三重刺激技术定量评价多系统萎缩患者重复经颅磁刺激治疗效果二例分析
2017-11-22王含王悦崔丽英
王含 王悦 崔丽英
三重刺激技术定量评价多系统萎缩患者重复经颅磁刺激治疗效果二例分析
王含 王悦 崔丽英
研究背景既往研究显示,初级运动皮质予重复经颅磁刺激可以改善皮质脊髓束损害。本研究采用三重刺激技术定量评价2例以帕金森综合征为主要表现的多系统萎缩(MSA⁃P)患者重复经颅磁刺激前后皮质脊髓束功能变化,探讨重复经颅磁刺激对皮质脊髓束损害的改善作用。方法2例MSA⁃P型患者(1例为62岁男性,1例为44岁女性),病程1年,均接受重复经颅磁刺激,采用小指展肌三重刺激技术波幅比和统一多系统萎缩评价量表第二部分(UMSARSⅡ)评价治疗前后皮质脊髓束功能和运动功能。结果2例MSA⁃P型患者治疗前小指展肌三重刺激技术波幅比为28.30%和69.10%,UMSARSⅡ评分22和20分;治疗后即刻小指展肌三重刺激技术波幅比为58.40%和71.70%,UMSARSⅡ评分16和12分,其中例1随访至重复经颅磁刺激后2个月,治疗后1和2个月小指展肌三重刺激技术波幅比分别为90.70%和50.70%,UMSARSⅡ评分17和23分。结论采用三重刺激技术可以定量评价重复经颅磁刺激对MSA⁃P型患者皮质脊髓束损害的改善作用。
诱发电位; 多系统萎缩; 经颅磁刺激
三重刺激技术(TST)是一种可以精确定量评价皮质脊髓束完整性的方法,有应用于多发性硬化(MS)[1⁃2]、肌萎缩侧索硬化症(ALS)[3⁃4]和脑卒中[2,5]的文献报道。研究显示,三重刺激技术评价脱髓鞘或神经退行性变致皮质脊髓束损害的灵敏度是传统经颅磁刺激(TMS)的 2.75 倍[1,6]。三重刺激技术波幅比可以反映激活的脊髓运动神经元比例,既往研究显示其正常值≥90%[6]。晚近研究显示,三重刺激技术在评价多系统萎缩(MSA)[6]和血管性帕金森综合征[7]患者皮质脊髓束损害方面具有重要价值,但此方面的研究仍十分有限。重复经颅磁刺激(rTMS)用于治疗帕金森病(PD)始于1994年[8],目前越来越多的证据显示,该项技术具有一定治疗效果[9⁃10],但其作用机制尚不明确。我们课题小组既往对以帕金森综合征为主要表现的多系统萎缩(MSA⁃P)的研究显示,重复经颅磁刺激可能对刺激局部和功能相关皮质或皮质下区域(包括皮质脊髓束)产生可塑性影响[11]。鉴于此,本研究采用三重刺激技术[12⁃13]对符合很可能 MSA⁃P 型诊断标准[14]的2例MSA⁃P型患者重复经颅磁刺激前后皮质脊髓束功能进行定量评价,以探讨重复经颅磁刺激对皮质脊髓束损害的改善作用。
临床资料
