冲击波联合肩关节功能训练治疗冈上肌肌腱炎的临床研究
2017-08-01何栩罗小兵李少柏赵琛
何栩 罗小兵 李少柏 赵琛
·论著·
冲击波联合肩关节功能训练治疗冈上肌肌腱炎的临床研究
何栩 罗小兵 李少柏 赵琛
目的探讨冲击波联合肩关节功能训练治疗冈上肌肌腱炎的临床疗效。方法2014年1月至2016年1月,四川省骨科医院运动医学科收治的70例冈上肌肌腱炎患者,随机分为冲击波治疗组(35例)、冲击波联合肩关节功能训练治疗组(35例)。肩关节功能训练由专业治疗师进行指导,训练方案包括肩关节灵活性提高、肩胛胸壁关节和盂肱关节运动控制两部分,共锻炼12周。两组患者治疗前美国肩肘外科协会(American shoulder and elbow surgeons′form,ASES)评分、美国加州大学洛杉矶分校(University of California at Los Angeles,UCLA)评分、视觉模拟评分(visual analogue scale,VAS)差异无统计学意义。观察比较治疗后5周、12周两组患者肩关节功能的恢复情况。结果将两组患者治疗后5周、12周肩关节功能分别同治疗前进行比较,结果显示患者肩关节功能均优于治疗前。治疗后5周,冲击波治疗组ASES评分(t=-7.972,P <0.05)、UCLA评分(t=-13.017,P <0.05)、VAS评分(t=2.095,P <0.05)同治疗前比较差异有统计学意义;冲击波联合肩关节功能训练治疗组 ASES评分(t=-10.296,P <0.05)、UCLA 评分(t=-11.544,P <0.05)、VAS评分(t=12.897,P <0.05)同治疗前比较差异有统计学意义。治疗后12周,冲击波治疗组 ASES评分(t=-10.344,P <0.05)、UCLA评分(t=-14.728,P <0.05)、VAS评分(t=3.161,P<0.05)同治疗前比较差异有统计学意义;冲击波联合肩关节功能训练治疗组ASES评分(t=-16.909,P <0.05)、UCLA评分(t=-16.440,P <0.05)、VAS评分(t=23.085,P <0.05)同治疗前比较差异有统计学意义。将治疗后5周两组评分组间比较,冲击波联合肩关节功能训练治疗组 ASES评分(t=3.709,P <0.05)、UCLA评分(t=3.622,P <0.05)、VAS评分(t=-4.361,P<0.05)均优于冲击波治疗组,差异有统计学意义。治疗后12周两组评分组间比较,冲击波联合肩关节功能训练治疗组 ASES评分(t=2.353,P <0.05)、UCLA评分(t=3.489,P <0.05)、VAS 评分(t=-2.795,P<0.05)同样优于冲击波治疗组,差异有统计学意义。结论冲击波联合肩关节功能训练治疗冈上肌肌腱损伤较单纯冲击波治疗有更好疗效,值得临床推广。
冈上肌肌腱;冲击波;肩关节功能训练
冈上肌肌腱炎是运动爱好者的常见病,易反复发作。上肢过肩运动中,冈上肌肌腱因反复做功而应力积累,或因肱骨头与喙肩弓的挤压撞击而损伤。冈上肌肌腱炎在针对局部病变对症治疗的同时,更应采用功能训练的手段,改善肩关节运动功能,消除损伤发生机制。在工作中针对肩关节运动功能密切相关的肩胛带肌群制定了肩关节功能训练方案,与冲击波联合用于治疗冈上肌肌腱炎,并与单独采用冲击波治疗进行了对比观察,现总结如下。
资料与方法
一、一般资料
