氩氦刀冷冻消融术在颅内肿瘤切除术中的应用
2017-11-22周宇浩出良钊
周宇浩 出良钊
氩氦刀冷冻消融术在颅内肿瘤切除术中的应用
周宇浩 出良钊
目的总结氩氦刀冷冻消融术辅助颅内肿瘤切除术的疗效。方法与结果共11例原发性颅内肿瘤患者(包括7例胶质瘤和4例脑膜瘤),肿瘤分别位于左侧额叶4例、左侧额顶叶2例、左侧颞叶2例、右侧颞顶叶3例,均采用氩氦刀冷冻消融术辅助颅内肿瘤切除术。7例胶质瘤全切除4例、部分切除3例,4例脑膜瘤均全切除;平均术中出血量80 ml,平均手术时间80 min;术后临床症状改善;复查头部CT或MRI未发生再出血;术后平均随访4年,无一例发生颅内感染等手术相关或术后并发症,未见肿瘤复发。结论氩氦刀冷冻消融术适用于不同部位和不同直径的颅内肿瘤,安全有效、手术相关和术后并发症较少、再出血和肿瘤复发风险较低,是一种安全、有效、经济的辅助手术方法。
中枢神经系统肿瘤; 氩; 氦; 冷冻外科手术; 神经外科手术
神经外科常见的颅内肿瘤常因术中出血量较大、肿瘤质地不均匀而增加手术切除难度和术中风险,术后常伴各种并发症,如再次出血、颅内水肿等。氩氦刀冷冻消融术采用低温技术,具有杀伤范围精确、创伤轻微、疗效迅速等特点,可以有效减少术中和术后并发症、缩短恢复时间。贵州医科大学附属医院神经外科2011年11月-2015年8月术中采用氩氦刀冷冻消融术辅助切除11例颅内肿瘤,效果满意,现总结报告如下。
对象与方法
一、研究对象
11例原发性颅内肿瘤患者,其中胶质瘤7例,脑膜瘤4例;男性6例,女性5例;年龄19~59岁,平均39岁;病程1~8个月,平均4个月;临床主要表现为头晕头痛7例(63.64%),头晕伴抽搐发作4例(36.36%)。头部CT和MRI检查显示,肿瘤位于左侧额叶4例(36.36%),左侧额顶叶2例(18.18%),左侧颞叶2例(18.18%),右侧颞顶叶3例(28.27%);肿瘤最大径2~6 cm,平均4 cm。
二、研究方法
1.手术治疗 采用美国Endocare公司生产的CYRO careTM低温手术系统,配备8刀头插入式超导冷冻枪。患者仰卧位或健侧卧位,于全身麻醉下常规开颅,精细分离肿瘤组织与正常脑组织,并以脑棉片分隔保护正常脑组织,根据术前CT和(或)MRI所示肿瘤部位、最大径、周围血管走行和血供,选择适宜尺寸的手术刀头,常用手术刀头直径为2、3、5和8 mm共4种类型:为减轻对周围脑组织的损伤,通常选择3或5 mm刀头,将刀头插入肿瘤内短时多次冷冻肿瘤,以免影响肿瘤周围正常脑组织;肿瘤范围较大时,选择小直径(2或3 mm)刀头,环形植入3~4枚刀头至肿瘤中心,刀头之间间隔15~20 mm;肿瘤范围较小时,选择5 mm刀头,直接插入肿瘤中心,多次插入,逐层完成肿瘤囊内切除,刀头插入深度控制在10 mm内。充分显露肿瘤,根据术前MRI图像提示插入1枚或多枚刀头,冷冻范围控制在肿瘤边界1 cm内。先予以氩气降温至⁃140℃并维持5 min,直视下肿瘤逐渐形成“冰球”状(图1);再予以氦气,1 min内复温至37℃,重复此步骤2~3次,随即拔除刀头,肿瘤穿刺孔以明胶海绵止血。然后根据冷冻消融范围逐步完成肿瘤囊内切除(图2),尤其是肿瘤体积较大时,无法一次性完成肿瘤囊内全切除,通常选择多个靶点,予多次分块冷冻消融并肿瘤囊内切除,直至肿瘤组织充分缩小后,于手术显微镜下精细分离肿瘤基底部与正常脑组织,全切除肿瘤。
2.疗效和安全性评价 (1)疗效评价:记录患者肿瘤全切除率、术中出血量、手术时间、术后症状改善,以及影像学复查再出血情况。(2)安全性评价:记录患者手术相关和术后并发症情况。

图1 术中采用直径3 mm氩氦刀刀头冷冻肿瘤,形成“冰球”状图2 手术切除复温的肿瘤组织Figure 1 Argon⁃helium knife of diameter 3 mm was used to frozen the tumor and form an "ice ball". Figure 2 Resectthe rewarming tumor tissue.