例1 男性,62岁,因头晕、行动迟缓1年余,于2009年2月9日至神经科门诊就诊。患者1年前无明显诱因出现间断性头晕,无天旋地转感,无头痛,站立和行走时显著、平卧时减轻,自觉肢体僵硬,伴颈背部疼痛;症状进行性加重,逐渐出现运动迟缓、双手静止性震颤、讲话时嘴唇震颤,伴双下肢浮肿、排尿不尽和便秘(1次/5~8 d),反复出现肺部感染(具体不详)。患者自发病以来,睡眠欠佳,时有梦魇和手足舞动,打鼾,偶有睡眠呼吸障碍;饮食、精神尚可,体重无明显变化。既往史、个人史及家族史:约3年前开始出现尿频、排尿不尽,逐渐进展至尿失禁,未予特殊处理;2年前行经尿道前列腺电切术,术后症状无明显改善;间断饮酒20年、500 g/次,吸烟约5年(约5支/d),目前已经戒烟10余年;家族史无特殊。门诊体格检查:卧位血压125/80 mm Hg(1 mm Hg=0.133 kPa)、立位 90/70 mm Hg;神志清楚,语言欠清晰,声音低沉,表情淡漠;双侧瞳孔等大、等圆,直径约3 mm,对光反射灵敏,双眼水平眼动充分、垂直眼动受限,Horner征阴性,咽反射减弱,其余脑神经检查未见明显异常;四肢肌力5级,右上肢肌张力增高,呈“铅管”样,余肢体肌张力正常;感觉系统未见异常,双手快复轮替动作缓慢,指鼻试验稳准,可见双手姿势性震颤;腱反射对称活跃,双侧Babinski征阳性,欢呼征可疑阳性,脑膜刺激征阴性。实验室检查各项指标均于正常值范围。头部MRI显示,脑桥和小脑欠饱满。睡眠期脑电图显示,快速眼动睡眠期(REM)肌肉迟缓障碍,符合快速眼动睡眠期行为障碍(RBD)。临床诊断为很可能MSA⁃P型,左旋多巴治疗无效,于2010年9月行重复经颅磁刺激,刺激频率5 Hz,脉冲次数1000次/d,刺激强度80%静息运动阈值(RMT),间隔时间40 s,每天1次、每周5 d,连续2周。治疗前小指展肌三重刺激技术波幅比为28.30%(图1a),统一多系统萎缩评价量表第二部分(UMSARSⅡ)评分为20分;治疗后即刻、1个月和2个月小指展肌三重刺激技术波幅比分别为58.40%,90.70%和50.70%(图1b~1d),UMSARSⅡ评分分别为16、17和23分。
例2 女性,44岁,因进行性动作迟缓1年余,于2010年3月23日至神经科门诊就诊。患者1年余前无明显诱因逐渐出现行走缓慢,双腿沉重感、抬起费力,进行性加重,行走距离逐渐缩短,伴轻度前倾;此后出现双上肢动作迟缓、笨拙,写字和解纽扣等精细动作迟缓,语言缓慢,生活尚能自理,可以自行上下楼梯、做饭;1个月后出现启动困难,尤以转身或跨越障碍时显著,坐位站起困难;此后1个月偶出现持物时双手颤抖,无静止性震颤,不能翻身,生活不能自理,自觉右侧肢体略沉重;病程中无认知功能障碍。