关节镜下改良Endobutton结合锚钉双重解剖重建技术在肩锁关节脱位治疗中的临床应用
2017-08-01董辉详黄长明范华强李鸿达
董辉详 黄长明 范华强 李鸿达
·论著·
关节镜下改良Endobutton结合锚钉双重解剖重建技术在肩锁关节脱位治疗中的临床应用
董辉详 黄长明 范华强 李鸿达
目的探讨关节镜下改良Endobutton结合锚钉双重解剖重建技术在肩锁关节脱位治疗中的临床应用。方法自2010年6月至2015年6月,厦门大学附属成功医院共收治了32例Ⅲ~Ⅴ型急性肩锁关节脱位患者,其中男22例,女10例;年龄21~60岁,平均28.4岁;其中22例累及主力肩。Rockwood分型Ⅲ型8例,Ⅳ型10例,Ⅴ型14例。所有患者均为急性损伤,即伤后时间≤3周。受伤原因:车祸伤13例,摔倒10例,运动损伤7例,高处坠落伤2例。全部患者均接受关节镜下改良Endobutton结合锚钉双重解剖技术重建喙锁韧带。术后颈腕吊带保护6周,循序行康复锻炼。术后采用美国肩肘外科协会评分(American shoulder and elbow surgeons'form,ASES),视觉模拟评分(visual analogue scale/score,VAS),Constant-Murley评分及肩关节简明测试(simple shouder test,SST),按评定标准评定优、良、一般及差四个等级。结果本组患者术后X线及三维CT重建检查均证实肩锁关节达到解剖复位。所有患者均获得随访,随访时间12~72个月,平均时间24.6个月。ASES评分为97.4分;患者VAS评分<1分;Constant-Murley评分为95.2分;SST问卷的肯定答案平均为11个。所有患者肩关节活动基本恢复正常,平均上举165°,外旋45°。按评定标准评定,优20例,良10例,一般2例,总体优良率达到了93.7%(30/32)。如对侧急性肩锁关节脱位,所有患者均愿意接受同样的手术治疗。所有患者均恢复术前的工作水平,29例(90.6%)恢复到术前运动水平。结论 采用关节镜下改良Endobutton结合锚钉双重解剖重建技术重建喙肩韧带,治疗肩锁关节脱位,具有微创、固定牢固、康复快、美观、满意度高等优点,同时可处理盂肱关节内合并伤,无需取出内固定,临床结果满意,并发症发生率低,是一种治疗急性肩锁关节脱位的较好方法。
肩锁关节;脱位;肩关节镜;Endobutton;锚钉
肩锁关节脱位是一种常见的肩关节损伤,约占肩部损伤的12%[1],占肩关节运动损伤的40%~50%[2-3],多见于青壮年,约70%为直接暴力损伤所致,如肩关节处于外展内旋位时,暴力冲击于肩的顶部或跌倒时肩部着地,均可引起肩锁关节脱位。肩锁关节的稳定主要依靠肩锁关节的关节囊及肩锁韧带、喙锁韧带等静力维持作用,还有三角肌和斜方肌的动力稳定作用。其伤后常导致锁骨外侧端翘起、肩锁关节肿痛及压痛、“琴键征”、肩关节主被动活动受限、力量减弱等症状。
目前临床上肩锁关节脱位多采用Rockwood分型,Ⅰ型:肩锁韧带扭伤,喙锁韧带完整,肩锁关节保持稳定;Ⅱ型:肩锁韧带断裂和喙锁韧带扭伤,常引起半脱位;Ⅲ型:肩锁关节囊及喙锁韧带均完全断裂,喙锁间隙较正常增加25%~100%;Ⅳ型:Ⅲ型伴喙锁韧带从锁骨撕脱,同时伴有锁骨远端向后移位进入或穿出斜方肌;Ⅴ型:Ⅲ型伴锁骨自肩胛骨喙锁间隙垂直方向移位较正常增加100%~300%,锁骨位于皮下;Ⅵ型:Ⅲ型伴锁骨外侧端向下脱位,位于喙突下[4]。目前文献对于Rockwood分型Ⅰ、Ⅱ、Ⅳ、Ⅴ、Ⅵ型肩锁关节损伤的治疗意见比较统一,Ⅰ、Ⅱ型一般采取非手术治疗,早期被动功能锻炼;Ⅳ、Ⅴ、Ⅵ型采取手术治疗,强调喙锁韧带的重建和加强[5]。Ⅲ型损伤有较多争议,有些学者推荐手术治疗,大多数学者建议非手术治疗,如果二期出现症状再行手术处理[6-10]。
文献报道过的肩锁关节脱位的手术治疗方法很多,大部分都取得比较好的临床疗效,各有优缺点[1112],但目前还没有一种手术技术被认为是治疗肩锁关节脱位的金标准。传统手术治疗主要采用切开复位,固定肩锁关节和(或)喙锁关节,或者锁骨外侧端切除结合喙锁韧带重建或喙肩韧带转移等。随着关节镜技术的发展及对肩锁关节重新认识,镜下微创肩锁韧带重建成为治疗肩锁关节脱位的一种新趋势。厦门大学附属成功医院自2010年6月至2015年6月共治疗了32例Ⅲ~Ⅴ型急性肩锁关节脱位患者,采用关节镜下改良Endobutton结合锚钉双重解剖重建技术重建喙锁韧带,取得满意的临床效果,报道如下。
资料与方法
一、一般资料
自2010年6月至2015年6月,本院共收治了32例Ⅲ~Ⅴ型急性肩锁关节脱位患者,其中男22例,女10例;年龄21~60岁,平均28.4岁;其中22例累及主力肩。Rockwood分型Ⅲ型8例,Ⅳ型10例,Ⅴ型14例。所有患者均为急性损伤,即伤后时间≤3周。受伤原因:车祸伤13例,摔倒10例,运动损伤7例,高处坠落伤2例。术前均行X线及三维CT重建检查(图1~2)。均在伤后2周内接受手术治疗,且手术均由同一位高年资医师完成。

图1 术前X线片

图2 术前三维CT重建
二、手术方法