结 果
本组7例胶质瘤全切除4例、部分切除3例,4例脑膜瘤均全切除;术中出血量30~200 ml、平均为80 ml,无一例需术中或术后输血;手术时间60~120 min,平均为80 min;术前头晕、头痛、抽搐发作症状均明显改善;术后复查CT或MRI,无一例发生再出血。术后随访2~6年、平均4年,无一例发生颅内感染等手术相关或术后并发症;所有患者均恢复良好,未见肿瘤复发。
典型病例
例1 男性患者,52岁,因左侧下肢无力4月余,于2015年3月30日入院。患者4月余前无明显诱因突然出现左侧下肢无力伴行走不稳,活动中跌倒2次,无头痛、头晕,无四肢抽搐、口吐白沫,无视物模糊,无恶心、呕吐,无咳嗽、咳痰,无胸闷、气促和呼吸困难,无大小便失禁。入院后体格检查:神志清楚,语言流利,查体合作;双侧瞳孔等大、等圆,直径约3 mm,对光反射灵敏,视力可,1 m外能正确数指,眼球各向活动充分,无斜视、眼震;可站立和缓慢行走,但站立和行走不稳;左下肢肌力5级、肌张力正常,余肢体肌力和肌张力均正常;双手指鼻试验可,Romberg征阴性,生理反射存在,病理反射征未引出,脑膜刺激征阴性。实验室检查各项指标均于正常值范围。影像学检查:头部MRI增强扫描显示,右侧大脑镰旁占位性病变,可疑脑膜瘤(图3a)。遂于2015年4月2日行氩氦刀冷冻消融技术辅助脑膜瘤切除术,术中可见近矢状窦旁硬脑膜出血明显,予止血纱布和明胶海绵压迫止血,沿骨窗边缘剪开硬脑膜,向中线翻开,显露肿瘤组织顶部,呈暗红色,边界清晰,血运丰富,选用5 mm氩氦刀刀头,插入肿瘤中心后予以氩气降温至⁃110℃,维持3 min,部分肿瘤组织形成“冰球”状,再予以氦气复温至37℃,重复此步骤3次,形成大小5 cm×4 cm×5 cm、质地较硬的肿瘤组织,完成肿瘤囊内全切除,术中出血量约30 ml,手术时间100 min。术后复查CT显示,脑膜瘤术后改变,未见明显再出血和水肿带(图3b)。术后予以脱水降低颅内压、预防癫发作、抗感染、补液和营养神经等对症治疗。患者术后12 d出院,随访至今,复查CT未见肿瘤复发,四肢肌力恢复良好,可自主站立和行走。
例2 男性患者,36岁,主因头晕6月余,症状加重1周,于2015年5月5日入院。患者6月余前无明显诱因间断性晨起或空腹时出现头晕,持续时间≤30 s,无头痛、恶心、呕吐,无视物模糊、视力减退,发病初期偶有头晕(1次/15 d);1周前头痛、头晕症状加重,难以忍受,偶有失语,自觉记忆力减退。入院后体格检查:神志清楚,语言流利,查体合作;双侧瞳孔等大、等圆,直径约3 mm,对光反射灵敏,眼球各向活动充分,双眼视物可,无眼震;四肢肌力5级,肌张力正常;生理反射存在,病理反射未引出,脑膜刺激征阴性。