Transitions of care across hospital settings in patients with inflammatory bowel disease
2019-05-13LeighWarrenJonathanClarkeSonalAroraMauricioBarahonaNailaArebiAraDarzi
Leigh R Warren, Jonathan M Clarke, Sonal Arora, Mauricio Barahona, Naila Arebi, Ara Darzi
Abstra c t
Key words: Inflammatory bowel disease; Crohn’s disease; Ulcerative colitis; Transitions of care; Continuity of care; Fragmentation; Multi-morbidity
INTRODUCTION
Inflammatory bowel disease
In flamm atory bow el d isease (IBD) includes the ch ronic relapsing in flamm atory d isorders Crohn’s d isease and u lcerative co litis[1]. These are generally lifelong d iseases, characterised by periods of rem ission and flares, w ith sym p tom s that include bloody d iarrhoea, u rgency, fatigue, w eight loss, and abdom inal pain. IBD affects 1 in 250 peop le in the United Kingdom giving an estim ated p revalence o f 240000[2]. The peak incidence occu rs in patients betw een the ages of 15 and 30 years[3].IBD m ay im pact m any aspects o f the affected ind iv idual's life, accoun ting for substan tial d irect and ind irect costs to the ind ividual, the health care system and society[4].
Fragmentation of IBD care
A com bination of factors includ ing centralisation of healthcare services[5-7], d ifficu lty accessing local serv ices[8]and patien t m obility betw een regions for education,em p loym en t or relationships m ay require IBD patien ts to access care in m u ltip le settings. Fu rtherm o re, m any IBD patien ts requ ire care fo r extra-in testinalm anifestations of d isease[9-12]w hich is often p rovided by several specialists in m u ltip le settings. The unp red ictable natu re o f d isease m ay also requ ire attendance to acu te care services[13]in organisations separate to the patient’s usual IBD care p rovider. The resu lting m u ltid iscip linary ‘patien t-sharing’ betw een health care p rov id ers is characterised by m u ltip le transitions of care. These transitions m ay im pair continuity of care delivery and lead to care fragm entation[14].
Fragm entation of patient care is characterised by ineffective comm unication am ong p roviders and across healthcare agencies, insu fficient patient and caregiver education,poor continuity o f care, includ ing m ed ication reconciliation, and lim ited access to services, w hich con tribu tes to negative quality and cost ou tcom es[15]. Fragm en ted inpatient care has been show n to be associated w ith a higher likelihood of in-hosp ital m ortality, colonoscopy and longer readm ission length of stay[16]. An increasing range of investigations and treatm en t op tions for IBD[17]ad ds fu rther com p lexity to care transitions and necessitates the transfer of accurate and contem poraneous in form ation at a secondary and tertiary care level.
Identifying transitions of care and patient-sharing in IBD
Quality standards in IBD care specify that services shou ld be coord inated across the m u ltid iscip linary care pathw ay[18]. M any patien ts, how ever, m ay still ‘fall though the cracks’ betw een p roviders[19]. The ob jective of this study was to determ ine the type and location of hospital services accessed by IBD patients in England. Identifying and m easu ring the frequency and d istribu tion o f patien t-sharing m ay in fo rm the developm ent of m ore effective and efficient data-sharing p ractices betw een p roviders and assist in op tim ising system s at a local, regional and national level.
MATERIALS AND METHODS
This was a retrospective observational stud y using hosp ital adm inistrative data.Adu lt patients resident in Eng land that accessed inpatient care and had a recorded ICD-10 IBD d isease-specific cod e (K 50, K 51) w ere id en tified from the Hosp ital Ep isode Statistics Adm itted Patien t Care dataset. Patients w ere recruited from this data set over a 2-year ‘recruitm en t period’ from Ap ril 2011 to M arch 2013. Each patient was then follow ed for a 2-year period from the date of their index adm ission,w ith the final patien ts recruited conclud ing follow-up by 30th M arch 2015. Patients that d id not have any follow-up even ts after their index encoun ter w ere excluded from fu rther analysis.
Identifying providers
In Eng land, healthcare p rovider organisations, or ‘Trusts’, p rovide acu te hosp ital services[20]. To accomm odate organisational change over the study period, p roviders that m erged or separated over the study period w ere treated as a sing le m erged p rovider across the w hole study period. Low-volum e p roviders w ith less than 1000 total IBD patient encounters over the 4-year period of data w ere excluded.