采用全身麻醉,取侧卧位,腋下垫软垫,侧卧挡板固定,患侧上肢外展前屈牵引,头部中立位固定,常规消毒及铺巾。关节镜主要使用4个入路:标准后侧入路,外侧入路,靠近肩峰前角的前入路,前侧入路(图3)。关节镜从后侧入路进入盂肱关节,然后由外向内技术制作位于肩袖间隙外侧的前侧入路,探钩从前侧入路插入,常规检查盂肱关节内病变,如肩袖、关节盂、盂唇、肱骨头、肱二头肌长头腱等,尤其应注意是否有合并上盂唇前后部(superior labral anterior and posterior,SLAP)损伤,根据其损伤情况行清创及修复;从前侧入路插入刨刀和等离子刀,向前上打开肩袖间隙,显露喙突,再制作靠近肩峰前角的前外侧入路,将关节镜镜头移至前外侧入路,清理喙突表面的软组织直至能完全显露喙突的内侧面、下表面及内侧缘;增加肩关节外侧入路,将关节镜镜头移入外侧入路,通过后侧入路清理肩峰下滑囊,再转前外侧入路清理喙突上表面(图4),注意保护喙肩韧带。在锁骨中外1/3处(离肩锁关节内侧约40mm处)切1个25mm长的皮肤切口,预先在锁骨中外1/3处靠后侧(锁骨端锥状韧带止点上表面皮质)用直径4mm钻头开一侧皮质孔,将专用导向器的钩端通过前侧入路后置于喙突基底部下表面(导针入点位于喙突基底部靠内侧),将导向器套筒口卡入孔内并锁紧,调整角度,沿着导向器从锁骨表面经锁骨经喙突钻到喙突基底部下方,撤出导向器,弯钳夹住克氏针喙突下方外露部分,防止移动或退针,沿导针用直径4.0mm空心钻扩孔,将空心钻留着,拔除导针,沿着空心钻将导引线从上向下沿空心钻穿至喙突基底部下方,抓线器从前侧入路伸入喙突底部将导引线拉出,退出空心钻(图5)。复位肩锁关节,测量喙突下方至锁骨表面的长度,选择袢合适长度的Endobutton钢板(一般大于测量长度2~5mm,凑成5mm整数,常用长30mm及35mm),利用导引线将Endobutton钢板引入,使钢板卡于喙突下方,袢穿喙突骨道再穿锁骨骨道至锁骨上表面,在锁骨上表面选择合适宽度的3~4孔微型钢板(手足外科钢板)穿入袢内,通过旋转钢板缩短袢长度使肩锁关节完全复位,钢板两侧钻孔拧入微型螺钉固定。关节镜镜头从外侧入路插入监视,从锁骨上表面的皮肤切口,在锁骨前方离外侧端约20mm处,使用由外到内技术,将1枚锚钉拧入喙突基底部上表面(离喙突骨道中心约10mm,位于其前外侧,图6)。锚钉尾部缝线绕锁骨拉紧打结固定,线结位于锁骨下方。形成改良Endobutton钢板结合锚钉的双重固定(图7~9)。关节镜彻底冲洗及止血后,吸净积水,退出关节镜,逐层缝合伤口,无菌敷料包扎。

图3 关节镜手术入路

图4 显露喙突后的情况

图5 空心钻钻入喙突下

图6 在喙突上表面拧入锚钉

图7 双固定后喙突下表面
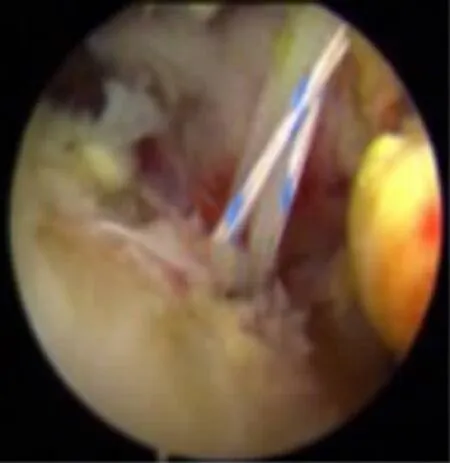
图8 双固定后喙突上表面

图9 双固定后的锁骨上表面
三、术后康复及处理
术后穿颈腕吊带保护6周,术后6周内只行肩关节被动活动:48h内<30°的钟摆活动,1周内<60°,2周内<90°,4周内<120°,4周后行全范围被动上举活动。术后6周行主动上举活动,术后半年避免负重。术后常规复查X线及三维CT重建检查,观察骨道及锚钉、Endobutton位置、肩锁关节复位情况(图10~12),以后每3个月复查1次X线片。

图10 术后X线片

图11 术后三维CT骨透明重建

图12 术后三维CT重建
四、疗效评价
术后采用美国肩肘外科协会(American shoulder and elbow surgeons'form,ASES)评分,视觉模拟评分 (visual analogue scale/score,VAS),Constant-Murley评分及肩关节简明测试 (simple shouder test,SST)进行疗效评价。ASES评分是一个需要换算的百分制系统,基于患者的主观评分,包括疼痛(50%)和生活功能(50%)两部分,满分100分。VAS是疼痛程度的评估方法,0~10分,0分:无痛;≤3分:有轻微的疼痛,患者能忍受;4~6分:患者疼痛并影响睡眠,尚能忍受;7~10分:患者有渐强烈的疼痛,疼痛难忍。Constant-Murley评分是以表格形式评估患者肩关节功能,分为4部分:疼痛(15分)、日常生活活动(20分)、主动活动范围(40分)、肌力(25分)。SST问卷是以问卷形式评估每个患者的肩关节功状态和功能,共11个问题,结果以肯定答案个数表示。临床结果评定标准:优,肩关节没有任何疼痛症状,患肢的应用无任何限制,恢复了正常的运动范围及肌力;良,患者对手术表示满意,仅偶尔感到患肩疼痛但不影响活动或不需要常规服用止疼药物;一般,患肩疼痛影响患者的活动或需要使用镇痛药物;差,患者有持续的肩关节疼痛并影响日常生活或复位完全丧失。肩锁关节复位的维持情况通过临床查体及X线片检查,记录患者的恢复体育运动及体力劳动的能力。
结 果