入院时Glasgow昏迷量表(GCS)评分15分。实验室检查各项指标均于正常值范围。影像学检查:头部MRI显示,左侧颞叶占位性病变,可疑胶质瘤(图4a)。遂于2015年5月12日行氩氦刀冷冻消融术辅助胶质瘤切除术,术中弧形剪开硬脑膜后可见近颅中窝底灰白色肿瘤组织,以脑棉片保护皮质静脉和脑组织后插入3 mm氩氦刀刀头,予以氩气降温至⁃120℃,维持4 min,部分肿瘤组织形成“冰球”状,再予以氦气复温至37℃,反复4次,形成大小约5 cm×3 cm×4 cm、质地较硬的肿瘤组织,完成肿瘤囊内全切除,术中出血量约35 ml,手术时间90 min。术后复查MRI显示,胶质瘤术后改变,未见明显再出血和水肿带(图4b)。术后予以脱水降低颅内压、预防癫发作、抗感染、补液和营养神经等对症治疗。患者术后10 d出院,随访至今,复查MRI未见肿瘤复发。
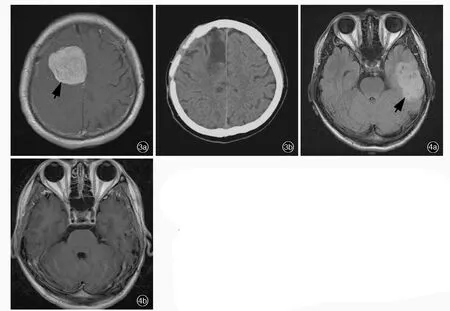
图3 手术前后头部影像学检查所见 3a 术前横断面增强T1WI显示,右侧大脑镰旁脑膜瘤(箭头所示) 3b 术后横断面CT显示病灶消失,未见明显术区水肿和再出血 图4 手术前后头部MRI检查所见 4a 术前横断面FLAIR成像显示,左侧颞叶胶质瘤(箭头所示) 4b 术后横断面增强T1WI显示病灶消失,未见明显术区水肿和再出血Figure 3 Head imaging findings before and after surgery Preoperative axial enhanced T1WI showed meningioma located in right cerebral parafalx(arrow indicates,Panel 3a).Postoperative axial CT showed the lesion was disappeared. No obviousedema orrebleeding wasfound (Panel3b).Figure 4 Head MRI findings before and after surgery Preoperative axial FLAIR showed lefttemporallobe glioma (arrow indicates,Panel4a).Postoperative axial enhanced T1WI showed the lesion was disappeared,with no obvious edema or rebleeding(Panel 4b).