2014年1月至2016年1月四川省骨科医院运动医学科收治患者70例,均为游泳、篮球、排球运动爱好者。采用随机数字表法将其随机分为冲击波治疗组(对照组)、冲击波联合肩关节功能训练治疗组(试验组),每组各35例。试验过程中对照组脱落3例,按实际32例统计。两组共67例患者,其中男51例,女16例;优势侧受累55例,非优势侧受累12例。病程时间3~16个月。
二、纳入及排除标准
纳入标准:①均经MRI确诊为冈上肌肌腱损伤患者,仅单侧发病;②未接受过任何规范化的治疗手段;③肩关节被动活动范围正常;④未合并颈椎病;⑤同意参与本研究并签署知情同意书。
排除标准:①冈上肌肌腱撕裂或完全断裂;②Ⅲ型肩峰;③钙化性冈上肌肌腱炎;④伴有粘连性关节囊炎;⑤伴有退化性关节炎。
三、方法
对照组:采用瑞士Storz Medical公司冲击波治疗仪,型号MP100,频率8~10Hz,冲击次数1 000次。治疗部位为患侧冈上肌在肱骨大结节止点及周围痛点,治疗压力以患者耐受力而定,治疗次数为5次,1次/周。
试验组:冲击波治疗同对照组。肩关节功能训练3次/周,共锻炼12周。训练方案包括肩关节灵活性提高、肩胛胸壁关节和盂肱关节运动控制两部分。肩关节功能训练由专业治疗师进行指导,每次具体训练角度、阻力大小依据患者具体情况由治疗师确定。肩关节灵活性提高(肩胛带周围肌群拉伸)包括:胸大肌拉伸、胸小肌拉伸、斜方肌上束拉伸、肩胛提肌拉伸。20s/组,2~3组/次,组间休息1~2min。肩胛胸壁关节和盂肱关节运动控制包括:①斜方肌中束、菱形肌肌力肌力训练:肩胛骨回缩;②斜方肌各束肌力及配合训练(肩肱节律运动模式训练):俯卧跪姿肩屈;③前锯肌肌力训练:膝位推肩俯卧撑;④内、外旋肌群肌力训练;⑤弹力带抗阻。30个/组,3组/次,组间休息1~2min。
四、疗效评价
分别于治疗前和治疗后5周、12周采用美国肩肘外科协会(American shoulder elbow surgeons′form,AESE)评分、美国加州大学洛杉矶分校评分(University of California at Los Angeles,UCLA)、视觉模拟评分(visual analogue scale,VAS)对两组患者肩关节功能进行评价。涵盖肩关节的疼痛、稳定性、生活功能、主动前屈活动度、前屈力量、患者满意度等方面,可综合反映肩关节功能恢复情况。
五、统计学分析
采用SPSS 17.0软件包进行统计学分析。两组间患者不同指标比较采用两独立样本t检验和四格表χ2检验,组内治疗前后不同指标比较采用配对t检验。检验水准α=0.05,P<0.05为差异有统计学意义。
结 果
一、两组患者基线资料比较
两组患者的基线资料比较差异均无统计学意义(P>0.05),见表1。

表1 两组患者基线资料比较
二、两组患者治疗前肩关节功能比较
治疗前两组间患者的ASES评分、UCLA评分、VAS评分差异均无统计学意义(P>0.05),见表2。
表2 两组患者治疗前肩关节功能情况比较(分,±s)
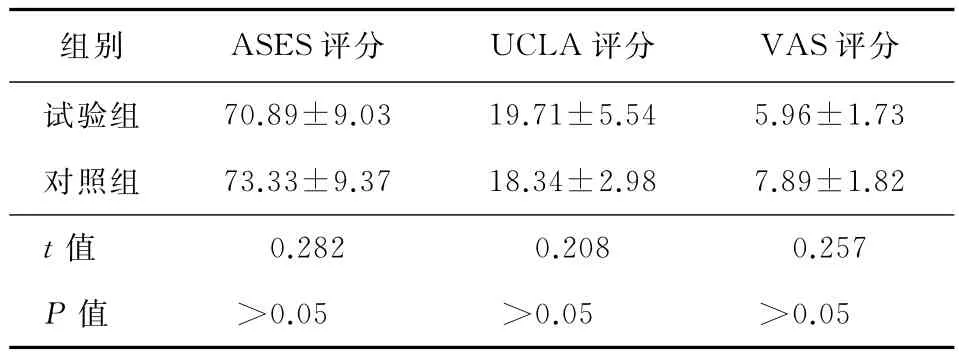
表2 两组患者治疗前肩关节功能情况比较(分,±s)
注:ASES为美国肩肘外科协会;UCLA为美国加州大学洛杉矶分校;VAS为视觉模拟评分
组别 ASES评分 UCLA评分 VAS评分试 验 组 70.89±9.03 19.71±5.54 5.96±1.73对 照 组 73.33±9.37 18.34±2.98 7.89±1.82t值 0.282 0.208 0.257P值 >0.05 >0.05 >0.05
三、两组患者治疗前后功能恢复情况
将两组患者治疗后5周、12周肩关节功能分别同治疗前进行比较,结果显示两组患者肩关节功能持续好转,且同治疗前比较ASES评分、UCLA评分、VAS评分差异均有统计学意义(P<0.05),见表3~4。