本组患者术后X线及三维CT重建检查均证实肩锁关节达到解剖复位。所有患者均获得随访,随访时间12~72个月,平均时间24.6个月。ASES评分为97.4分;患者 VAS评分<1 分;Constant-Murley评分为95.2分;SST问卷的肯定答案平均为11个。所有患者肩关节活动基本恢复正常,平均上举165°,外旋45°。按评定标准[11]评定,优20例,良10例,一般2例,总体优良率达到了93.7%(表1)。结果一般的2例患者,其中1例疼痛点在肩锁关节处,考虑是肩锁关节软骨面损伤所致,与没有常规行肩锁关节面清理有关;另1例为早期患者,疼痛点可能与锚钉线结有关,当背有肩带的包时疼痛较明显,后期患者将线结放于锁骨后下方就未再发现此类疼痛。在随后的X线片检查随访中,发现3例肩锁关节小于3mm的复位丢失,复位丢失率约9.3%,其中1例有过外伤史,但3例都没有明显不适症状,其中优2例,良1例,不影响最终的临床结果。本组患者没有感染,没有血管神经损伤,没有并发锁骨或者喙突骨折,没有断袢或丝线断裂,没有丝线或者钢板所致骨溶解等并发症。所有患者在被问及“如果相同的情况发生在您的对侧肩关节上,您是否愿意接受相同的手术?”时,其回答均为肯定。所有患者均恢复术前的工作水平,29例(90.6%)恢复到术前运动水平。
讨 论
一、肩锁关节脱位的手术技术及特点
文献报道过的肩锁关节脱位的固定方式有80多种[12-17],大致可以分为以下4类:第1类为肩锁关节的直接固定或外固定,直接固定常使用克氏针、螺钉、丝线、钢丝等,具有简单、经济等优点,取得一定的临床疗效[18-20]。锁骨钩钢板是肩锁关节经典外固定之一,临床上使用较为广泛。其并发症发生率为10%~12%,主要包括复位丢失、创伤性关节炎、肩峰下撞击综合征和肩峰下骨溶解等[21-24]。其在合并喙突骨折的患者具有明显优势。第2类为喙锁关节内固定或替代同时伴有(或没有)肩锁关节韧带修补或重建,固定物有:空心钉、钢丝、钢缆、筋膜、联合建[11]、半腱肌[25]、丝线、袢钢板[26]、锚钉[27-28]或锁扣带袢双钛板紧缩系统。第3类为锁骨远端切除同时伴有(或没有)肩锁韧带筋膜或丝线修补,或者喙肩韧带转位,主要用于慢性肩锁关节不稳[29-34]。第4类为肌腱动态转位伴有(或没有)锁骨远端切除,如喙突尖移位重建喙锁韧带法[12],属于动力性重建,这种操作损伤大,局部解剖破坏大,容易造成肌皮神经损伤,康复期间不能提供动态稳定,难以维持解剖复位,增大肩锁关节处的活动,造成关节不稳定和关节炎,临床上应用较少。
随着肩关节镜技术的发展,肩锁关节脱位的镜下治疗成为一种趋势。镜下治疗肩锁关节脱位,除了具有微创、恢复快、美观、满意度高等传统关节镜优点,还能有效诊治盂肱关节伴随损伤,同时无需取出内固定等优势。Jensen等[23]在2004年至2009年,比较了56例使用关节镜下双束紧缩系统与切开锁骨钩钢板内固定治疗急性高分度(Rockwood分型Ⅲ~Ⅳ型)的肩锁关节脱位,认为两者临床结果相似,虽然都可观察部分复发的垂直不稳定,但关节镜满意度更高,患者更接受关节镜手术,其优势是能有效诊治盂肱关节伴随损伤,无需取出内固定。
文献报道了多种镜下肩锁关节脱位手术技术,主要包括以下几种:(1)镜下锁骨远端切除喙肩韧带转位至新的锁骨外侧端;(2)镜下喙突基底部植入带线锚钉重建喙肩韧带法;(3)镜下丝线绕过喙突重建喙锁韧带法;(4)镜下利用紧缩系统复位肩锁关节重建喙锁韧带法。第1类方法最大缺点是破坏喙肩弓及移位后喙肩韧带强度不足[27,30-33]。第2类锚钉法主要依靠植入喙突带线锚钉重建代替喙锁韧带。因手术操作或术后功能锻炼不当等原因常可能会发生锚钉固定失败,如锚钉脱出、缝线断裂、锚钉受损等。而丝线在锚钉孔处的断裂、锚钉孔的毁损及丝线的强度差是公认的弱点[27,32]。第3类丝线法,丝线滑动会造成锁骨端前移,导致肩锁关节不配合,造成疼痛或活动障碍、无力等;丝线微动可能导致雨刷效应,导致喙突及锁骨骨质的磨损,甚至引起疼痛。单纯丝线固定强度也令人担忧。第4类镜下利用紧缩系统或Endubotton钢板复位肩锁关节重建喙锁韧带法是目前的热点。主要采用单束和双束的紧缩系统或Endubotton重建喙锁韧带,认为其强度超过正常肩锁韧带,取得满意的临床疗效。其优点是肩锁关节的弹性解剖固定。在保持复位的同时允许锁骨的正常旋转。其并发症有锁骨骨折、喙突骨折、袢断裂、复位丢失等。Endobutton钢板固定和缝合锚固定允许关节微动,符合肩锁关节的解剖特点和生物力学,也符合目前国内外学者倾向于重建喙锁韧带系统这一共识。Endobutton钢板是钛合金材料,生物相容性好,无需二次取出,其环形袢的强度和刚度超过天然韧带。Beitzel等[26]采用Endobutton重建喙锁韧带,认为其强度超过喙肩韧带约40%。缝合锚也是钛合金材料,锚钉完全埋入骨组织内,不会对软组织造成刺激,生物相容性好,无需二次取出。Harris等[27]和Liu等[28]认为缝合锚固定重建喙锁韧带的强度与完整的喙锁韧带相近。本组患者利用Endobutton和锚钉的双重固定治疗肩锁关节脱位,解剖重建喙肩韧带,固定可靠,临床效果满意。

表1 32例急性肩锁关节脱位患者术后评分结果
二、关节镜下改良Endobutton结合锚钉双重解剖重建技术