患者近2年出汗减少,怕热;近1年颈部和背部酸痛,尿不尽,曾发生3~4次尿失禁,便秘。既往史、个人史及家族史:贫血30余年(具体不详);28年前(1982年)曾发生一氧化碳中毒,意识障碍,自行缓解,未影响认知功能;1年前出现支气管扩张(具体不详);个人史及家族史无特殊。门诊体格检查:卧位血压90/60 mm Hg、立位60/40 mm Hg,皮肤黏膜苍白;神志清楚,语言缓慢,表情淡漠,脑神经检查未见异常;四肢肌力5级、肌张力增高,深浅感觉对称存在,双手快复轮替动作缓慢,指鼻试验和跟⁃膝⁃胫试验欠稳准;Romberg征可疑阳性,慌张步态,双侧腱反射对称活跃,双侧Hoffman征阳性、Babinski征可疑阳性、Chaddock征阳性,脑膜刺激征呈阴性。简易智能状态检查量表(MMSE)评分30分。实验室检查:血常规血红蛋白113 g/L(110~150 g/L);血清转铁蛋白饱和度(TS)0.18(0.25~0.35),血清铁7.34 μmol/L(12.53 ~ 26.85 μmol/L);血液涂片无异常。头部MRI检查未见异常。肌电图和神经传导速度(NCV)未见异常。肛门括约肌肌电图呈神经源性损害,膀胱残余尿量240 ml。临床诊断为很可能MSA⁃P型,左旋多巴治疗无效,遂于2010年9月行重复经颅磁刺激,刺激频率5 Hz,脉冲次数1000次/d,刺激强度为80%静息运动阈值,间隔时间40 s,每天1次、每周5 d,连续2周。治疗前小指展肌三重刺激技术波幅比为69.10%(图2a)、UMSARSⅡ评分为20分;治疗后即刻小指展肌三重刺激技术波幅比为71.70%(图2b)、UMSARSⅡ评分为12分。由于患者在外地不方便随诊,未能客观评价远期三重刺激技术波幅比和UMSARSⅡ评分。
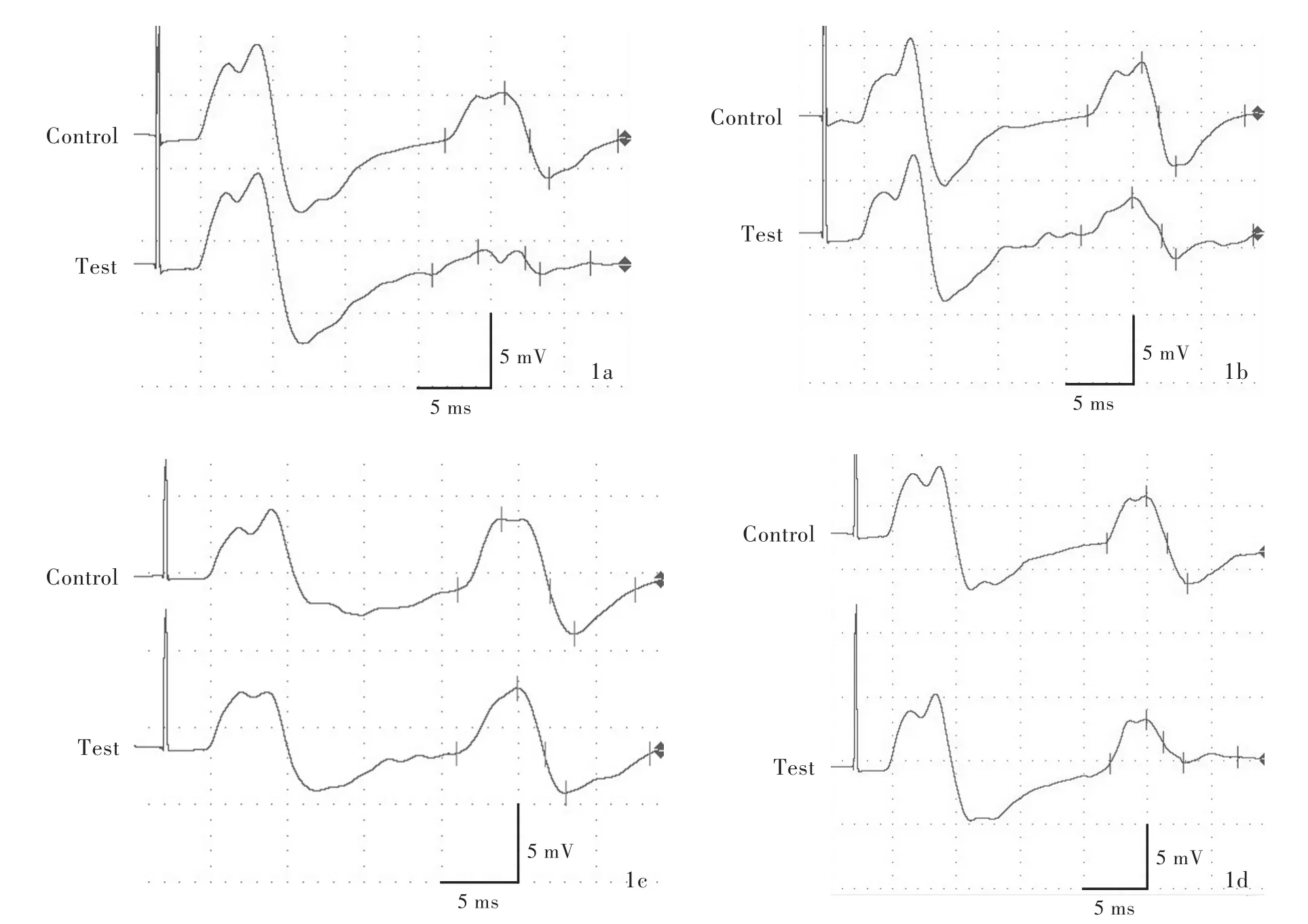
图1 小指展肌三重刺激技术所见 1a 治疗前三重刺激技术波幅比为28.30% 1b 治疗后即刻三重刺激技术波幅比为58.40% 1c 治疗后1个月三重刺激技术波幅比为90.70% 1d 治疗后2个月三重刺激技术波幅比为50.70%Figure 1 TST findings at abductor digiti minimi The TST amplitude ratio before rTMS(Panel 1a),immediately after rTMS(Panel 1b),one month after rTMS(Panel 1c)and 2 months after rTMS(Panel 1d)was 28.30%,58.40%,90.70%and 50.70%,respectively.