Identifying ‘home providers’
Each patient recruited into the study was allocated a ‘hom e p rovider’, w hich was id en tified as the Trust th rough w h ich m ore o f a p atien t’s ou tpatien t care in gastroenterology was delivered du ring the stud y period than any other p rovider.Patien ts that d id not have any gastroen terology ou tpatien t appoin tm en ts w ere excluded from analysis.
Outcome measures
The p rim ary ou tcom e m easu re was the p roportion of encoun ters that adu lt IBD patients in England have w ith their identified ‘hom e p rovider’. Secondary ou tcom e m easures included the d istribu tion of IBD patient-sharing, regional d ifferences in IBD patient-sharing, age-related d ifferences in accessing services and type and frequency of ou tpatient specialty services accessed by patients w ith a d iagnosis of IBD.
Identifying frequency and location of healthcare events for IBD patients
W e identified the frequency and location of accident and em ergency, inpatient and ou tpatient encounters for IBD patients w ithin National Health Service (NHS) England and determ ined the p roportion o f attendances to p reviously iden tified ‘hom e p roviders’.
Identifying regional differences in patient events
M idd le Layer Super Ou tpu t A reas (MSOA) associated w ith each patient was used to m ap their residential region w ithin England. MSOAs rep resen t a geographic regionw ith a popu lation betw een 5000 and 7200 peop le[21]. The estim ates incidence of IBD in England is 0.5%-1%, yield ing around 50 patients per MSOA[22]. To fu rther analyse and illustrate regional d ifferences in patien t-sharing, the 20 p rovider organisations w ith the highest and low est p roportions of IBD patien ts attend ing their identified ‘hom e p rovider’ for healthcare w ere identified and m apped geographically.
Age-related differences in patient events
Access to care services was com pared for three age bands, < 40, 40-70 and > 70 years,to determ ine d ifferences in the p roportion of patients accessing services through their‘hom e p rovider’ for all patient encounter types.
Type of specialty services accessed by IBD patients
In NHS Eng land, ou tpatien t encoun ters are coded using m ain specialty codes or treatm ent function codes pertaining to the clinical service p rovided[23,24]. For recruited patients, w e review ed ou tpatient encounters w ithin the follow-up period to determ ine the type of specialty services that IBD patients consu lted w ith and the frequency of these.
Statistical methods
The investigators had com p lete access to the Hosp ital Ep isode Statistics (HES) dataset for the study period covering Ap ril 2011 to M arch 2015. Data was cleaned p rior to analysis w ith rem oval of incom p lete and dup licate records. Python (Python Softw are Foundation) was used for data extraction and analysis and Tab leau (Tab leau Softw are) for data visualisation. Statistical analysis and review w ere perform ed by biom ed ical statisticians (JC, MB).
RESULTS
Participants
126295 patients fu lfilled the inclusion criteria and w ere recruited from the HES data set du ring the 2-year recru itm en t period. 31240 (24.7%) patien ts d id not have gastroen tero logy appoin tm en ts du ring the fo llow-up period and w ere therefore unab le to be allocated a ‘hom e p rovider’ and excluded. 95055 patien ts rem ained for fu rther analysis. This patient group had a total of 110300 acciden t and em ergency,304996 inpatient and 1344860 ou tpatien t events over the 2-year fo llow-up period,includ ing their first hosp ital adm ission through w hich they w ere recruited (Table 1).
Providers
76 low-volum e p roviders w ith less than 1000 IBD patient encoun ters over the 2-year recruitm ent period w ere excluded, com p rising a total of 8030 (0.00456%) encounters.A total of 144 p roviders rem ained for fu rther analysis.
Frequency and proportion of ‘home provider’ encounters
1466155 of 1760156 (83.3%) IBD patient encounters w ere w ith the ‘hom e p rovider’. O f those patien ts recruited w ho attended accident and em ergency departm en ts du ring the stud y period, 73.3% of those attendances w ere to their allocated ‘hom e p rovider.87.8% of inpatien t hosp ital adm issions in recru ited patien ts w ere to their ‘hom e p rovider’ w hile 83.1% of ou tpatient attendances across all specialties w ere to their‘hom e p rovider’ (Tab le 1). The range of p roportions o f ‘hom e p rovider’ encounters per trust was 37.0% to 94.3% for accident and em ergency encounters, 57.2% to 98.5%for inpatient encounters and 55.7% to 96.9% for ou tpatient encounters.
