糖类抗原19-9、糖类抗原50和糖类抗原242联合检测对可手术胰腺癌的临床诊断价值
2019-01-08窦荣汉周国明张彬叶柳青
窦荣汉 周国明 张彬 叶柳青


[摘要]目的 應用Logistic回归和受试者工作特征(ROC)曲线分析糖类抗原19-9(CA19-9)、糖类抗原50(CA50)和糖类抗原242(CA242)在Ⅰ~Ⅲ期可手术胰腺癌中的临床诊断价值。方法 回顾性分析2016年1月~2018年12月在浙江省肿瘤医院住院并接受过规范手术治疗的246例胰腺癌患者的临床资料作为胰腺癌组,另选取同期接受手术的128例胰腺良性肿瘤患者作为对照组。采用化学发光免疫分析(CLIA)法检测患者血清中的CA19-9、CA50和CA242的表达水平;比较两组患者血清中的CA19-9、CA50和CA242的表达水平;比较胰腺癌组中不同肿瘤(TNM)分期患者血清中的CA19-9、CA50和CA242水平;采用Logistic回归和ROC曲线计算并比较各指标单项检测及联合检测时的ROC-曲线下面积(AUC)、灵敏度、特异性及准确率。结果 胰腺癌组血清中的CA19-9、CA50和CA242水平高于对照组,差异均有统计学意义(P<0.05)。在246例可切除胰腺癌中,随着胰腺癌肿瘤(TNM)分期的增加,血清CA19-9、CA50和CA242水平逐渐升高,差异均有统计学意义(P<0.05)。Logistic回归模型为Logit(P)=-0.877+0.031Y CA19-9+0.007Y CA50-0.034Y CA242。三项联合检测的AUC、灵敏度、准确率高于CA19-9、CA50和CA242单项检测,特异性低于CA19-9、CA50和CA242单项检测,差异均有统计学意义(P<0.05)。结论 血清CA19-9、CA50和CA242联合检测有助于可切除胰腺癌的临床诊断和病情评估,值得临床推广应用。
[关键词]胰腺癌;肿瘤标志物;受试者工作特征曲线;Logistic回归分析
[中图分类号] R735.9 [文献标识码] A [文章编号] 1674-4721(2019)11(b)-0012-05
Clinical diagnostic value of combined detection of carbohydrate antigen 19-9, carbohydrate antigen 50 and carbohydrate antigen 242 in operative pancreatic cancer
DOU Rong-han1,2,3 ZHOU Guo-ming1,2,3 ZHANG Bin1,2,3 YE Liu-qing1,2,3
1. Institute of Oncology and Basic Medicine, Chinese Academy of Sciences, Zhejiang Province, Hangzhou 310022, China; 2. Department of Clinical Laboratory, Cancer Hospital Affiliated to University of Chinese Academy of Sciences, Zhejiang Province, Hangzhou 310022, China; 3. Department of Clinical Laboratory, Zhejiang Tumor Hospital, Hangzhou 310022, China
[Abstract] Objective To use the Logistic regression and receiver operating characteristic (ROC) curves to analyze saccharide antigens 19-9 (CA19-9), carbohydrate antigen 50 (CA50) and carbohydrate antigen 242 (CA242) in stage Ⅰ-Ⅲ operable pancreatic cancer clinical diagnostic value. Methods The clinical data of 246 patients with pancreatic cancer who were hospitalized in Zhejiang Cancer Hospital from January 2016 to December 2018 and received standard surgical treatment were analyzed retrospectively as the pancreatic cancer group, and 128 patients with pancreatic benign tumor who received surgery at the same time were selected as the control group. The levels of CA19-9, CA50 and CA242 in serum of patients were detected by chemiluminescent immunoassay (CLIA). The expression levels of CA19-9, CA50 and CA242 in serum of the two groups were compared. The serum CA19-9, CA50 and CA242 levels of patients with different TNM stages in pancreatic cancer group were compared. The area under curve (AUC) of ROC, sensitivity, specificity and accuracy were calculated by Logistic regression and ROC curve. Results The levels of CA19-9, CA50 and CA242 in serum of pancreatic cancer group were higher than those of control group, the differences were statistically significant (P<0.05). In 246 cases of resectable pancreatic cancer, the levels of CA19-9, CA50 and CA242 increased with the increase of TNM stage, the differences were statistically significant (P<0.05). The regression model was Logit(P)=-0.877+0.031Y CA19-9+0.007Y CA50-0.034Y CA242. The AUC, sensitivity and accuracy of the three combined tests were higher than those of CA19-9, CA50 and CA242, and the specificity was lower than that of CA19-9, CA50 and CA242, the differences were statistically significant (P<0.05). Conclusion The combined detection of serum CA19-9, CA50 and CA242 is helpful to the clinical diagnosis and condition evaluation of resectable pancreatic cancer, which is worthy of clinical application.