2010年始,作者采用镜下改良Endobutton结合锚钉双重解剖重建技术治疗肩锁关节脱位,重建后肩锁韧带强度更高、张力分散均匀、微动小及不易切割,临床效果满意,术后无锁骨骨折、喙突骨折、袢断裂及明显的复位丢失等并发症。文献报道的镜下并发症主要包括:喙突及锁骨骨折、复位丢失、固定失效和感染等,且并发症发生率不低。2012年Milewski等[35]报道了一组27例镜下喙锁韧带解剖韧带重建,其中喙突隧道组(10例)有并发症8例(80%):喙突骨折 2 例 (20%),复位丢失 5 例(50%),喙突Endobutton固定失效1例(10%);喙突基底绕线法组(17例)有并发症6例(35%):喙突骨折3例(17%),复位丢失1例(6%),复位丢失合并感染1例(6%),术后粘连性关节炎1例(6%)。2012年至2013年,Clavert等[36]分析了116例关节镜下Endobutton固定重建喙锁韧带治疗肩锁关节脱位病例,无术中并发症,术后并发症25例:11例因内固定失效导致复位丢失,1例喙突骨折,7例粘连性关节炎,2例局部感染,5例内固定物疼痛,并发症发生率为22.4%,影响运动恢复,无并发症的患者术后效果良好。2016年Spencer等[37]比较了急性肩锁关节脱位的解剖重建和非解剖重建术后并发症,X线复位失败及再手术率分成4组:(1)改良的Weaver Dunn法;(2)经喙突及锁骨隧道固定法;(3)环绕喙突锁骨固定法;(4)环绕喙突锁骨法和经骨道Endobutton固定的复合方法。术后X线失败率21.4%(33/154),一半发生在术后6周,其中第4组发生率最低,约4.8%(2/42);再手术率9.7%,第4组再手术率最低。Tang等[38]比较了双Endobutton带袢钢板与带线锚钉结合Endobutton钢板两种喙锁韧带重建技术治疗TossyⅢ型肩锁关节脱位的临床疗效,认为两者疗效相当,但后者无复位丢失及异位骨化病例,操作更简便,手术时间更短,并发症更少。本组病例也没有明显并发症。从上述文献说明采用两种固定方式的组合,能规避或减少上述治疗方法的并发症。
双Endobutton带袢钢板技术,带袢钢板规格有限(长15~45mm),而喙锁间距存在个体差异,在手术过程中有时已将肩锁关节解剖复位,却无法找到与之长度完全匹配的材料。本组锁骨端不使用Endobutton钢板,改为微型钢板,将可选宽度的微型钢板穿入袢内,再利用旋转钢板调整袢长度,可以有效、精确控制袢长度,同时不影响袢强度,避免Endobutton钢板袢长度固定规格的缺陷,可以有效恢复肩锁关节对位。紧缩系统材料能调整长度,但只有4~6组丝线组成,而袢是有纵多的纤维丝线组织,更符合韧带的结构,同时强度也略高于紧缩系统。复位丢失是并发症焦点。Singh等[39]报道了9例使用紧缩系统治疗肩锁关节脱位患者,有7例在平均3.1个月(1~7个月)有渐进的肩锁关节复位丢失,其中3例患者再次手术,考虑可能原因是一种雨刷效应。提醒选择这种手术方式需注意复位丢失这种高发生率并发症。锁骨上微型钢板两端用螺钉固定,能完全避免袢脱出,减少袢隧道内微动,减少雨刷效果,减少断袢可能。微型钢板穿Endobutton上的袢形成环形结构重建锥状韧带,锚钉重建斜方韧带,双重规定,提供了足够的强度,张力分散均匀,固定方式更牢靠,相比丝线结不易出现滑移、松动等,能保证术后肩锁关节的稳定性,无复位丢失的担忧。一些文献报道[40]术后并发异位骨化。本组只使用一组骨隧道,可减少术后异位骨化。并发喙突锁骨骨折的影响因素有隧道大小、数量、分布等。Spiegl等[41]比较直径2.4mm和6mm两种锁骨隧道的肩锁关节脱位喙锁韧带重建方式,显示隧道扩大与强度减弱呈正相关,更大的锁骨骨隧道更容易导致术后锁骨骨折。喙突骨折也与骨隧道分布及数量明显相关。本组病例锁骨上只钻取直径4mm的骨道,锁骨端袢内采用微型钢板固定,它比Endobutton钢板宽大,两端使用螺钉固定,可分散应力,强化薄弱点(骨道),能有效避免锁骨端骨折。本组喙突端采用1组骨隧道及1组锚钉,能有效避免喙突骨折。其原因:(1)通过肩峰下间隙显露喙突上表面后,可直视下监控锚钉植入位置,调整入点与骨隧道的最小距离;(2)锚钉更容易调整植入方向,模仿斜方韧带的张力方向,避免应力叠加;(3)锚钉斜行植入喙突,减少喙突内侧缘骨折的风险;(4)锚钉直径3.5mm,小于骨隧道的最小直径4mm。Salzmann等[42]研究了喙锁韧带的止点,测量喙突基底部的宽度为(14.1±2.9)mm,斜方韧带中心点距离外侧缘距离为(4.4±2.8)mm,锥状韧带中心点距离内侧缘(1.7±0.7)mm,它们中点距离为(10.1±4.2)mm。在相距约10mm两点钻2个直径4.5mm的骨隧道,两孔边缘只剩下5.5mm;斜方韧带骨道边缘距离喙突外侧缘最小距离为(2.8±2.1)mm,锥状韧带骨道边缘距离喙突内侧缘的最小距离为(0.7±0.5)mm。从上述数据表明在狭小的喙突行双隧道重建技术要求高,钻取直径4.5mm双骨隧道将明显降低骨质强度,操作不当容易造成骨折。采用直径3.5mm的锚钉取代一组骨隧道,具有上述优势,操作上简单方便,可准确定位,不易影响喙突强度,避免并发喙突骨折。
三、手术治疗要点及注意事项