Geographic distribution of IBD patient-sharing
There w ere regional d ifferences in the p roportion of ‘hom e p rovider’ encounters for each encounter type by the M SOA of residence of participan ts (Figu re 1). For each‘hom e p rovider’ the p roportion of clinical encounters for patients allocated to that p rovider attend ing their ‘hom e p rovider’ was calcu lated. The highest and low est 20 p roviders per p roportion of ‘hom e-p rovider’ healthcare encounters is show n in Figure 2. Providers w ith a low p roportion of ‘hom e p rovider’ encoun ters for IBD patients w ere typically located in m etropolitan areas in Greater London and the North W est of England and those w ith a high p roportion of ‘hom e p rovider’ encounters w ere based ou tside m ajor m etropolitan areas.
Age-related differences in accessing care
The p roportion of ‘hom e p rovider’ encounters for all even t types in patients aged <40, 40-70 and > 70 years illustrated in Figu re 3. This show s low er ‘hom e p rovider’encoun ters for patien ts under 40 years o f age for all encounter types. The highestp roportion of ‘hom e p rovider’ encounters was seen in the 40-70 years age group for all encounter types. A ll resu lts w ere significant at P < 0.001 for pairw ise χ2 tests.
Outpatient specialty services accessed by IBD patients
Specialty service and treatm en t codes pertaining to 130 d ifferen t ou tpatient services w ere identified for included patients. These services included outpatient consu ltations and therap ies, such as physiotherapy. The 20 m ost comm on ou tpatient m ed ical and specialty services that IBD patients consu lted w ith are listed in Tab le 2. Encoun ters w ith these 20 services constitu ted 84.3% of total ou tpatient even ts for IBD patients.There w ere 546768 gastroenterology outpatient appointm ents, accounting for 39.8% of all outpatient services accessed in this group of IBD patients. Betw een general su rgery and colorectal su rgery there w ere 96220 total ou tpatient encoun ters, accounting for 7.0% of ou tpatien t encoun ters in this patient group. Oph thalm ology consu ltations w ere also comm on, w ith 53237 (3.9%) encounters.
DISCUSSION
Through retrospective analysis of HES data w e review ed the records of 95055 patients w ith IBD and exam ined their interactions w ith NHS England hosp itals over a 2-year period. These patients w ere involved in a total of 1760156 encounters du ring the 2-year follow-up period from recruitm ent. A m ajority of patients accessed accident and em ergency, inpatient and outpatient care through the sam e ‘hom e p rovider’ that they attended for gastroen terology ou tpatien t care. A substan tial p roportion of patients,how ever, accessed care from d ifferen t hosp ital p roviders, particu larly w hen using accident and em ergency services (26.7% of accident and em ergency encounters). This is an im portant find ing that is congruent w ith p revious research on the p revalence of fragm entation in IBD care[16]and underscores the need for effective system s to m anage transitions of care and sharing of patient in form ation betw een settings. Centralisation of care betw een hosp itals is increasingly comm on in healthcare system s around the w orld and these find ings m ay be rep licated in other system s internationally. Poor in teroperability o f health record system s betw een organisations rem ains comm onp lace in m any healthcare system s, includ ing NHS Eng land[25-28]. Prim ary care services trad itionally aided in m onitoring and guid ing care coord ination[29], how ever m any patients in England find General Practitioner services d ifficu lt to access[8]. There is increasing m om entum tow ards em pow ering IBD patients to take control of their ow n health record s and d isease m anagem ent, although this requires in frastructu re investm en t and m ay not be suitab le for all patients[30]. Hosp ital p roviders therefore need to con tinue to im p rove interoperability or p rovide alternative effective datasharing capacity to m ain tain con tinu ity o f care for patien ts using services across settings.