讨 论
氩氦刀冷冻消融术作为一种新型手术方式,众多研究均支持该项技术可以对不同部位肿瘤进行切除,如肺癌、胰腺癌、肝癌、前列腺癌等[1⁃2]。冷冻技术最早开始于19世纪,通过液氮控温设备和立体定向技术治疗帕金森病,至20世纪40年代方有学者对其机制进行研究[3],此后该项技术应用于颅内肿瘤的切除,主要包括胶质瘤和脑膜瘤等。肿瘤血供丰富时,术中止血和术后预防脑水肿成为肿瘤切除术成功与否的关键。一般的双极电凝止血在颅内肿瘤切除术中常因止血困难而延长手术时间、增加术中出血量,使术野显露不清,干扰对肿瘤周围组织的切除,增加手术风险。冷冻技术通过降低肿瘤组织温度而阻断血供,但是由于降温速度过快、冷冻范围过大且易出现并发症等,冷冻技术用于颅内肿瘤切除术一直是亟待解决的热点问题。液氮控温设备对温度控制较差,1993年氩氦刀问世,氩氦刀冷冻消融术恰可以解决上述问题,且操作简单、安全有效、手术成功率高、手术相关和术后并发症发生率低,不仅可以减少肿瘤残留风险,还可以规避过度低温造成的肿瘤毗邻组织或神经损伤。既往研究显示,氩氦刀冷冻消融术用于颅内肿瘤的切除可以迅速固定刀头周围肿瘤组织,形成肿瘤囊内切除过程中无血操作,减少术中止血操作、缩短手术时间,使肿瘤体积充分缩小,再进一步分离肿瘤周围组织,从而完成对肿瘤组织及其基底部的处理,减少对脑组织牵拉和对肿瘤周围重要功能区的干扰,且无明显手术相关和术后并发症[4⁃6]。Maroon等[7]的研究显示,术中实时影像学检查使得对肿瘤及其周围组织的冷冻变得前所未有的可视化,中枢神经系统低温检测变得可行有效。使用新型冷冻仪器进行手术的疗效较好,有利于切除脑肿瘤和脊髓肿瘤,减少术中出血量,尤以切除上矢状窦和窦汇区残留肿瘤疗效显著。我们的前期研究对血供较丰富的26例脑膜瘤患者进行载瘤动脉栓塞术联合氩氦刀冷冻消融术,术中出血量少,术后头部MRI显示无肿瘤残留,且无明显手术相关和术后并发症,经过长期(10年)随访,24例恢复良好、2例轻残,无植物状态生存或死亡病例[8]。本研究11例颅内肿瘤患者,由于肿瘤体积巨大、位置特殊且血供丰富,肿瘤组织与正常脑组织不易分离,分离过程中因牵拉易造成出血或损伤,极大影响手术疗效和患者预后,亦难以全切除肿瘤。,氩氦刀冷冻消融术可以冰冻肿瘤组织,形成“冰球”状,在绝大部分肿瘤无血或少血操作情况下切除冰冻部分,显露足够术野,再分离肿瘤基底部与周围脑组织,在减少牵拉和无血操作情况下全切除肿瘤。采用该项技术可以显著降低手术难度,经反复2~3次冰冻和复温,彻底清除病灶。
目前较为常见的颅内肿瘤治疗方法包括射频消融术、冷冻消融术等。射频消融术是通过放射一定频率的射频电流而产生较高频率的电磁波,将射频能转换为热能,通过加热肿瘤组织而使肿瘤细胞凝固坏死。有文献报道,最早用于肝癌切除术的射频止血切割器Habib4X,目前已用于颅内肿瘤的切除,且效果良好,患者预后较好[9]。冷冻消融术与射频消融术原理相反,氩氦刀冷冻消融术通过氩气迅速降低肿瘤组织温度,使其形成“冰球”状,再通过氦气使肿瘤组织迅速复温,以达到摧毁肿瘤的目的。尽管两种方法均对颅内肿瘤的切除有巨大帮助,但二者仍存区别:射频消融术通过升高肿瘤组织温度而达到摧毁肿瘤的目的,但是由于难以精确控制升温范围,术后易发生脑水肿、头痛等并发症;氩氦刀冷冻消融术通过降低肿瘤组织温度,使肿瘤局部微循环改变,机体免疫系统对经冷冻消融的肿瘤组织更加敏感,从而通过自身免疫调节杀灭冰冻病灶边缘的肿瘤组织[2⁃3]。
综上所述,氩氦刀冷冻消融术作为一种安全、有效的新型手术方式,受到神经外科医师的重视并广泛应用于临床。该项技术不仅术中止血效果显著、有效缩短手术时间和降低手术风险,而且通过上调机体抗肿瘤免疫机制,有效阻止肿瘤再生长、降低复发风险。氩氦刀具有不同尺寸刀头,适用于不同部位和不同直径的颅内肿瘤,且刀头经消毒后可重复使用,显著降低经济负担,对于经济状况较为落后地区的患者,是一种经济、有效的手术方法。随着医学技术的日新月异,众多高科技的手术方法逐渐应用于颅内肿瘤切除术,但氩氦刀冷冻消融术仍是一种安全、有效、经济的辅助手术方法。
[1]Tang Y,Yuan ZN,Liu FH,Hao JH.Cryotherapy and cryoimmunotherapy for pancreatic cancer.Zhongguo Zhong Liu Lin Chuang,2012,39:997⁃999[.唐勇,苑占娜,刘凤华,郝继辉.胰腺癌冷冻治疗及冷冻免疫.中国肿瘤临床,2012,39:997⁃999.]