[Key words] Pancreatic cancer; Tumor markers; Receiver operating characteristic curves; Logistic regression analysis
胰腺癌是常见的消化系统恶性肿瘤,其发病机制尚未明确,发病原因与吸烟、饮酒、高脂高蛋白饮食等有关[1-3]。胰腺癌恶性程度高、病情进展快,早期治疗能改善预后并提高总体生存率,但由于其早期临床特征无显著特异性,漏诊率极高,大部分患者就诊时已进展为中晚期,预后极差,因此对胰腺癌的早期诊断尤为重要[4-7]。血清肿瘤标志物检测的异常早于影像学检查的异常,其标本易获取,可重复检测,且与肿瘤的发生发展有一定相关性,因此,选择适当的肿瘤标志物联合检测可提升检测的灵敏度与特异性[8-9]。本研究应用Logistic回归和受试者工作特征(ROC)曲线分析糖类抗原19-9(CA19-9)、糖类抗原50(CA50)和糖类抗原242(CA242)在Ⅰ~Ⅲ期可手术胰腺癌中的临床诊断价值,现报道如下。
1资料与方法
1.1一般资料
回顾性分析2016年1月~2018年12月在浙江省肿瘤医院住院并接受过规范手术治疗的246例胰腺癌患者的临床资料作为胰腺癌组,另选取同期接受手术的128例胰腺良性肿瘤患者作为对照组。胰腺癌组中,男148例,女98例;年龄43~84岁,平均(63.37±8.33)岁。对照组中,男71例,女57例;年龄12~79岁,平均(54.32±12.75)岁。两组患者的一般资料比较,差异无统计学意义(P>0.05),具有可比性。纳入标准:①术前未行化疗等其他治疗者;②术后常规病理证实为胰腺良、恶性肿瘤者;③具有完整的临床、病理资料者。排除标准:①术前已行其他治疗者;②手术不能切除病灶者;③合并胰腺外其他器官恶性肿瘤史者。本研究经医院医学伦理委员会审核批准。
1.2检测方法
1.2.1样本采集 全部患者均于入院次日(术前)采集空腹静脉血5 ml,室温静置30 min后以3000 r/min离心10 min,取上层血清待检。所有标本均无黄疸、溶血、脂浊等情况。
1.2.2血清标志物检测 血清CA19-9、CA50和CA242含量均采用化学发光免疫分析(CLIA)法检测,CA19-9[西门子医学诊断产品(上海)有限公司,批号:23388437]、CA50(深圳市新产业生物医学工程股份有限公司,批号:0371800102)、CA242(深圳市新产业生物医学工程股份有限公司,批号:0611800103),严格按照各厂家提供的试剂盒说明书进行操作。
1.3观察指标及评价标准
比较两组患者血清中的CA19-9、CA50和CA242的表达水平;比较胰腺癌组中不同肿瘤(TNM)分期患者血清中的CA19-9、CA50和CA242水平;進一步联合Logistic回归和ROC曲线计算并比较各指标单项检测及联合检测时的ROC-曲线下面积(AUC)、灵敏度、特异性及准确率。①以CA19-9>37.00 U/ml,CA50>25.00 U/ml,CA242>20.00 U/ml为胰腺癌诊断的cut-off值。②灵敏度=真阳性例数/(真阳性+假阴性)例数×100%;特异性=真阴性例数/(真阴性+假阳性)例数×100%;准确率=(真阳性+真阴性)例数/(真阳性+假阴性+真阴性+假阳性)例数×100%。
1.4统计学方法
采用统计学软件SPSS 22.0分析数据,符合正态分布的计量资料以均数±标准差(x±s)表示,采用t检验;不符合正态分布的计量资料以M(P25,P75)表示,采用Mann-Whitney非参数检验;多组间比较采用单因素方差分析;采用Logistic回归模型及ROC曲线评估各指标的诊断价值,预测ΔCI≥15%的效能,并确定各参数最佳临界值,以P<0.05为差异有统计学意义。
2结果
2.1两组患者血清中CA19-9、CA50和CA242表达水平的比较
胰腺癌组患者的血清CA19-9、CA50和CA242的表达水平高于对照组,差异均有统计学意义(P<0.05)(表1)。
2.2胰腺癌组患者不同TNM分期血清中CA19-9、CA50和CA242表达水平的比较
胰腺癌组患者中随着TNM分期的增加,血清中CA19-9、CA50和CA242的表达水平逐渐升高,差异均有统计学意义(P<0.05)(表2)。
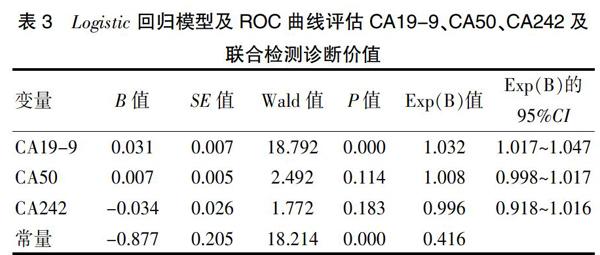