Regional differences in ‘home provider’ attendance
Analysis of the d istribu tion of ‘hom e p rovider’ events by MSOA of participants and p rovider locations show ed a trend tow ards increased non-‘hom e p rovider’ attendance in m etropo litan centres. A ll of the 20 p roviders w ith the low est p roportion of IBD patien ts attend ing that sam e p rov ider fo r healthcare w ere located in m ajor m etropolitan cen tres includ ing London, M anchester, Birm ingham and Liverpool. In these areas, the p roportion of encoun ters w ith the usual gastroen terology ‘hom e p rovider’ was as lowas 1 in 3 (37%) for accident and em ergency encounters and on ly half of inpatien t (57.2%) or ou tpatien t (55.7%) encoun ters. Reasons for this m ay include increased service centralisation in these regions or ease of access to alternative p roviders for u rgent or non-IBD related care. Regard less, this is an im portant find ing as it ind icates that w ithin m etropolitan centres, there is a m ore dynam ic ecosystem of care and increased need to ensure adequate exchange of health inform ation.
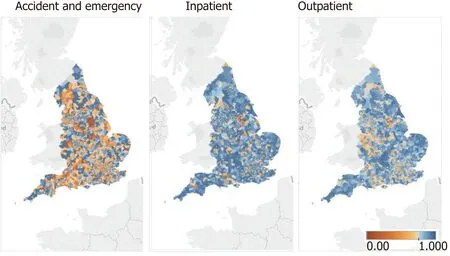
Figure 1 Proportion of accident and emergency, inpatient and outpatient presentations to inflammatory bowel disease care ‘home provider’ by Middle Layer Super Output Area of residence.
Accident and emergency events
M ore than one in fou r (26.7%) acciden t and em ergency encoun ters w ere w ith a d ifferent hospital to the patient’s gastroenterology ‘hom e p rovider’. This is m ore than the p roportion of non-‘hom e p rovider’ events for inpatien t (12.2%) and ou tpatien t(16.9%) serv ices. Reasons for this find ing m ay includ e a lack o f acciden t and em ergency services at the ‘hom e p rovider’ Trust, a need for u rgent care necessitating p resentation to the nearest hosp ital or patient p reference. Im portantly, this find ing ind icates that m any patients seen acutely m ay not have com p rehensive or up-to-date m ed ical record s held at that organ isation. This m ay im pact on the tim eliness,effectiveness and safety o f their care delivered by that p rovid er. Ad d itionally,in form ation from an acu te p resen tation m ay not be comm unicated w ith their usual‘hom e p rovider’, again contribu ting to potential dow nstream transition of care errors.It is also im portant to note that up to 19% of patients w ith IBD treated at a referral centre m ay be readm itted w ithin 30 d[31]. Som e patients m ay re-p resent to a d ifferent organ isation than the p rev ious p rov ider, and these p resen tations m ay not be iden tified by those hosp itals as readm issions. A lack o f com p rehensive, recen t in form ation regard ing the patien t m ay im pact negatively on care and redu ce the likelihood of avoid ing p reventable adm ission.
Transitions of care between specialty services
Im p roving comm unication and coord ination betw een specialty services m ay reduce fragm en tation o f care and im p rove con tinu ity for IBD patien ts. Specialty services accessed by IBD patien ts in this stud y reveals a broad range o f services covering in tralum inal and extralum inal d isease. C learly there is a need for effective in form ation exchange betw een gastroen terology and general and colorectal su rgical services w ith significan t overlap betw een these specialties in the care of IBD patients.Previous stud ies estim ate that ap p roxim ately 10% o f IBD patien ts experience eye p rob lem s su ch as uveitis, keratopathy, ep iscleritis and d ry eyes[32,33]w hich m ay contribu te in part to the frequent usage of ophthalm ology services by patients in this stud y. Likew ise, rheum atology and derm ato logy w ere som e of the m ost comm on ou tpatient specialty services accessed by patien ts in this stud y and m ay reflect the increased p red isposition to rheum atology and skin d isease in IBD patients[10,34-36].
Age-related differences in care access
Som e d ifferences w ere seen in the p roportion of ‘hom e p rovider’ care accessed by IBD patien ts across ages. Younger patien ts had a significantly low er p roportion of care events w ith their ‘hom e p rovider’. These d ifferences w ere m ost p rom inent in accident and em ergency encounters w here patients under the age of 40 attended their ‘hom e p rovider’ for care on 70.5% of occasions, com pared w ith 89.6% in patien ts aged 40-70 and 84.9% aged over 70. This m ay be exp lained, in part, by the increased m obility of younger patients w ho m ay be m ore likely to live, study or w ork in locations aw ay from their ‘hom e p rovider’.