表3 两组患者治疗前与治疗后5周的肩关节功能比较(分,±s)
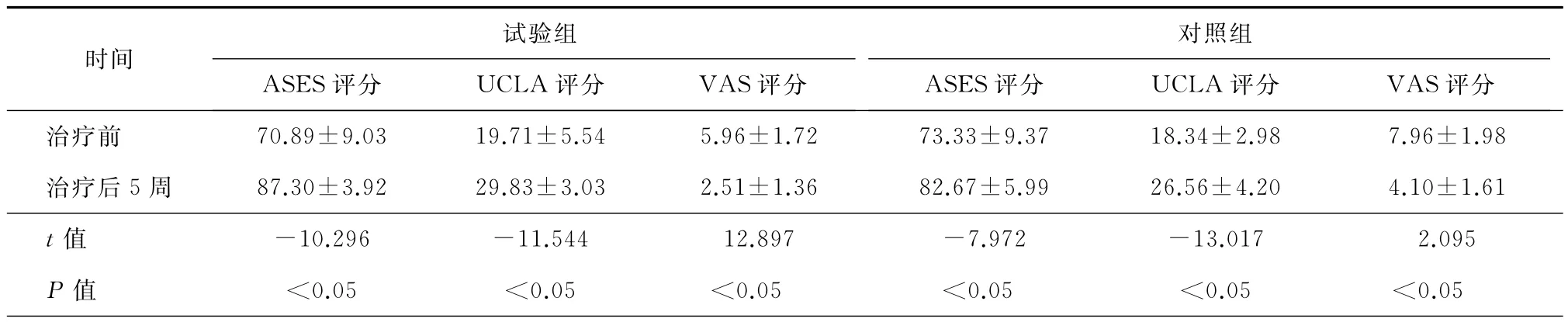
表3 两组患者治疗前与治疗后5周的肩关节功能比较(分,±s)
注:ASES为美国肩肘外科协会;UCLA为美国加州大学洛杉矶分校;VAS为视觉模拟评分
试验组对照组时间ASES评分 UCLA评分 VAS评分ASES评分 UCLA评分 VAS评分治 疗 前 70.89±9.03 19.71±5.54 5.96±1.72 73.33±9.37 18.34±2.98 7.96±1.98治 疗 后 5 周 87.30±3.92 29.83±3.03 2.51±1.36 82.67±5.99 26.56±4.20 4.10±1.61t值 -10.296 -11.544 12.897 -7.972 -13.017 2.095P值 <0.05 <0.05 <0.05 <0.05 <0.05 <0.05
表4 两组患者治疗前与治疗后12周的肩关节功能比较(分,±s)

表4 两组患者治疗前与治疗后12周的肩关节功能比较(分,±s)
注:ASES为美国肩肘外科协会;UCLA为美国加州大学洛杉矶分校;VAS为视觉模拟评分
试验组对照组时间ASES评分 UCLA评分 VAS评分ASES评分 UCLA评分 VAS评分治 疗 前 70.89±9.03 19.71±5.54 5.96±1.72 73.33±9.37 18.34±2.98 7.89±1.82治 疗 后 12 周 91.87±5.75 32.34±2.04 1.28±1.17 88.02±7.57 29.38±4.40 2.20±1.50t值 -16.909 -16.440 23.085 -10.344 -14.728 3.161P值 <0.05 <0.05 <0.05 <0.05 <0.05 <0.05
四、两组患者治疗后功能恢复情况组间对比
试验组治疗后5周和12周的ASES评分、UCLA评分、VAS评分均优于对照组,差异有统计学意义,见表5。单纯冲击波治疗组12周内复发2例,复发率比较差异无统计学意义。
表5 两组患者治疗后5周、12周的肩关节功能比较(分,±s)
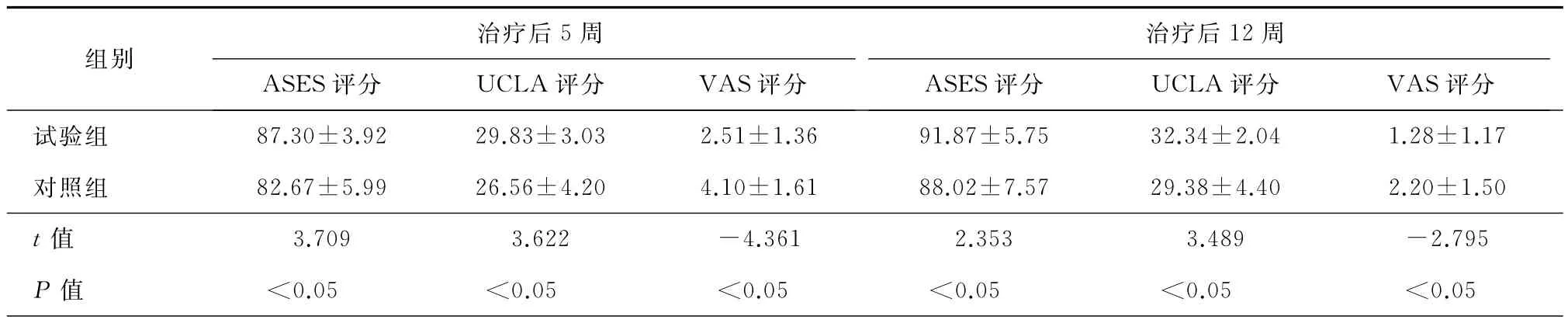
表5 两组患者治疗后5周、12周的肩关节功能比较(分,±s)
注:ASES为美国肩肘外科协会;UCLA为美国加州大学洛杉矶分校;VAS为视觉模拟评分
治疗后5周治疗后12周组别ASES评分 UCLA评分 VAS评分ASES评分 UCLA评分 VAS评分试 验 组 87.30±3.92 29.83±3.03 2.51±1.36 91.87±5.75 32.34±2.04 1.28±1.17对 照 组 82.67±5.99 26.56±4.20 4.10±1.61 88.02±7.57 29.38±4.40 2.20±1.50t值 3.709 3.622 -4.361 2.353 3.489 -2.795P值 <0.05 <0.05 <0.05 <0.05 <0.05 <0.05
讨 论
肩袖损伤是肌腱损伤中最为常见的类型[1],其中又以冈上肌肌腱损伤最为多发[2]。冈上肌是上肢外展的主要动力肌,其肌腱在靠近肱骨大结节近1~1.5cm 处有一乏血管区[3-4],且又穿行于肱骨头与喙肩弓之间,在上肢过顶运动中易受到撞击、挤压。这些结构与功能上的特点是冈上肌肌腱易于损伤的原因。