(1)合并喙突骨折病例不适合行单纯喙锁韧带重建,术前需常规行三维CT检查排除喙突骨折;(2)采用全身麻醉及低压麻醉,减少出血及保证视野清楚;(3)本组病例均采用侧卧位,术中需注意头部应放于患侧上肢牵引后的中立位,并适当固定,防止臂丛神经牵拉伤;(4)准确建立关节镜入路能事半功倍,推荐四入路技术;(5)术中注意保护臂丛神经及锁骨下动静脉等结构,超过喙突内侧缘的操作需小心谨慎,刨刀方向应始终朝外;(6)肩峰下显露喙突时,喙肩韧带是标志,可沿其走行寻找,同时需注意保护喙肩韧带;(7)清楚掌握斜方和锥状韧带止点及行走,术中清楚显露喙突边缘,防止钻爆;(8)放松牵引,上举肩关节,能更轻松复位肩锁关节;(9)定位器导向时,可先在锁骨锥状韧带锁骨止点上表面钻一侧皮质孔,将导向器套筒卡入孔内,防止钻导针时滑动,便于操作及准确定位;(10)当用空心钻沿导针经锁骨经喙突钻到喙突下表面后,不退出空心钻,解开电钻,拔除导针,沿空心钻送入到导引线,这样可简化穿导引线程序;(11)测量袢长度时注意肩关节是否完全复位,否则容易造成袢过长,一般选择3.0mm或3.5mm,术中利用钢板的宽度及旋转钢板调整喙锁间隙,以达到肩锁关节的最佳复位;(12)考虑既往有较多复位丢失病例,复位肩锁关节时应过度复位1~2mm,为复位丢失预留缓冲空间;(13)一般选择3.5mm金属锚钉,无需预钻,简单方便,锚钉尾线打结打在锁骨下方,防止术后线结较大引起疼痛,可利用钢板孔及螺钉固定锁骨端锚钉尾线的位置。
总之,采用关节镜下改良Endobutton结合锚钉双重解剖重建技术重建喙肩韧带,治疗肩锁关节脱位,具有微创、固定牢固、康复快、美观、满意度高等优点,同时可处理盂肱关节内合并伤,无需取出内固定,临床结果满意,并发症发生率低,是一种治疗急性肩锁关节脱位的较好方法。但目前缺乏这种方法的生物力学测试,与其他喙锁韧带重建方式的生物力学比较有待进一步研究。
[1]Kim AC,Matcuk G,Patel D,et al.Acromioclavicular joint injuries and reconstructions:a review of expected imaging findings and potential complications[J].Emerg Radiol,2012,19(5):399-413.
[2]Kaplan LD,Flanigan DC,Norwig J,et al.Prevalence and variance of shoulder injuries in elite collegiate football players[J].Am J Sports Med,2005,33(8):1142-1146.
[3]Sorrells RB.Acromioclavicular separation--aplea for conservative treatment[J].J Ark Med Soc,1984,81(5):263-266.
[4]Guy DK,Wirth MA,Griffin JL,et al.Reconstruction of chronic and complete dislocations of the acromioclavicular joint[J].Clin Orthop Relat Res,1998,(347):138-149.
[5]Urist R.Complete dislocations of the acromiclavicular joint;the nature of the traumatic lesion and effective methods of treatment with an analysis of forty-one cases[J].J Bone Joint Surg Am,1946,28(4):813-837.
[6]Beitzel K,Mazzocca AD,Bak K,et al.ISAKOS upper extremity committee consensus statement on the need for diversification of the Rockwood classification for acromioclavicular joint injuries[J].Arthroscopy,2014,30(2):271-278.
[7]Vaisman A,Villalón Montenegro IE,Tuca De Diego MJ,et al.A novel radiographic index for the diagnosis of posterior acromioclavicular joint dislocations[J].Am J Sports Med,2014,42(1):112-116.
[8]Cox S.The fate of the acromioclavicular joint in athletic injuries[J].Am J Sports Med,1981,9(1):50-53.
[9]Phillips AM,Smart C,Groom AF.Acromioclavicular dislocation.Conservative or surgical therapy [J].Clin Orthop Relat Res,1998,(353):10-17.
[10]Schlegel F,Burks T, Marcus L,et al.A prospective evaluation of untreated acute gradeⅢacromioclavicular separations[J].Am J Sports Med,2001,29(6):699-703.