讨 论
多系统萎缩是散发性神经变性病,临床表现为帕金森综合征、小脑共济失调和自主神经功能障碍的组合,目前尚无肯定有效的治疗方法。皮质脊髓束损害是多系统萎缩的临床表现之一,约28%患者可见病理征,43%可见腱反射亢进[15]。Eusebio等[6]采用三重刺激技术定量分析MSA⁃P型患者皮质脊髓束损害,结果显示,50%存在皮质脊髓束损害,平均三重刺激技术波幅比为86.60%。我们的既往研究显示,MSA⁃P型患者三重刺激技术波幅比为(40.70±18.60)%[16],表明皮质脊髓束损害常见。
本组2例MSA⁃P型患者均行重复经颅磁刺激治疗,采用三重刺激技术定量评价疗效,结果显示,皮质脊髓束损害明显改善(例1小指展肌三重刺激技术波幅比自28.30%增至90.70%,例2自69.10%增至71.70%),运动功能明显提高(例1 UMSARSⅡ评分自20分降至16分,例2自20分降至12分),表明三重刺激技术波幅比与临床症状具有相关性。既往研究显示,帕金森综合征患者皮质兴奋性主要受基底神经节向皮质流出异常的影响,并非直接累及皮质脊髓束的投射[17]。在本研究中,究竟是由于重复经颅磁刺激对皮质脊髓束的影响逆向改变基底神经节向皮质的流出,还是重复经颅磁刺激通过远隔效应改变基底神经节向皮质的流出,从而达到改善皮质脊髓束的目的,尚待进一步深入研究。此外,在本研究中,我们还观察到重复经颅磁刺激对三重刺激技术波幅比的影响相对持久,治疗后1个月三重刺激技术波幅比仍持续升高,同时伴UMSARSⅡ评分降低,间接提示三重刺激技术波幅比与临床症状之间具有相关性。三重刺激技术波幅比升高趋势于重复经颅磁刺激1个月后发生衰退,可能是由于多系统萎缩持续性进展的特征,同时也为重复经颅磁刺激的治疗周期提供参考依据。
本研究仅是三重刺激技术定量评价重复经颅磁刺激治疗效果的初步探讨,尚待更大样本量的研究加以证实。毋庸置疑的是,对于多系统萎缩这种缺乏有效治疗方法的疾病而言,任何有阳性结果的研究均鼓舞人心,但仍需谨慎求证。
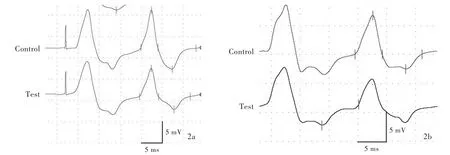
图2 小指展肌三重刺激技术所见 2a 治疗前的三重刺激技术波幅比为69.10% 2b 治疗后即刻的三重刺激技术波幅比为71.70%Figure 2 TST findings at abductor digiti minimi The TST amplitude ratio before rTMS(Panel 2a)and immediately after rTMS(Panel 2b)was 69.10%and 71.70%,respectively.
[1]Magistris MR,Rösler KM,Truffert A,Landis T,Hess CW.A clinical study of motor evoked potentials using a triple stimulation technique.Brain,1999,122:265⁃279.
[2]Groppa S,Oliviero A,Eisen A,Quartarone A,Cohen LG,Mall V,Kaelin⁃Lang A,Mima T,Rossi S,Thickbroom GW,Rossini PM,Ziemann U,Valls ⁃Solé J,Siebner HR.A practical guide to diagnostic transcranial magnetic stimulation:report of an IFCN committee.Clin Neurophysiol,2012,123:858⁃882.
[3]Rosler KM,Truffert A,Hess CW,Magistris MR.Quantification of upper motor neuron loss in amyotrophic lateral sclerosis.Clin Neurophysiol,2000,111:2208⁃2218.
[4]Grapperon AM,Verschueren A,Duclos Y,Confort⁃Gouny S,Soulier E,Loundou AD,Guye M,Cozzone PJ,Pouget J,Ranjeva JP,Attarian S.Association between structural and functional corticospinal involvement in amyotrophic lateral sclerosis assessed by diffusion tensor MRI and triple stimulation technique.Muscle Nerve,2014,49:551⁃557.
[5]Tan F,Wang X,Li HQ,Lu L,Li M,Li JH,Fang M,Meng D,Zheng GQ.A randomized controlled pilot study of the triple stimulation technique in the assessment of electroacupuncture for motor function recovery in patients with acute ischemic stroke.Evid Based Complement Alternat Med,2013:ID431986.