2.3 Logistic回归模型及ROC曲线评估CA19-9、CA50、CA242及联合检测的诊断价值
2.3.1 Logistic回归模型评估CA19-9、CA50、CA242及联合检测诊断价值 以病理结果为应变量,CA19-9、CA50和CA242检测结果为自变量,强制选入作二项分类非条件Logistic回归分析,建立Logistic回归模,Logit(P)=-0.877+0.031Y CA19-9+0.007Y CA50-0.034Y CA242(表3)。
2.3.2 ROC曲线评估CA19-9、CA50、CA242及联合检测的诊断价值 三项联合检测的AUC值高于CA19-9、CA50和CA242单项检测,差异均有统计学意义(P<0.05)(表4、图1)。
2.4 CA19-9、CA50、CA242检测及联合检测对可切除胰腺癌的诊断效能
三项联合检测的灵敏度和准确率高于CA19-9、CA50和CA242单项检测,特异性低于CA19-9、CA50和CA242单项检测,差异均有统计学意义(P<0.05)(表5)。
3讨论
CA19-9、CA50和CA242均为常见的肿瘤标志物,在消化系统恶性肿瘤患者的血清中均有不同程度的升高,尤其是胰腺癌患者的血清中其浓度升高更为明显[10-11]。李静等[12]研究显示,胰腺癌组血清中的CA19-9水平明显高于良性胰腺疾病组与正常对照组(P<0.01)。Lei等[13]通过分析112例Ⅰa-Ⅱb期胰腺导管腺癌患者、100例良性胰腺病变患者和90例健康健康体检者血清中CA19-9、CA50和CA242的表达水平,恶性组血清中的CA19-9,CA242和CA50表达水平和阳性率均显著高于良性组和健康对照组。本研究结果显示,胰腺癌组患者的血清CA19-9、CA50和CA242的表达水平高于对照组,差异均有统计学意义(P<0.05),提示检测外周血中的CA19-9、CA50和CA242水平,有助于提高胰腺癌的检出率。本研究结果显示,胰腺癌组患者中随着TNM分期的增加,血清中CA19-9、CA50和CA242的表达水平逐渐升高,差异均有统计学意义(P<0.05),提示血清CA19-9、CA50和CA242水平随着病程的进展而明显升高。
Cao等[14]检测了119例可切除胰腺癌患者术前CA19-9的表达水平,结果显示,术前血清CA19-9的阳性检出率为81.51%,高于其他指标。曾万里等[15]对比了77例胰腺癌患者和77例健康体检人群后发现胰腺癌组血清中的CA19-9阳性率显著高于对照组。林文科等[16]研究显示,血清CA19-9、CA242和CA50在胰腺癌中的阳性率分别达82.2%、67.1%、39.7%。Zhang等[17]的一项包含21项研究共3497个病例的Meta分析显示,血清CA19-9和CA242对胰腺癌的诊断灵敏度分别为75.40%、67.80%,特异度为77.60%,83.00%,其中CA19-9和CA242联合检测能提高诊断灵敏度至89.95%,特异度为75.95%。本研究结果显示,在对胰腺可切除肿物的良恶性判定中,单项检测时血清CA19-9的AUC值最高(0.860);诊断灵敏度同样是血清CA19-9最高(74.80%);诊断特异性方面,血清CA19-9、CA50、CA242检测均>90.00%。三项联合检测的AUC(0.886)值高于CA19-9、CA50和CA242单项检测,差异均有统计学意义(P<0.05),三项联合检测的灵敏度和准确率高于CA19-9、CA50和CA242单项检测,特异性低于CA19-9、CA50和CA242单项检测,差异均有统计学意义(P<0.05)。研究结果显示[18],胆汁淤积者血清中的CA19-9水平有不同程度的升高,良性胰腺疾病患者均有不同程度的黄疸,但不如胰腺癌患者升高明显,CA242与胆汁淤积程度无关,因此CA19-9对胰腺癌诊断的特异性较CA242低。综合运用胰腺肿瘤的血清标志物可提高胰腺癌的临床诊断能力,为更多的胰腺癌患者提供手术机会。
综上所述,血清标志物的检测是临床诊断胰腺癌的重要手段[19-21],综合运用胰腺肿瘤的血清标志物可提高胰腺癌的临床诊断能力,血清CA19-9、CA50和CA242联合检测有助于可切除胰腺癌的临床诊断和病情评估,为更多的胰腺癌患者提供手术机会,值得临床推广应用。
[参考文献]
[1]郑旭,邱雄,邵泽勇,等.胰腺癌患者血清CEMIP、CA19-9和CA242水平变化及其临床意义[J].实用肝脏病杂志,2019,22(2):280-284.