冲击波是通过电液压效应、电磁效应、压电效应等物理效应产生的一种能透过人体组织的声波[5],目前研究报道,冲击波治疗冈上肌肌腱炎疗效确切[67]。可能的治疗机制是冲击波可以通过改善局部血氧灌注,改变炎性反应过程,调节转化生长因子b1(transforming growth factor-b1,TGF-b1)基 因表达,使胶原蛋白合成,重塑腱性结构[8-9]。本研究中,冲击波对冈上肌肌腱炎的治疗作用也得到证实。
然而,在游泳、篮球、排球等上肢过顶运动人群,冈上肌肌腱炎患者病程较长,且病情易反复。针对这一特殊人群,局部治疗的同时,更应加强局部运动功能,解除冈上肌肌腱在运动中被撞击挤压的机制。
和冈上肌肌腱损伤密切相关的是上肢外展运动,由盂肱关节、肩胛胸壁关节、肩锁关节、胸锁关节共同组成的肩复合体协同运动完成[10]。其中主要由盂肱关节的外展与肩胛骨的上回旋构成,二者遵循2∶1角度的肩肱节律[10]。
良好的外展运动功能首先需要肩胛带周围肌群良好的柔韧性。紧张的肩胛带肌群不仅使肩胛骨运动起始位置不佳(如过于紧张的胸小肌会使肩胛骨前倾内旋,增大肱骨头、肩峰撞击的可能),在运动中也会因肌力、肌张力的不平衡影响运动轨迹。其次,需要肩复合体协同运动的平衡、稳定力量。主要涉及两方面:第一是盂肱关节肱骨头的稳定力量。旋转肌群中的肩胛下肌、冈下肌、小圆肌在肱骨外展时提供使肱骨向下的力,综合三角肌、冈上肌使肱骨头向上的力,防止肱骨头向上撞击喙肩弓,挤压冈上肌腱[2]。冈下肌与小圆肌同时还使肱骨外旋,增大大结节与肩峰之间的间隙[10]。第二是肩胛胸壁关节肩胛骨上回旋运动中保持稳定运动轨迹的力。近年研究认为,肩胛骨运动在肩关节功能中处于核心地位,并提出了肩胛运动功能障碍或肩胛胸壁关节紊乱的概念,认为和肩撞击征、肩袖损伤、肩盂唇损伤、肩锁损伤等肩关节损伤密切相关[11-12]。肩胛骨周围肌肉构建了肩胛胸壁关节的稳定性[13],保证肩胛骨的运动功能不能只单独考虑肩关节某一肌肉的绝对肌力不足[14],应从整体关注针对肩胛带肌群平衡的训练,并结合功能状态进行。导致肩胛骨上回旋运动中稳定性不足的重要原因除菱形肌、斜方肌中下束的力量相对力量不足外,斜方肌上束通常过度活跃,斜方肌中下束、前锯肌激活不足是重要因素[15]。制定功能训练方案应综合兼顾以下几个要点:一是斜方肌上束最小程度的刺激下最大化地激活前锯肌和斜方肌中下束。站立位的训练会增加斜方肌上束的激活,故选择俯卧位下的肩关节功能训练。二是前锯肌的激活一直是实际工作中的难点,可参考现有研究成果,标准推肩俯卧撑较站立位、膝位推肩俯卧撑更能激活前锯肌[16-17],但对受训者力量要求较高,故本研究还是采用膝位推肩俯卧撑。三是肩胛骨面上肢外展(拇指向上),这是唯一能激活中斜方肌达到最大主动收缩力量20%以上的训练[17]。
基于以上要点,制定的肩关节功能训练方案综合兼顾肩关节灵活性提高和肩胛胸壁关节、盂肱关节运动控制,在联合冲击波治疗冈上肌肌腱炎的研究中取得良好疗效。目前,在肩袖损伤、肩盂唇损伤、甚至颈椎病等与肩关节功能密切联系的疾病治疗中,肩关节的功能恢复越来越受到重视,但临床实际工作中,肩关节功能训练的方案制定是难点,望本文的探索尝试可供同行参考借鉴。
[1]Schaer M,Schober M,Berger S,et al.Biologically based strategies to augment rotator cuff tears[J].Int J Shoulder Surg,2012,6(2):51-60.
[2]Johnso DH,Fedowitz RA.实用骨科运动医学 [M].陈世益,王予彬,李国平,译.北京:人民军医出版社,2008:127-163.