[6]Eusebio A,Azulay JP,Witjas T,Rico A,Attarian S.Assessment of cortico⁃spinal tract impairment in multiple system atrophy using transcranial magnetic stimulation.Clin Neurophysiol,2007,118:815⁃823.
[7]Jang W,Park J,Kim JS,Youn J,Oh E,Jo KD,Lee MK,Kim HT.Triple stimulation technique findings in vascular Parkinsonism and Parkinson's disease.Clin Neurophysiol,2014,125:1834⁃1839.
[8]Pascual⁃Leone A,Valls⁃Solé J,Brasil⁃Neto JP,Cammarota A,Grafman J,Hallett M.Akinesia in Parkinson's disease:Ⅱ.Effects ofsubthreshold repetitive transcranialmotorcortex stimulation.Neurology,1994,44:892⁃898.
[9]Elahi B,Elahi B,Chen R.Effect of transcranial magnetic stimulation on Parkinson motor function:systematic review of controlled clinical trials.Mov Disord,2009,24:357⁃363.
[10]Shirota Y,Ohtsu H,Hamada M,Enomoto H,Ugawa Y;Research Committee on rTMS Treatment of Parkinson's Disease.Supplementary motor area stimulation for Parkinson disease:a randomized controlled study.Neurology,2013,80:1400⁃1405.
[11]Chou YH,You H,Wang H,Zhao YP,Hou B,Chen NK,Feng F.Effect of repetitive transcranial magnetic stimulation on fMRI resting⁃state connectivity in multiple system atrophy.Brain Connect,2015,5:451⁃459.
[12]Magistris MR,Rösler KM,Truffert A,Myers JP.Transcranial stimulation excites virtually all motor neurons supplying the target muscle:a demonstration and a method improving the study of motor evoked potentials.Brain,1998,121:437⁃450.
[13]Roth G,Magistris MR.Identification of motor conduction block despite desynchronisation: a method. Electromyogr Clin Neurophysiol,1989,29:305⁃313.
[14]Gilman S,Wenning GK,Low PA,Brooks DJ,Mathias CJ,Trojanowski JQ,Wood NW,Colosimo C,Dürr A,Fowler CJ,Kaufmann H,Klockgether T,Lees A,Poewe W,Quinn N,Revesz T,Robertson D,Sandroni P,Seppi K,Vidailhet M.Second consensus statement on the diagnosis of multiple system atrophy.Neurology,2008,71:670⁃676.
[15]Köllensperger M,Geser F,Ndayisaba JP,Boesch S,Seppi K,Ostergaard K,DupontE,CardozoA,TolosaE,AbeleM,Klockgether T,Yekhlef F,Tison F,Daniels C,Deuschl G,Coelho M,Sampaio C,Bozi M,Quinn N,Schrag A,Mathias CJ,Fowler C,Nilsson CF,Widner H,Schimke N,Oertel W,Del Sorbo F,Albanese A,Pellecchia MT,Barone P,Djaldetti R,Colosimo C,Meco G,Gonzalez⁃Mandly A,Berciano J,Gurevich T,Giladi N,Galitzky M,Rascol O,Kamm C,Gasser T,Siebert U,Poewe W,Wenning GK;EMSA ⁃SG.Presentation,diagnosis,and management of multiple system atrophy in Europe:final analysis of the European multiple system atrophy registry.Mov Disord,2010,25:2604⁃2612.
[16]Wang H,Wang Y,Cui LY.Electrophysiological characteristics of cortico⁃spinaltractimpairmentin patients with atypical parkinsonism:clinicalvalue of triple stimulation technique.Zhonghua Lao Nian Duo Qi Guan Ji Bing Za Zhi,2015,14:655⁃659[.王含,王悦,崔丽英.不典型帕金森患者皮质脊髓束损害的电生理特点——三重刺激技术研究初探.中华老年多器官疾病杂志,2015,14:655⁃659.]
[17]Kühn AA,Grosse P,Holtz K,Brown P,Meyer BU,Kupsch A.Patterns ofabnormalmotor cortex excitability in atypical parkinsonian syndromes.Clin Neurophysiol,2004,115:1786⁃1795.
2017⁃04⁃06)
The 23rd World Congress of Neurology
Time:September 16-21,2017
Venue:Kyoto,Japan
Website:www.2017.wcn-neurology.com
The 23rd World Congress of Neurology(WCN 2017)will take place in Kyoto,Japan on September 16-21 2017,cohosted by the Japanese Society of Neurology(JSN),Societas Neurologica Japonica,and Asian and Oceanian Association of Neurology(AOAN).The theme of WCN 2017 will be"Defining the Future of Neurology".
