated. In the event that patients do not attend scheduled follow up visits because they are well, “missing” data may, in fact, signal improvement that is unreported or undetected. We also employed a strict definition of resolution on the GRF, requiring that symptoms, even if improved, were causing no impairment in patients' functioning. Thus, even if patients identified themselves as better, but continued to experience even mild impairment in their functioning due to abdominal pain (i.e., GRF = 3), our analyses classified these as instances of non-resolution. As such, we argue that our results are likely to be rather conservative estimates of our patients' improvement, though additional data would be needed to confirm this claim.
ACKNOWLEDGEMENTS
The authors would like to thank the dedicated APC nursing staff and our patients and their families for their contribution to this work.
ARTICLE HIGHLIGHTS
Research background
Abdominal pain characteristic of pediatric functional gastrointestinal disorders (FGIDs) is known to be associated with a high degree of psychosocial comorbidity and to persist into adulthood without intervention. Likewise, it is well accepted that a host of biological,psychological, and social factors contribute and interact in complicated and varying ways to produce the various FGID phenotypes. Historically, treatment for pediatric FGIDs has been conducted such that, following a “negative” medical evaluation and/or unsuccessful medical treatment, referrals to mental health providers are made and relevant treatments undertaken.One alternative to this model is the delivery of co-located medical and psychological care in the context of an interdisciplinary treatment team. Although the benefits of integrated care are well documented in pediatrics, interdisciplinary care remains the exception, rather than the standard,in the care of pediatric FGID patients. The current study aims to address this current gap in the existing literature.
Research motivation
In an effort to measure and improve upon clinical change in both medical and psychosocial outcomes in pediatrics FGIDs, we employed naturalistic data collection as part of standard of care in an interdisciplinary specialty clinic. In so doing, we collected a rich and diverse data set that allowed us to evaluate patients' clinical resolution, as well as identify factors that complicate symptom improvement. This is significant in that it adds to the small, existing literature on the efficacy of interdisciplinary treatment for pediatric FGIDs in an outpatient tertiary care setting.Furthermore, identification of psychosocial factors that delay or prevent symptom improvement sets the stage for early, proactive intervention.
Research objectives
The primary research objectives included: evaluation of outcomes with interdisciplinary treatment in pediatric patients with pain-related FGIDs, and identification of patient characteristics that predicted clinical outcomes.
Research methods
Study participants were 392 children, ages 8-18 (M = 13.8; SD = 2.7), seen between August 1, 2013 and June 15, 2016 in an interdisciplinary APC housed within the Gastroenterology Division of a medium-sized children's hospital in the United States. To be eligible for the study, patients had to be 8 years of age or older and have had abdominal pain for ≥ 8 wk at the time of initial evaluation. Medical and psychosocial data collected naturalistically as part of standard of care were retrospectively reviewed and analyzed. Logistic regression was used to model odds of reporting vs. never reporting improvement, as well as to differentiate rapid from slower improvers. Collecting data in this way allows for early identification of patient factors that can complicate the treatment course of pediatric FGIDs, thereby allowing for proactive intervention.Second, data collection at each and every visit allows provider teams to be clinically nimble and adapt to changes in patients' presentations more quickly than would be possible without this information. Finally, repeated data collection at naturalistic time points during provides ample statistical power for modeling complex clinical questions whose answers reflect the real-world waxing and waning of symptoms and associated circumstances, thereby decreasing the chance of missing naturally occurring symptomatic variability.
Research results
Nearly 70% of patients followed during the study period achieved clinical resolution on at least one of the employed outcome indices. Among those who achieved resolution during follow up,close to half did so within roughly 2 mo after initial evaluation and initiation of interdisciplinary treatment. Patient age, sleep, ease of relaxation, and depression all significantly predicted the likelihood of resolution, with older age, poor sleep, difficulty relaxing, and the presence of depression predicting worse outcomes. Poor sleep also was found to significantly predict the rapidity of clinical resolution such that it delayed clinical resolution of symptoms beyond the first follow up visit. The identification of the relationships between patient age, sleep, ease of relaxation, and depression and FGID symptom improvement is a critical first step in crafting the most effective biopsychosocial interventions for this complex set of diagnoses.
Research conclusions
As anticipated, a great majority of patients treated in the context of an interdisciplinary model of care for chronic abdominal pain demonstrated improvement. In addition, unique psychosocial characteristics were able to be identified that uniquely predicted the presence and pace of positive outcomes. Based on our findings, clinical outcomes among youth with pediatric FGIDs are likely facilitated by intensive targeting of older children and teens to bolster their clinical outcomes, consistent attention paid to sleep quality and quantity during clinic visits, offering of training in specific relaxation training methods, and repeated screening and referral for pediatric and adolescent depression. Furthermore, these findings highlight the need for continued inquiry into the benefit and necessity of concurrent medical and psychosocial screening and intervention as standard of care for all for children affected by FGIDs.
Research perspectives
Use of naturalistically collected data in the context of an observational study provides rich and unique clinical and research opportunities. Data collected as standard of care in a busy clinic provides opportunities for individualized, in-the-moment intervention with patients as they present, as well as the ability of researchers to identify patterns among groups of patients. In the case of the current study, we were able to identify behavioral factors that, if addressed, have the potential to increase the likelihood of clinical symptom resolution among youth with FGIDs.Future investigations would benefit from the use of controlled research designs wherein researchers compared standard medical care to interdisciplinary care.
杂志排行
World Journal of Gastroenterology的其它文章
- Immunotherapy for hepatocelluiar carcinoma:Current and futrure
- Application of Big Data analysis in gastrointestinal research
- Biomarkers and subtypes of deranged lipid mettabolism in non-alcohlic fatty liver disease
- Imaging biomarkers for the treatment of esophageal cancer
- Development and in vitro study of a bi=specific magnetic resonance imaging molecular probe for hepatocellular carcinoma
- Effect of NLRC5 on activation and reversion of hepatic stellate cells by regulating the nuclear factor-κB signaling pathway