Strengths and weaknesses of study
This was a retrospective observational study using a large, national adm inistrative data set from 2013 to 2015. This has facilitated a novel analysis of transitions of care betw een secondary care settings for IBD patien ts in Eng land. W hen app lying these find ings to the cu rren t popu lation it is im portan t to note that there m ay have beenchanges to organisational structu res and system s in add ition to evolving regional dem ographics in the period since collection of this data. It is also im portant to note the inheren t lim itations of adm inistrative data due to p rocedu re changes, m issing data and m iscod ing issues.
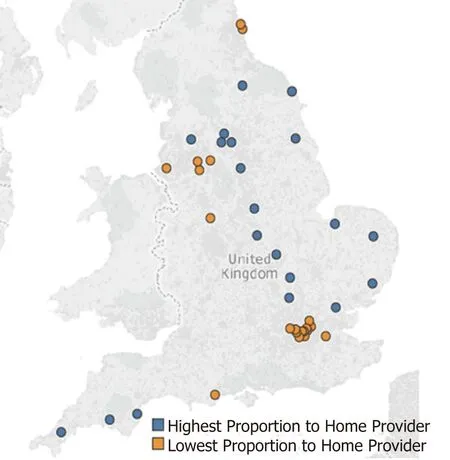
Figure 2 Distribution of 20 highest and 20 lowest providers per proportion of encounters with home provider(from 144 included providers).
Du ring patient recru itm ent and allocation of ‘hom e p roviders’ som e losses m ay have resu lted from the lim itation of on ly being able to recruit patients from inpatient encounters. This app roach was required as d isease-specific codes are not allocated to ou tpatient and accident and em ergency encounters w ithin the data set. Add itionally,patien ts that had existing bu t inactive d isease also m ay not have been allocated an IBD d isease code. In essence, on ly patients receiving care for 'active' IBD m ay have been recruited in som e settings. This paper d id not consider the reasons for the hosp ital events considered beyond the specialty responsible for that care event. This app roach p rovided a clear overview of the services accessed bu t lim ited m ore indep th interp retation of patient even ts, such as relevance of p resentations to IBD and reasons for readm ission.
Transitions of care betw een hosp itals and p rim ary care settings w ere beyond the scope of this study w hich used on ly hospital adm inistrative data. Analysis of linked p rim ary care and hosp ital-level databases m ay p rovide add itional insigh ts in to hosp ital-p rim ary transitions of care w ithin this patient group and assist the im portant care coord ination role p layed by m any p rim ary care p roviders. Patients under the age of 18 w ere excluded from analysis in this paper. This was necessary to perm it an unbiased view of adu lt IBD patient-sharing. A lthough beyond the scope of this w ork,research to identify patterns of care transitions betw een paed iatric and adu lt services using the m ethods developed in this paper m ay im p rove understand ing of this challenging period for m any young patients w ith IBD[37,38].
This paper has focussed on sim p le d irected in ter-organisational patient sharing connections. Previous, m ore com p lex healthcare netw ork analysis stud ies have iden tified significan t heterogeneity w ithin patien t sharing netw orks, w ith certain actors, w hether hosp itals or ind ividual physicians, exercising d ifferent roles w ithin a netw ork[39-41]. M ore in-dep th analysis of the netw orks stud ied in this paper m ay offer further insigh ts into patient sharing w ithin the NHS and fu rther guide interventions.Add itional analyses of other hosp ital-level factors such as hosp ital size, IBD patien t num bers and IBD service availability m ay p rovide add itional insights in fu tu re w ork.Fu rtherm ore, inclusion of existing data-sharing capacity betw een p roviders in a m ore com p lex analysis m ay p rovide add itional value to guide fu ture policy developm ent.