[2]Wang RX,Ren GX.Cryoablation treatment of tumor progression.Zhonghua Lin Chuang Yi Shi Za Zhi(Dian Zi Ban),2015,9:3109⁃3111[.王润湘,任国欣.冷冻消融治疗肿瘤进展.中华临床医师杂志(电子版),2015,9:3109⁃3111.]
[3]Paul SB, Gamanagatti SR, Aneesh MK, Acharya SK.Percutaneous ablative therapy for hepatocellular carcinoma.Natl Med J India,2011,24:347⁃355.
[4]Li P,Li WL,Sun ZF,Guo Z.Status and prospect of argon⁃helium cryosurgery system for the treatment of gliomas.Zhongguo Zhong Liu Lin Chuang,2014,41:345⁃348[.李鹏,李文良,孙增峰,郭志.氩氦刀冷冻消融治疗脑胶质瘤的现状与展望.中国肿瘤临床,2014,41:345⁃348.]
[5]Xia B,Tan YR,Zhang XJ,Su ZY.Nursing care of patients with intracranial tumors patients treated with cryocare surgical system guided by MR.Yi Xue Ying Xiang Xue Za Zhi,2009,19:730⁃731.[夏冰,谭艳榕,张秀菊,苏志莹.MR导向氩氦刀治疗脑肿瘤的护理.医学影像学杂志,2009,19:730⁃731.]
[6]Zhang SZ,Zhang JR,Xu RX,Xu Q,Wang SM.Cryosurgery of cerebralgliomas with cryocare surgicalsystem guided by stereotactic technology.Zhongguo Wei Qin Xi Shen Jing Wai Ke Za Zhi,2000,5:103⁃106[.张世忠,张积仁,徐如祥,徐强,汪森明.立体定向引导氩氦刀靶向冷冻治疗脑胶质瘤.中国微侵袭神经外科杂志,2000,5:103⁃106.]
[7]Maroon JC,Onik G,Quigley MR,Bailes JE,Wilberger JE,Kennerdell JS.Cryosurgery re⁃visited for the removal and destruction of brain,spinal and orbital tumours.Neurol Res,1992,14:294⁃302.
[8]Feng LQ,Yang H,Chu LZ,Li YM,Xiang X,Lü Y.Combination of embolization and argon⁃helium cryoablation in the treatment of 26 meningiomas patients.Zhongguo Yi Yao Dao Kan,2011,13:1708⁃1709[.冯鲁乾,杨华,出良钊,李玉明,向欣,吕莹.氩氦刀联合介入栓塞治疗脑膜瘤26例疗效分析.中国医药导刊,2011,13:1708⁃1709.]
[9]Liu RD,Yin XT,Li Q,Chen ZY,Liu B,Han QS,Zhou YP.Application of radiofrequency ablation in meningioma surgery.Zhonghua Shen Jing Wai Ke Za Zhi,2015,31:241⁃242[.刘瑞东,殷雪涛,李琪,陈卓元,刘斌,韩青松,周忆频.射频消融技术在脑膜瘤手术中的应用.中华神经外科杂志,2015,31:241⁃242.]
