原发性肾上腺淋巴瘤4例临床特点分析并文献复习
2017-11-13时一添袁风红邹耀红
时一添 袁风红 邹耀红
【摘要】 目的:探讨分析原发性肾上腺淋巴瘤(primary adrenal lymphoma)的临床特征、诊断、治疗及预后,提高对该疾病的认识。方法:回顾性分析4例经病理证实的原发性肾上腺淋巴瘤临床特征并复习相关文献。患者均以发热为主要首发症状,CT提示肾上腺占位,依靠穿刺明确诊断。结果:4例均为非霍奇金淋巴瘤,其中1例为T细胞来源,于确诊后1个月死亡,剩余3例为B细胞来源,均予R-CHOP方案化疗,2017年3月随访2例无瘤存活,1例化疗中。结论:原发性肾上腺淋巴瘤临床缺乏特异性表现,通常由CT等影像学检查发现肾上腺肿物,经由穿刺活检病理确诊,大部分为非霍奇金淋巴瘤,多联合化疗为首选治疗方案,病理类型影响疾病预后。
【关键词】 肾上腺; 淋巴瘤; 非霍奇
doi:10.14033/j.cnki.cfmr.2017.18.084 文献标识码 B 文章编号 1674-6805(2017)18-0161-04
Clinical Features Analysis of Four Cases of Primary Adrenal Lymphoma and Review of Literature/SHI Yi-tian,YUAN Feng-hong,ZOU Yao-hong.//Chinese and Foreign Medical Research,2017,15(18):161-164
【Abstract】 Objective:To discuss the clinical features,diagnosis,therapy and prognosis of primary adrenal lymphoma(PAL) in order to enhance the understanding of this disease.Method:The clinical data of 4 patients with pathologically proven as PAL were retrospectively analyzed,considering literatures review.Fever was the first symptom of all 4 patients,occupying lesions in adrenal gland were discovered by computed tomography(CT) and diagnosed by needle biopsy.Result:Pathology revealed all 4 cases had non-Hodgkins lymphoma,1 case was T-cell type,who died within 1 month,the other 3 cases were B cell type,received