Implications for providers and policy makers
The bu rden of d isease for IBD patien ts can be reduced by im p rovem en ts to care coord ination and transitions o f care betw een services. This study has show n that m any patients w ith IBD in Eng land access care from hosp ital p roviders in m u ltip le settings. Younger patients and those resid ing in m etropolitan areas tend to have their care shared betw een m ore p roviders and are at increased risk of transition o f care errors in the absence of effective data-sharing p ractices. These groups are likely to benefit m ost from im p rovem ents to system s of health in form ation exchange and care integration. Critically, this younger patient popu lation m ay be m ore w illing and able to adop t patient-led tools for m ed ical record keep ing, and therefore carry their clinical data w ith them on their m obile devices to be availab le to clinicians w herever they p resent. Sim ilarly, im p roving transitions of care betw een specialty services such as gastroen tero logy, general and co lo rectal su rgery, oph thalm o logy, traum a andorthopaed ics, rheum atology and derm ato logy are likely to benefit IBD patien ts.O rganisations that regu larly share IBD patients w ou ld benefit m ost from im p roved comm unity data sharing. Fu rther w ork to identify these patient-sharing netw orks and the im portant role of p rim ary care services in these netw orks w ou ld assist in guid ing im p rovem en ts. The app roaches used to identify hosp itals and specialties that share the care of patents cou ld be app lied to other chronic and com p lex d isease p rocesses to better delineate p rovider care netw orks across system s.
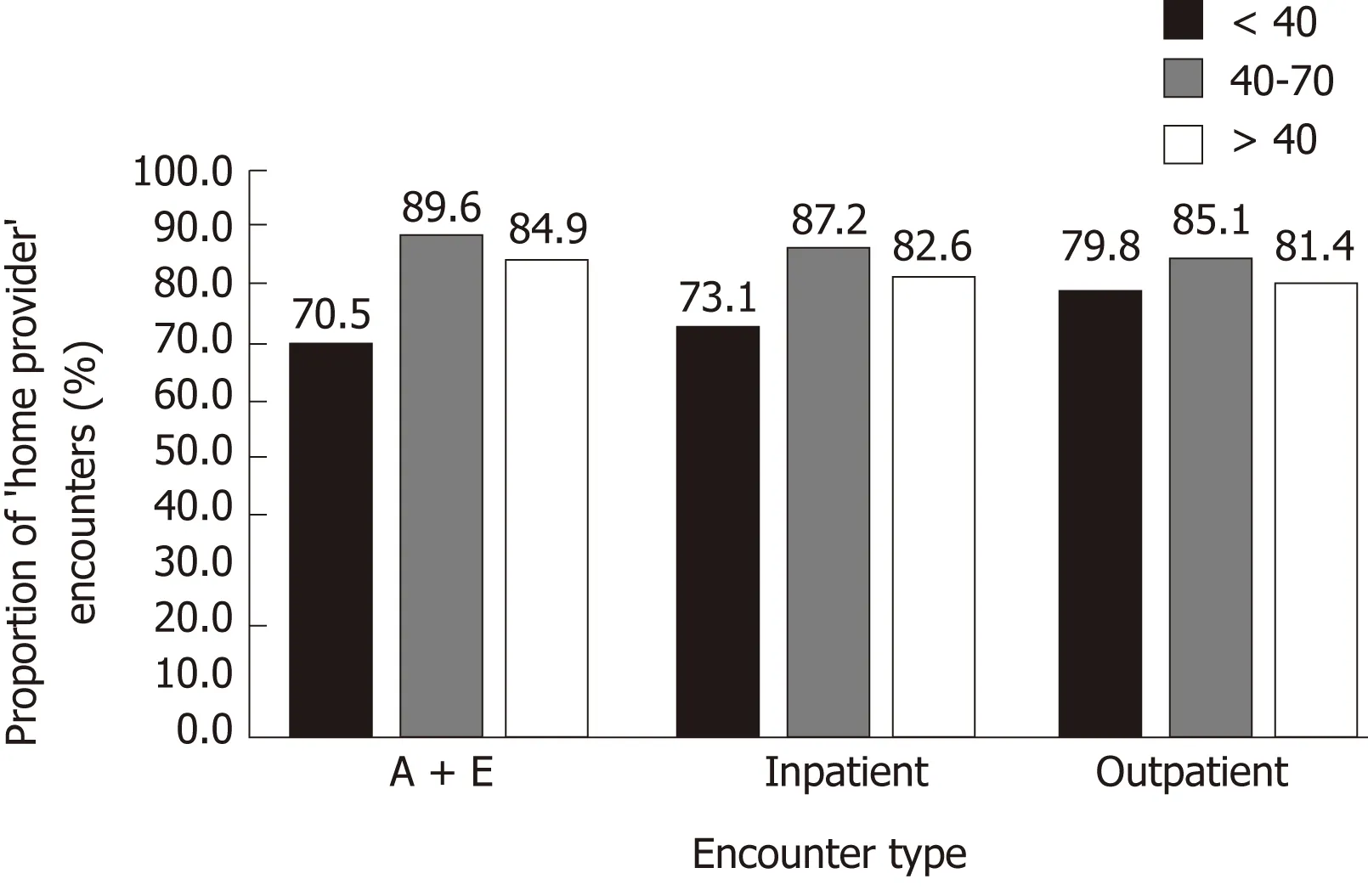
Figure 3 Proportion of ‘home provider’ encounters per age for three age bands, <40, 40-70 and > 70 years.