[11]姜春岩,朱以明,王满宜,等.联合腱外侧半肌腱反转移位重建喙锁韧带治疗肩锁关节脱位 [J].中华创伤骨科杂志,2005,7(9):803-807.
[12]Bishop JY,Kaeding C.Treatment of the acute traumatic acromioclavicular separation[J].Sports Med Arthrosc,2006,14(4):237-245.
[13]Weaver JK,Dunn HK.Treatment of acromioclavicular injuries,especially complete acromioclavicular separation[J].J Bone Joint Surg Am,1972,54(6):1187-1194.
[14]Bosworth BM.Acromioclavicular dislocation:end-results of screw suspension treatment[J].Ann Surg,1948,127(1):98-111.
[15]Larsen E,Petersen V.Operative treatment of chronicacromioclavicular dislocation[J].Injury,1987,18(1):55-56.
[16]Wang G,Shen H,Zeng S,et al.Arthroscopic treatment of acromioclavicular joint dislocation [J].Chin J Shoulder Elbow,2014,2(3):15-19.
[17]Urist MR.Complete dislocation of the acromioclavicular joint[J].J Bone Joint Surg Am,1963,45(8):1750-1753.
[18]Kienast B,Thietje R,Queitsch C,et al.Mid-term results after operative treatment of rockwood grade Ⅲ-V acromioclavicular joint dislocations with an AC-hook-plate[J].Eur J Med Res,2011,16(2):52-56.
[19]Guttmann D,Paksima E,Zuckerman D.Complications of treatment of complete acromioclavicular joint dislocations[J].Instr Course Lect,2000,49(3):407-413.
[20]Morrison S, Lemos J.Acromioclavicular separation.Reconstruction using synthetic loop augmentation [J].Am J Sports Med,1995,23(1):105-110.
[21]Di Francesco A,Zoccali C,Colafarina O,et al.The use of hook plate in type Ⅲ and Ⅴ acromio-clavicular Rockwood dislocations:clinical and radiological midterm results and MRI evaluation in 42patients[J].Injury,2012,43(2):147-152.
[22]Eschler A,Gradl G,Gierer P,et al.Hook plate fixation for acromioclavicular joint separations restores coracoclavicular distance more accurately than PDS augmentation,however presents with a high rate of acromial osteolysis [J].Arch Orthop Trauma Surg,2012,132(1):33-39.
[23]Jensen G,Katthagen JC,Alvarado LE,et al.Has the arthroscopically assisted reduction of acute AC joint separations with the double tight-rope technique advantages over the clavicular hook plate fixation?[J].Knee Surg Sports Traumatol Arthrosc,2014,22(2):422-430.
[24]Patzer T,Clauss C,Kühne CA,et al.Arthroscopically assisted reduction of acute acromioclavicular joint separations:comparison of clinical and radiological results of single versus double TightRopeTMtechnique [J].Unfallchirurg,2013,116(5):442-450.
[25]Hegazy G,Safwat H,Seddik M,et al.Modified weaver-dunn procedure versus the use of semitendinosus autogenous tendon graft for acromioclavicular joint reconstruction [J].Open Orthop J,2016,10(1):166-178.
[26]Beitzel K,Cote MP,Apostolakos J,et al.Current concepts in the treatment of acromioclavicular joint dislocations [J].Arthroscopy,2013,29(2):387-397.
[27]Harris RI, Wallace AL, Harper GD,et al.Structural properties of the intact and the reconstructed coracoclavicular ligament complex[J].Am J Sports Med,2000,28(1):103-108.
[28]Liu YJ,Cai X,Wang ZG,et al.Arthroscopic assisted bankart repair with bio-absorbable fixation tacks[J].Zhonghua Wai Ke Za Zhi,2005,43(16):1072-1074.
[29]Eskola A,Santavirta S,Viljakka T,et al.The results of operative resection of the lateral end of the clavicle[J].J Bone Joint Surg Am,1996,78(4):584-587.
[30]Weaver JK,Dunn HK.Treatment of acromioclavicular injuries,especially cmplete acromioclavicular separation[J].J Bone Joint Surg Am,1972,54(6):1187-1194.
[31]Moinfar AR,Murthi AM.Anatomy of the pectoralis minor tendon and its use in acromioclavicular joint reconstruction[J].J Shoulder Elbow Surg,2007,16(3):339-346.
[32]Lee TQ,Black AD,Tibone JE,et al.Release of the coracoacromial ligament can lead to glenohumeral laxity:a biomechanical study [J].J Shoulder Elbow Surg,2001,10(1):68-72.
[33]Lafosse L,Baier GP,Leuzinger J.Arthroscopic treatment of acute and chronic acromioclavicular joint dislocation [J].Arthroscopy,2005,21(8):1017.
[34]Hosseini H,Friedmann S,Trger M,et al.Arthroscopic reconstruction of chronic AC joint dislocations by transposition of the coracoacromial ligament augmented by the tight rope device:a technical note[J].Knee Surg Sports Traumatol Arthrosc,2009,17(1):92-97.
[35]Milewski MD,Tompkins M,Giugale JM,et al.Complications related to anatomic reconstruction of the coracoclavicular ligaments[J].Am J Sports Med,2012,40(7):1628-1634.
[36]Clavert P,Meyer A,Boyer P,et al.Complication rates and types of failure after arthroscopic acute acromioclavicular dislocation fixation.Prospective multicenter study of 116cases[J].Orthop Traumatol Surg Res,2015,101(8):S313-S316.
[37]Spencer T,Hsu L,Sodl J,et al.Radiographic failure and rates of re-operation after acromioclavicular joint reconstruction:a comparison of surgical techniques[J].Bone Joint J,2016,98(4):512-518.
[38]Tang H,Gao S,Yin Y,et al.Comparison of effectiveness between two operative techniques of coracoclavicular ligament reconstruction for treatment of tossy type iii acromioclavicular joint dislocation [J].Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi,2015,29(11):1321-1326.