2017⁃04⁃17)
The Annual Meeting of American Academy of Addiction Psychiatry 2017
Time:December 7-10,2017
Venue:San Diego,California,USA
Website:www.aaap.org/annual-meeting
Abstract deadline:June 1,2017
The Annual Meeting of American Academy of Addiction Psychiatry 2017 will be held on December 7-10,2017 in San Diego,California,USA.The Annual Meeting and Scientific Symposium provide the latest scientific developments in addiction psychiatry for physicians and allied health professionals who treat patients with substance use disorders(SUD)and mental health disorders.The meeting is structured to encourage interaction among clinicians from various disciplines,approaches and settings.
The Meeting aims to recognize emerging issues and trends in addiction psychiatry and be on the forefront of diagnosis and treatment of substance use disorders and co⁃occurring mental disorders.Participants should be able to:1)identify how to recognize,diagnose,and treat substance use disorders as they change in society.2)Increase their competency in using evidence based psychotherapy,medications and other treatments.3)Improve their knowledge using didactic lectures,skill building workshops,and unique educational formats to support concepts in addiction psychiatry.4)Increase skills to educate peers,colleagues,trainees,patients and the community about addiction psychiatry.
The Meeting can also provide support and education to addiction psychiatrists and clinicians treating patients with substance use disorders.Therefore,participants should be able to:1)utilize and promote evidence⁃based approaches and current treatment guidelines for biopsychosocial treatment of substance use disorders and co⁃occurring mental disorders.2)Network with peers and mentors to find support and guidance in the field of addiction psychiatry.3)Develop and expand current educational curriculum in the field of addiction psychiatry.
The Meeting will demonstrate for trainees the various evidence⁃based approaches,treatments and settings applicable to the field(or practice)of addiction psychiatry.Trainees should be able to:1)identify various career paths in addiction psychiatry available to them. 2)Increase their familiarity with career options and pathways by networking with leaders in addiction psychiatry.3)Enhance their knowledge relevant to early careers in addiction psychiatry.
Application of argon⁃helium cryoablation in resection of intracranial tumors
ZHOU Yu⁃hao1,CHU Liang⁃zhao2
1Grade 2014,Graduate School,Guizhou Medical University,Guiyang 550004,Guizhou,China
2Department of Neurosurgery,the Affiliated Hospital of Guizhou Medical University,Guiyang 550004,Guizhou,China
Corresponding author:CHU Liang⁃zhao(Email:365446506@qq.com)
ObjectiveTo summarize the curative effect of argon⁃helium cryoablation in resection of intracranial tumors.Methods and ResultsA total of 11 patients with primary intracranial tumors,including 7 cases of glioma and 4 cases of meningioma,were enrolled in this study.The tumor was located in left frontal lobe in 4 cases,left fronto⁃parietal lobe in 2 cases,left temporal lobe in 2 cases and right temporo⁃parietal lobe in 3 cases.Argon⁃helium cryoablation was used to assist intracranial tumor resection.Among 7 cases of glioma,4 cases were totally removed and 3 cases were partially resected.Four cases of meningioma were totally removed.The average intraoperative blood loss was 80 ml,and average operation time was 80 min. Postoperative clinical symptoms were improved,and head CT or MRI showed no rebleeding.Patients were followed up for an average of 4 years,and none of them suffered from operation⁃related or postoperative complications such as intracranial infection,or tumor recurrence.ConclusionsArgon⁃helium cryoablation is suitable for intracranial tumors with different diameters and in different locations.It is safe and effective,with few operation⁃related or postoperative complications,less rebleeding and low risk of recurrence,which is a highly efficient and relatively low⁃cost assistant surgical method.
Central nervous system neoplasms; Argon; Helium; Cryosurgery; Neurosurgical procedures
10.3969/j.issn.1672⁃6731.2017.06.011
550004贵阳,贵州医科大学研究生院2014级(周宇浩);550004贵阳,贵州医科大学附属医院神经外科(出良钊)
出良钊(Email:365446506@qq.com)