In conclusion, to ensu re quality and safe care for patients w ith IBD, p roviders shou ld have access to the righ t in form ation abou t the right patient at the right tim e.Find ings from this w ork have show n that patients w ith IBD often transition betw een d ifferent hospital p roviders in m u ltip le settings. This m ay act as a barrier to accessing up-to-date patien t health in form ation and negatively im pact care. These find ings shou ld encou rage and assist the developm ent of m echanism s to enable effective and efficient coord ination of care betw een p roviders that share the care of IBD patients.
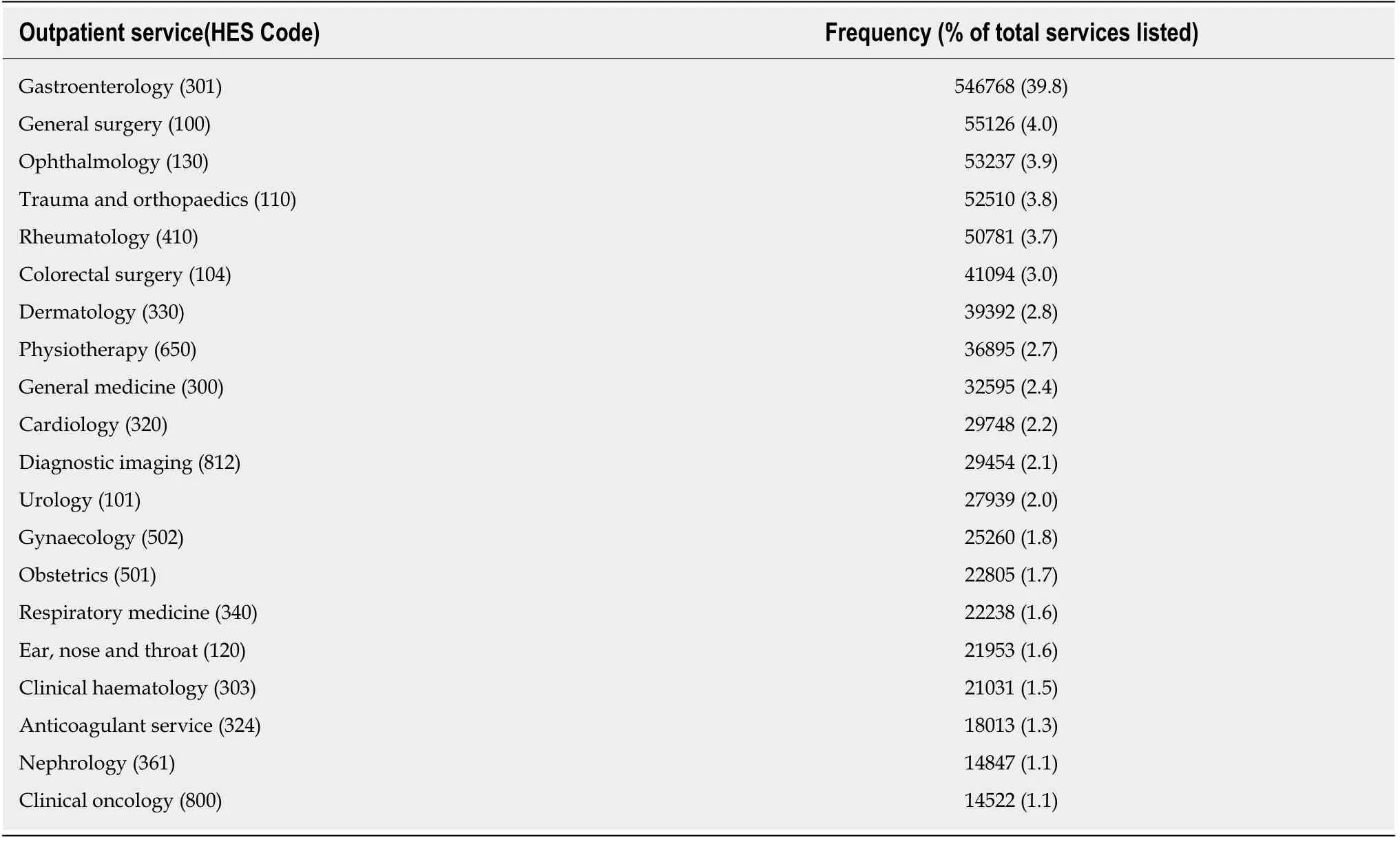
Table 2 The 20 most frequently accessed outpatient services and corresponding proportion of total outpatient services
ARTICLE HIGHLIGHTS
Research background
In flamm atory bow el d isease (IBD) is a ch ronic, in flamm atory d isorder characterised by both intestinal and extra-in testinal pathology. Patients m ay receive both em ergency and elective care from several p rov iders, o ften in d ifferen t hosp ital settings. Poorly m anaged transitions o f care betw een p roviders can lead to inefficiencies in care and patient safety issues. To ensu re that the sharing of patien t in form ation betw een p rov iders is app rop riate, tim ely, accu rate and secu re,effective data-sharing in frastructu re needs to be developed. To op tim ise in ter-hosp ital datasharing for IBD patien ts, w e need to better understand patterns o f hosp ital encoun ters in this group.
Research motivation
There is lim ited data on the types o f hosp ital serv ices accessed by patien ts w ith IBD and the frequency and location o f hosp ital encoun ters. Iden tification o f patterns of hosp ital care can guide in ter-hosp ital data-sharing and care coord ination w hich m ay im p rove con tinuity of care for these patien ts.
Research objectives
This study aim ed to identify and quan tify the hosp ital services accessed by patients w ith IBD in Eng land.
Research methods
This retrospective observational study used Hosp ital Ep isode Statistics, a large adm inistrative dataset in N ational H ealth Serv ice in Eng land, to iden tify characteristics o f hosp ital care encoun ters for IBD patients. The p roportion of encounters w ith p roviders other than the patien ts usual ‘hom e p rovider’ o f IBD care was calcu lated, in add ition to associations w ith patien t age,location and type of specialist p roviders attended.