[3]Determe D,Rongieres M,Kany J,et al.Anatomic study of the tendinous rotator cuff of the shoulder[J].Surg Radiol Anat,1996,18(3):195-200.
[4]孙常太,黄公怡.肩袖撕裂的病因探讨 [J].中华骨科杂志,1996,16(9):562-563.
[5]燕铁斌,常华.体外冲击波在骨关节疾患中的应用 [J].中华物理医学与康复杂志,2002,24(11):699-700.
[6]谷玉静,林松,冯晓东.体外冲击波治疗非钙化性冈上肌肌腱炎疗效观察 [J].中国骨与关节杂志,2014,3(9):657-660.
[7]戈允申,陈世益,李云霞.体外冲击波治疗肩关节肌腱软组织损伤35例报道 [J].中国运动医学杂志,2011,30(11):1026-1029.
[8]Chao YH,Tsuang YH,Sun JS,et al.Effects of shock waves on tenocyte proliferation and extracellular matrix metabolism[J].Ultrasound Med Biol,2008,34(5):841-852.
[9]Notarnicola A,Moretti L,Tafuri S,et al.Reduced local perfusion after shock wave treatment of rotator cuff tendinopathy[J].Ultrasound Med Biol,2011,37(3):417-425.
[10]Neumann,DA.骨骼肌肉功能解剖学 [M].刘颖,师玉涛,闫琪,译.2版,北京:人民军医出版社,2008:153-168.
[11]Kibler WB,Sciascia A,Wilkes T.Scapular dyskinesis and its relation to shoulder injury [J].J Am Acad Orthop Surg,2012,20(6):364-372.
[12]Cools A,Witvrouw E,Declercq G,et al.Evaluation of isokinetic force production and associated muscle activity in the scapular rotators during aprotraction-retraction movement in overhead athletes with impingement symptoms[J].Br J Sports Med,2004,38(1):64-68.
[13]谭洪波,蔡第心,丁晶,等.肩胛骨弹响综合征治疗进展及个案报道 [J/CD].中华肩肘外科电子杂志,2014,2(4):251-254.
[14]Sahrman S.Diagnosis and treatment of movement impairment syndromes[M].St Louis:Mosby,2002.
[15]Cools AM,Dewitte V,Lanszweert FA,et al.Rehabilitation of scapular muscle balance-Which exercises to prescribe?[J].Am J Sports Med,2007,35(10):1744-1751.