R-CHOP chemotherapy,all the 3 patients were followed up in March 2017,2 patients were tumor-free survival,1 patient was currently undergoing chemotherapy.Conclusion:PAL has no special clinical manifestations,it is usually discovered by CT imaging findings of adrenal masses,diagnosed by pathological examination though needle biopsy.A majority type of the patients are NHL,the principal treatment is adjuvant combination chemotherapy,pathologic type affects the prognosis of the disease.
【Key words】 Adrenal glands; Lymphoma; Non-Hodgkin
First-authors address:The Affiliated Wuxi Peoples Hospital of Nanjing Medical University,Wuxi 214023,China
目前国内外关于原发性肾上腺淋巴瘤(PAL)的报道少见[1],人们对该疾病的临床症状、病例特点、诊治及预后认识有限,临床上很容易误诊,笔者回顾性分析近年来笔者所在科收治的4例原发性肾上腺淋巴瘤患者,并综合文献复习以提高对该疾病的认识。
1 病例介紹
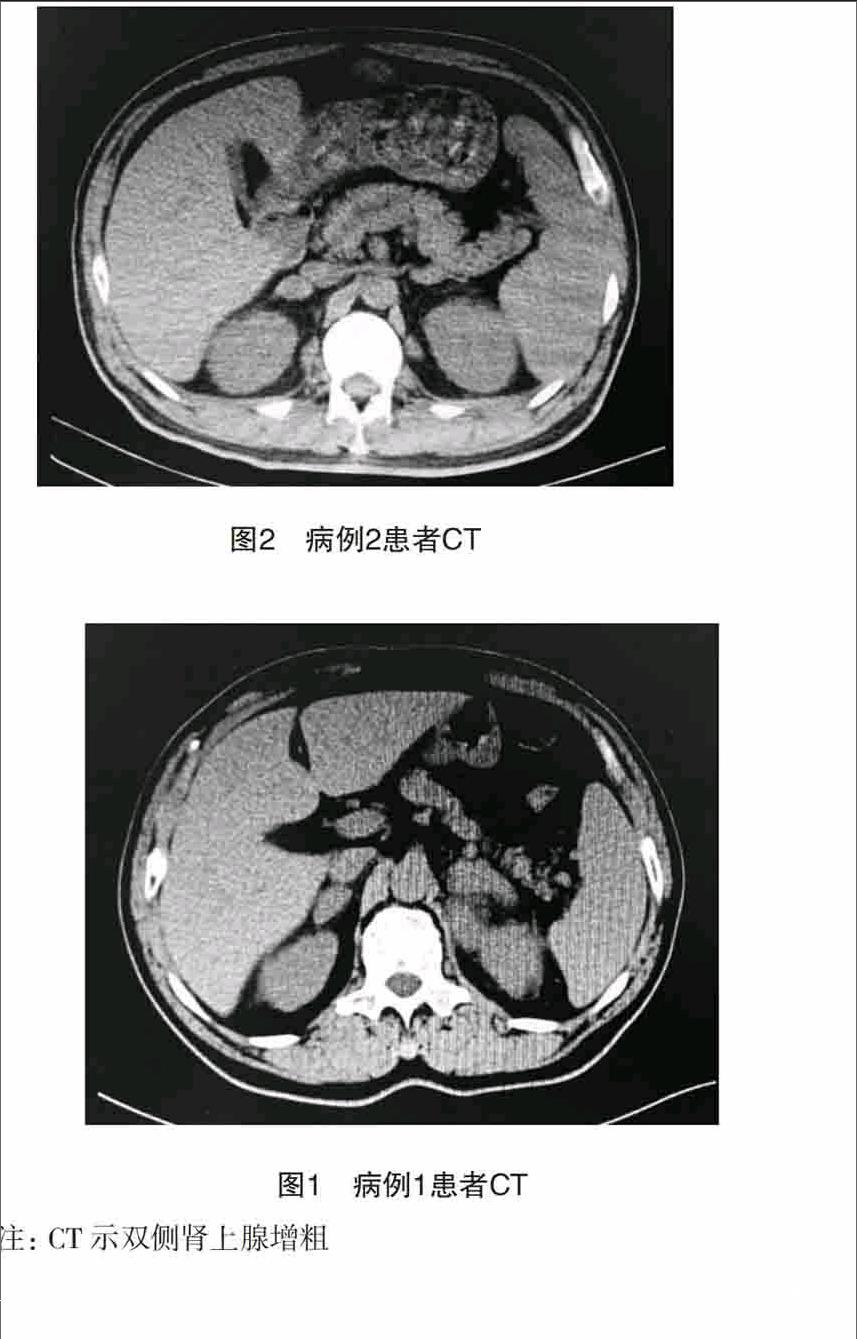
病例1:男,62岁,因“反复发热1个月”于2015年1月6日收治笔者所在科,外院体温最高39.2 ℃,多于下午出现,夜间达到发热高峰,无特殊阳性症状,院外予哌拉西林舒巴坦、左氧氟沙星抗感染治疗无效,查体无阳性体征,入院后查胸部+腹部CT示双侧肾上腺块团影,左侧较大,大小约66 mm×35 mm,增强后轻中度强化(图1),纵隔及后腹膜未见肿大淋巴结;浅表彩超未见肿大淋巴结;骨穿:感染性髓像;血常规:WBC 2.85×109/L,Hb 110 g/L,血小板63×109/L,CRP 9 mg/L,血沉15 mm/h,肝肾功能、电解质正常,LDH>21 500 U/L;T-spot.TB阳性,A孔74,B孔40;查皮质醇、ACTH、肾素血管紧张素醛固酮、尿香草基苦杏酸(VMA)、性激素等均在正常范围,甲状腺功能:FT3 2.05 pmol/L(3.8~6 pmol/L),FT4、TSH正常;CT引导下肾上腺穿刺活检,病理提示非霍奇金淋巴瘤(T细胞来源),但因患者一般情况持续恶化,未予化疗,于1个月后死亡。endprint