[2]Jiang YX,Spurny M,Schübel R,et al.Changes in pancreatic fat content following diet-induced weight loss[J].Nutrients,2019,11(4): E912.
[3]Hao S,Huo S,Du Z,et al.MicroRNA-related transcription factor regulatory networks in human colorectal cancer[J].Med(Baltimore),2019,98(15):e15158.
[4]Zhou B,Xu JW,Cheng YG,et al.Early detection of pancreatic cancer:where are we now and where are we going?[J].Int J Cancer,2017,141(2):231-241.
[5]Okano K,Suzuki Y.Strategies for early detection of resectable pancreatic cancer[J].World J Gastroenterol. 2014,20(32):11 230-11 240.
[6]Kikuyama M,Kamisawa T,Kuruma S,et al.Early diagnosis to improve the poor prognosis of pancreatic cancer[J].Cancers(Basel),2018,10(2):E48.
[7]Gao HL,Liu L,Qi ZH,et al.The clinicopathological and prognostic significance of PD-L1 expression in pancreatic cancer:a meta-analysis[J].Hepatobiliary Pancreat Dis Int,2018,17(2):95-100
[8]梁巍,胡雨薇,應媛媛.联合检测D-二聚体、糖类抗原-199、癌胚抗原在结直肠癌患者中的临床价值[J].中国实验诊断学,2019,23(1):83-85.
[9]Liu X,Zheng W,Wang W,et al.A new panel of pancreatic cancer biomarkers discovered using a mass spectrometry-based pipeline[J].Br J Cancer,2017,117(12):1846-1854.
[10]任勇亚,杜丽坚,任鸿.血清CA50、CA199、CA242、CA724在胃癌诊断及预后评估中的应用[J].临床医学研究与实践,2018,3(36):119-120.
[11]朱剑峰,李志辉,朱红静,等.CEA、CA199、CA724、CA242、 CA125、CA50对消化道肿瘤的诊断价值[J].实用癌症杂志,2014,29(5):501-502.
[12]李静,梁晓芳,翟桂兰.血清CA19-9、CA125和CEA联合检测在胰腺癌诊断中的应用[J].吉林大学学报(医学版),2014,40(6):1252-1255.
[13]Lei XF,Jia SZ,Ye J,et al.Application values of detection of serum CA19-9,CA242 and CA50 in the diagnosis of pancreatic cancer[J].J Biol Regul Homeost Agents,2017,31(2):383-388.
[14]Cao J,Fu Z,Gao L,et al.Evaluation of serum D-dimer,fibrinogen,and CA19-9 for postoperative monitoring and survival prediction in resectable pancreatic carcinoma[J].World J Surg Oncol,2017,15(1):48.
[15]曾万里,叶廷云.CEA、CA19-9、CA125联合检测在胰腺癌诊治中的应用[J].中华肿瘤防治杂志,2016,23(S2):182,201.
[16]林文科,吴吉芳,郑志昂.多种肿瘤标志物在胰腺癌中的诊断价值及相关性研究[J].中国免疫学志,2017,33(1):120-125.
[17]Zhang Y,Yang J,Li H,et al.Tumor markers CA19-9,CA242 and CEA in the diagnosis of pancreatic cancer:a meta-analysis[J].Int J Clin Exp Med,2015,8(7):11 683-11 691.
[18]徐笑红,束新华,卢加荪,等.血清CA242、CA19-9在胰腺癌诊断和治疗中的应用评估[J].标记免疫分析与临床,2001,8(3):185-187.
[19]Gu YL,Lan C,Pei H,et al.Applicative value of serum CA19-9,CEA,CA125 and CA242 in diagnosis and prognosis for patients with pancreatic cancer treated by concurrent chemoradiotherapy[J].Asian Pac J Cancer Prev,2015,16(15):6569-6573.
[20]邢瑞青,彭道荣.血清CA19-9、PIVKA-Ⅱ、VEGF联合检测对胰腺癌的诊断价值研究[J].国际检验医学杂志,2019, 40(5):554-557.
[21]Gallego J,López C,Pazo-Cid R,et al.Biomarkers in pancreatic ductal adenocarcinoma[J].Clin Transl Oncol,2017, 19(12):1430-1437.
(收稿日期:2019-04-09 本文編辑:刘克明)