Research results
The p roportion of encounters w ith hosp itals other than the usual gastroentero logy ‘hom e p rovider’ for 95055 IBD patien ts was up to 26.7% for accident and em ergency encoun ters,follow ed by 16.9% for outpatient and 12.2% for inpatient encounters. Patients living in cities and younger patients w ere less likely to attend their ‘hom e p rovider’ for hospital services. The m ost comm on ly attended ou tpatient specialty services w ere gastroenterology, general surgery and ophthalm ology.
Research conclusionsUp to one in fou r acciden t and em ergency encounters for patien ts w ith IBD in Eng land w ere w ith a d ifferen t p rovider to the patien t’s usual gastroen tero logy ‘hom e p rov ider’ of IBD care.IBD patien ts also often attended other hosp itals for a range of ou tpatien t and inpatient services.These find ings em phasise the im portance o f develop ing effective data-sharing strategies betw een hosp itals to m aintain continuity of in form ation and con tinuity of care for IBD patien ts.
Research perspectives
Find ings from this study p rovide a national-level view o f transitions o f care betw een hosp itals for patien ts w ith IBD in Eng land. W e have show n that certain g roups o f patien ts, includ ing younger patients and those based in m etropolitan areas, have m ore frequent transitions o f care and m ay be a su itab le target for fu rther research and in terventions to im p rove care con tinu ity.Fu rther qualitative and quan titative research is needed to understand the im p lications o f these find ings and im p rove in ter-hosp ital data-sharing.
杂志排行

World Journal of Gastroenterology的其它文章
- Microbial metabolites in non-alcoholic fatty liver disease
- Recent advances in gastric cancer early diagnosis
- Evolving screening and surveillance techniques for Barrett's esophagus
- Proton pump inhibitor: The dual role in gastric cancer
- Herbs-partitioned moxibustion alleviates aberrant intestinal epithelial cell apoptosis by upregulating A20 expression in a mouse model of Crohn’s disease
- Analysis of the autophagy gene expression profile of pancreatic cancer based on autophagy-related protein microtubule-associated protein 1A/1B-light chain 3