[39]Singh B, Mohanlal P,Bawale R.Early failure of coracoclavicular ligament reconstruction using TightRope system [J].Acta Orthop Belg,2016,82(1):119-123.
[40]Martetschlger F,Saier T,Weigert A,et al.Effect of coracoid drilling for acromioclavicular joint reconstruction techniques on coracoid fracture risk:a biomechanical study [J].Arthroscopy,2016,32(6):982-987.
[41]Spiegl J, Smith D, Euler A, et al.Biomechanical consequences of coracoclavicular reconstruction techniques on clavicle strength[J].Am J Sports Med,2014,42(7):1724-1730.
[42]Salzmann GM,Paul J,Sandmann GH,et al.The coracoidal insertion of the coracoclavicular ligaments:an anatomic study[J].Am J Sports Med,2008,36(12):2392-2397.
Clinical application of arthroscopic Endobutton improvement combined with anchors double anatomy reconstruction in treatment of acromioclavicular joint dislocation
Dong Huixiang,Huang Changming,Fan Huaqiang,Li Hongda.Department of Orthopedics,Successful Affiliated Hospital of Xiamen University,Xiamen 361000,China
Huang Changming,Email:huangchm123@163.com
BackgroundAcromioclavicular(AC)dislocation is a very common shoulder injury that occupies approximately 12%of the shoulder injury and 40%-50%of the shoulder athletic injury.The injury happens mostly in young adults with about 70%caused by the direct damage.For instance,the violence impacted on the top of the shoulder or falling down with the shoulder to the ground can cause the acromioclavicular dislocation when the shoulder joint is in the abduction and rotation.The stability of the acromioclavicular joint relies mainly on the action of static maintenance of acromioclavicular joint capsule,acromioclavicular ligament and beak lock ligament and the dynamic stability of the deltoid muscle and trapezius muscle.The acromioclavicular joint injury often leads tolateral displacement of clavicle,acromioclavicular swelling and tenderness,"Piano Keys Sign",limited shoulder joint movement,weakened strength and other symptoms.Previous literatures have reported many methods for the surgical treatment of acromioclavicular dislocation,but the golden standard for the treatment has not been found.While the traditional treatment mainly uses the incision operation,the reconstruction of the acromioclavicular joint under the microscope becomes a new trend of treatment with the development of the arthroscopic technique and the new understanding of the acromioclavicular joint.In this study,32cases of patients with typeⅢ-Ⅴacute acromioclavicular joint dislocation from June 2010to June 2015in Chenggong hospital of Xiamen university were observed and analyzed for the discussion of the clinical application of arthroscopic Endobutton improvement combined with anchors double anatomy reconstruction in the treatment of acromioclavicular joint dislocation.Methods(1)General data.32patients diagnosed with acute AC dislocation were treated in our department from June 2010to June 2015,which have a mean age of 28.4years (ranging from 21 to 60years).The group includes 22cases of male and 10cases of female,and 22cases involve the main shoulder.There are 8cases of typeⅢ,10cases of typeⅣand 14cases of typeⅤ with radiological evidence of isolated Rockwood type.All of the patients suffered from acute injuries with the time of less than 3weeks after injury.The causes include 13cases of traffic accident,10cases of fall,7cases of sports accident and 2cases of fall from high place.All of the patients had the X-ray and the three-dimensional CT reconstruction before the operation.They
the surgical treatment within 2weeks after injury,and the operations were performed by the same senior doctor.(2)Operative method.The treatment uses the general anesthesia,and patients take the lateral position with cushion pad under otter and the lateral side baffle fixed.The affected upper limb is kept with abduction flexion traction,and the head is fixed with the neutral position.Regular disinfection and paving is used during the surgery.Arthroscopy mainly uses 4approaches:the standard posterior approach,the lateral approach,the anterolateral approach near the anterior horn of the acromion and the anterior approach.Arthroscopic enters into the glenohumeral joint from the posterior approach and subsequentially makes the anterior approach at the lateral margin of the rotator cuff using the outsidein technique.The hook is inserted from the anterior approach to exam the glenohumeral joint lesions such as rotator cuff,glenoid cavity,glenoid labrum,humeral head,biceps brachia tendon and so on.Special attention is required for the occurrence of the combination with the anterior and posterior labrum superior labral anterior and posterior(SLAP)injury,and the corresponding debridement and repair are needed based on the damage condition.The cutter and plasma cutter are inserted from the anterior approach,and the coronoid process is revealed by forwardly opening the shoulder sleeve clearance.Later,the arthroscopy lens is moved to the anterolateral approach made near the anterior horn of acromion,to clean soft tissue on the surface of the coracoid until the medial aspect of the inner side,the lower surface and the inner margin are fully revealed.The lateral approach of the shoulder joint is increased,and the arthroscopy lens are firstly put into the posterior approach to clean up the subacromial bursa and secondly used to clean up the surface of the coracoid from the anterolateral approach.The protection of the coracoacromial ligament is required for special attention during the previous step.A skin incision of about 25mm long is made on the collarbone with a distance of 1/3of the total length toward the far end(about 40mm inside the acromioclavicular joints),and a cortex holes is opened on the back of the collarbone where the skin cut is made(the surface cortex of the conoid ligament of the clavicle)using the drill with the diameter of 4mm.Then,the hook of the special guide is put onto the lower surface of the coracoid through the anterolateral approach(the point located on the inside of the coronoid basal part).The guide sleeve is subsequentially clamped into the hole and locked tightly.With the angle adjustment,a drill is made from the surface of the clavicle to the bottom of the coracoid basal part along the guide.Afterward,the guide is pulled out.The curved pliers are used to clamp the exposed bottom part of Kirschner wire to prevent movement or withdrawal.Then,the hole is expanded along the guide pin using hollow drill with a