Founded originally in 1902,the JSN has evolved into a large society with 8579 members.Initially a combined neurology and psychiatry association,the current JSN separated in 1959 and continued to flourish ever since.It was the 12th WCN meeting held at Kyoto in 1981 that greatly contributed to the development of JSN and AOAN.Therefore,WCN 2017 which is being held at the very same venue would be a very historic meeting which will again serve as a springboard to strongly advance the Asia Initiative of World Federation of Neurology(WFN)for worldwide advancement of neurology in both scientific and clinical aspects,thus"Defining the Future of Neurology".You can participate in very active discussions and cutting⁃edge lectures by the world's top scientists and neurologists including three Nobel laureates as well as hear all the advances of scientific and clinical neurology.Gene therapy and stem/induced pluripotent stem(iPS)cell medicine are such examples on the one hand and brain⁃machine⁃interface,information technology and robotics in care and rehabilitation on the other.Neurology related to environmental and disaster medicine will also attract many neurologists particularly in rapidly developing counties.
The Local Organizing Committee of JSN in close collaboration with the WFN looks forward to welcoming you in Kyoto for WCN 2017.
The 142nd Annual Meeting of American Neurological Association
Time:October 15-17,2017
Venue:San Diego,California,USA
Website:2017.myana.org
Abstract deadline:September 11,2017
The 142nd Annual Meeting of American Neurological Association(ANA2017)will be held on October 15-17,2017 in San Diego,California,USA.ANA2017 offers exceptional education,career development for all levels of academic neurology and networking opportunities with leaders in the field.Scientific symposia cover broad spectrum of subspecialties.Poster sessions are packed with the latest emerging neuroscience and interactive lunch workshops take breakout sessions to the next level.
ANA2017 will feature five main symposia,which highlight groundbreaking conceptual and therapeutic advances in a variety of neurologic disease states,as well as interactive educational sessions designed to both support career development and provide educational opportunities in sub⁃specialties.
Triple stimulation technique to evaluate the curative effect of repetitive transcranial magnetic stimulation in patients with multiple system atrophy:two cases report
WANG Han1,WANG Yue1,CUI Li⁃ying1,2
1Department of Neurology,Peking Union Medical College Hospital,Chinese Academy of Medical Sciences and Peking Union Medical College,Beijing 100730,China
2Neurosciences Center,Chinese Academy of Medical Sciences,Beijing 100730,China
Corresponding author:WANG Han(Email:wanghanpumch@163.com)
BackgroundPrevious studies suggest that the cortico⁃spinal tract can be modulated by M1 repetitive transcranial magnetic stimulation(rTMS).However,it is not well investigated in patients with multiple system atrophy(MSA).We discuss 2 cases of MSA with parkinsonism⁃predominant(MSA⁃P),who have been evaluated the function of cortico⁃spinal tract using triple stimulation technique(TST)before and after rTMS,so as to explore the effect of rTMS on improving the damage of cortico⁃spinal tract.MethodsTwo MSA⁃P patients(one 62⁃year⁃old male,one 44⁃year⁃old female)with disease course of one year were examined with TST at abductor digiti minimi.TST amplitude ratio and the motor score of Unified Multiple System Atrophy Rating Scale(UMSARSⅡ)were used to assess the damage of cortico⁃spinal tract and motor function before and after rTMS treatment.ResultsTST amplitude ratio at abductor drgiti minimi of both patients was 28.30%and 69.10%,and UMSARSⅡscore was 22 and 20 before treatment.Immediately after rTMS the amplitude ratio was 58.40% and 71.70%,and UMSARSⅡscore was 16 and 12,respectively.The improvement sustained in Case one in the next month(TST amplitude ratio 90.70%,UMSARSⅡscore 17)and the second month(TST amplitude ratio 50.70%,UMSARSⅡscore 23).ConclusionsTST can be used to quantitatively evaluate the integrity of cortico⁃spinal tract after rTMS.
Evoked potentials; Multiple system atrophy; Transcranial magnetic stimulation This study was supported by the National Natural Science Foundation of China(No.30800352).
10.3969/j.issn.1672⁃6731.2017.06.008
国家自然科学基金资助项目(项目编号:30800352)
100730中国医学科学院 北京协和医学院 北京协和医院神经科(王含,王悦,崔丽英);100730北京,中国医学科学院神经科学中心(崔丽英)
王含(Email:wanghanpumch@163.com)