diameter of 4.0 mm.The guide pin was later pulled out with the hollow drill left inside,and the guide wire was madethrough the hollow drill to the bottom of the coracoid basal part.The hollow drill is not moved out until the pliers reaches to the coracoid basal part from the anterolateral approach and pulls the guide wire out.After the acromioclavicular joint is restored,the length of the clavicle to the coracoid is measured for the selection of the Endobutton steel plate of proper length(generally longer than the measured length by 2-5mm,and the value is round up to multiples of 5mm.The common length includes 30mm and 35mm).The guide wire is used to direct the Endobutton plate through the coronoid bone tunnel and clavicle bone to the supraclavicular surface with the plate locked under the coracoid.Later,a 3-4whole miniature steel plate of appropriate width is selected to penetrate through the loop under the supraclavicular surface (foot surgery plate).The acromioclavicular joint is completely reset by rotating the plate to reduce the length of the loop,and the plate is fixed with both ends drilled and applied with screw.With the monitor of arthroscopy lens inserted from the lateral approach,an incision is made on the surface of the collarbone.Then,an anchor nail is screwed into the coronoid basal part on the front of the clavicle(approximately 20mm from the lateral segment and 10 mm from the bone center of the coracoid,located at the anterior lateral side)using the outside-in technique.The anchor rope on the tail of the anchor nail is fixed around the clavicle,and the knot is below the clavicle.In this way,a double fixation of modified Endobutton plate combined with anchors is formed.After the washing of arthroscope and hemostasis,the accumulated water is cleaned up.The arthroscope is subsequentially pulled out,and the wound is sutured layer by layer and covered with the sterilized dressing.(3)Postoperative recovery and processing.After the operation,the patients wear wrist strap and neck protection and participate in only the following shoulder joint passive activity for 6weeks:<30°pendulum activity within 48hours;<60°within 1week;<90°within 2weeks;<120°within 4weeks;full range passive lifting activities after 4weeks;initiative lifting activity after 6 weeks;avoiding weight within half a year.Regular reviews of X-ray and three-dimensional CT reconstruction are required to track the positions of bone,anchors,and the Endobutton and the rest of the acromioclavicular joint.The review of X-ray should be done every 3months.(4)Therapeutic evaluation.The postoperative therapeutic efficiency is evaluated by the American shoulder and elbow surgeons′form (ASES),the visual analogue scale/score(VAS),the Constant-Murley score and the simple shoulder test(SST).The evaluation criteria of the clinical result:Optimal,the shoulder joint does not have any pain symptoms,and the limb activity does not have any restrictions.The limb returns to the normal range of movement and muscle strength;Good,the patients were satisfied with surgery and only occasionally feel pain.The pain does not affect the activity of shoulder or require regular pain medications;Normal,the pain of patients affects the daily activity or requires the use of analgesic drugs;Poor,patients have persistent shoulder pain that affects daily life,or the reset is completely lost.ResultsThe postoperative X-ray and CT reconstruction confirmed the anatomical repositioning of acromioclavicular joints for the treated group of patients.All patients were followed up for 12-72months with the average time of 24.6months.ASES score is 97.4points;VAS score<1;Constant-Murley score is 95.2points;Average positive answers to SST questionnaire are 11.The shoulder joint activity of all patients basically recovered to normal with the lift of 165°and the rotation of 45°on average.According to evaluation criteria:20cases are optimal;10cases are good;2cases are normal.Overall,the general fine rate reached 93.7%.For the 2patients with normal clinical outcome,one of them has a pain points at the acromioclavicular joints.The damaged cartilage surface of acromioclavicular joint is considered as the reason,which is associated with the failing of regular cleaning up of the acromioclavicular joint surface;another case was an early patient,and the corresponding pain point might be associate with ground anchor line knot.When the patient has a shoulder bag,the pain become more obvious.It is found that the pain disappears as the knot is put below the collarbone for the later patients.During the X-ray follow-up,3cases of acromioclavicular joint reset loss of less than 3mm were found(1case with history of trauma),and the rate of loss of reduction was about 9.3%.However,all cases including 1optimal and 2good have no obvioussymptoms,and the losses of reduction don′t affect the clinical outcome.This group of patients have no infection,no blood vessels injury,no nerve damage,no concurrent clavicle or coracoid process fracture,no broken loops or thread breakage and no complications such as bone dissolution caused by silk or steel.When all patients were asked"if the same happens on another of your shoulders,are you willing to accept the same surgery?"the answers were all positive.All the patients recovered to preoperative working level,and 29patients (90.6%)recovered to preoperative athletic level.ConclusionsThe treatment of acromioclavicular joint dislocation by reconstructing coracoacromial ligament using the Arthroscopic Endobutton improvement combined with anchors double anatomy reconstruction technique has many advantage including minimally invasive,stable fixation,quick recovery,beautiful appearance,high satisfaction and so on.This strategy can treat the injury of glenohumeral joint without the necessity of taking out the internal fixation.The clinical results were satisfactory,and the complication rate is low.Hence,it is a good method to treat the acute acromioclavicular joint dislocation.However,the biomechanical testing of this method and the biomechanical comparison with other methods of the coracoclavicular ligament reconstruction are insufficient and required in the future.
Acromioclavicular joint; Dislocation;Shoulder arthroscopy; Endobutton;Anchor
2016-09-22)
(本文编辑:胡桂英;英文编辑:陈建海、张晓萌、张立佳)
10.3877/cma.j.issn.2095-5790.2017.01.007
361000 厦门大学附属成功医院暨解放军厦门第174医院骨二区
黄长明:Email:huangchm123@163.com
董辉详,黄长明,范华强,等.关节镜下改良Endobutton结合锚钉双重解剖重建技术在肩锁关节脱位治疗中的临床应用[J/CD].中华肩肘外科电子杂志,2017,5(1):36-46.