[16]Ludewig PM,Cook TM.Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement[J].Phys Ther,2000,80(3):276-291.
[17]皮尚伯.肩胛部肌肉力量的平衡对肩关节功能康复的影响[J].中国康复医学杂志,2013,28(8):782-784.
Research on the clinical effect of combination treatment of extracorporeal shock wave therapy and shoulder joint function training on the supraspinatus tendinitis
He Xu,Luo Xiaobing,Li Shaobai,Zhao Chen.Department of Sports Medicine,Sichuan Provincial Orthopedic Hospital,Chengdu 610041,China
He Xu,Email:1563330129@qq.com
BackgroundSupraspinatus tendinitis is a common disease in sports enthusiasts withrepeated attacks.In the upper limb movements above the shoulder,the supraspinatus tendon injury was accumulated by repeated work,or because of the impact of the humeral head and the coracoacromial arch.While treating the local lesions,rehabilitations should be introduced to improve shoulder joint function and reduce the mechanism of injury.We made training plans of shoulder girdlemuscles closely related to shoulder joint activities and thus explore the clinical effect of the combination treatment of extracorporeal shock wave therapy and shoulder joint function training on the supraspinatus tendinitis.Methods70Patients who have the supraspinatus tendinitis were randomly divided into two groups:The first group(35patients)was given the extracorporeal shock wave therapy;the second group(35patients)was given the extracorporeal shock wave therapy in combined with the shoulder joint function training.The shoulder joint function training was instructed by professional therapists,which includesthe improvement of the flexibility of shoulder joints and the motion control ability of the scapulothoracu and the glenohumeral joints.The training period lasted for 12weeks.Before the treatment process,the difference of the shoulder joint function between the patients in two groups showed no statistical significant according to the rating scale of the American shoulder and elbow surgeons′form (SAES),the rating scale of university of California at Los Angeles(UCLA)and the visual analogue scale(VAS).The recuperations of patients′shoulder joint function were observed and compared 5weeks and 12weeks after the treatment separately.Results The patients′shoulder joint function 5weeks and 12weeks after the treatment receives a better evaluation than the function before the treatment.Five weeks later,the ASES(t=-7.972,P <0.05),UCLA (t=-13.017,P <0.05)and VAS(t=2.095,P <0.05)of the patients who
extracorporeal shock wave therapy differ from those of the patients before the treatment with a statistical significance;the ASES(t=-10.296,P <0.05),UCLA(t=-11.544,P <0.05)and VAS(t=12.897,P <0.05)of the patients who received 5weeks of combination treatment also differ from those of the patients before the treatment with a statistical significance 12weeks later,the ASES(t=-10.344,P <0.05),UCLA (t =-14.728,P <0.05)and VAS(t =3.161,P <0.05)of the patients who received extracorporeal shock wave therapy differ from those of the patients before the treatment with a statistical significance;the ASES(t=-16.909,P <0.05),UCLA(t=-16.440,P <0.05)and VAS(t=23.085,P <0.05)of the patients who received 12weeks of combination treatment also differ from those of the patients before the treatment with a statistical significance when the rating scores of the two groups received five weeks of different frames of treatment are compared,it is found that the ASES(t=3.709,P <0.05),UCLA (t=3.622,P <0.05)and VAS (t=-4.361,P <0.05)of the group with the combination treatment of extracorporeal shock wave therapy and shoulder joint function training are all superior to those of the group with only the extracorporeal shock wave therapy.Moreover,the differences in between are statistical significant.Similarly,the ASES(t=2.353,P <0.05),UCLA (t=3.489,P <0.05)and VAS(t=-2.795,P <0.05)of the group with 12weeks of combination treatment are also superior to those of the group with 12 weeks of single treatment of extracorporeal shock wave therapy,and the differences are statistical significant.ConclusionsThe supraspinatus tendinitis is one type of common disease among sport amateurs with easily repeated attacks.During the movements of the upper limb over the shoulder joint,the supraspinatus may get injured for two reasons:repeated acting behaviors triggered accumulation of the taken force and the squeeze or crash between humeral head and coracoacromial arch.At the same time of providing correspond treatment to the affected part of the patients with the supraspinatus tendinitis,physician should also use function training to improve their function of the shoulder joint and to eliminate their injury attacks mechanism.The function training improves the flexibility of the shoulder joints and the motion control ability of the scapulothoracu and the glenohumeral joints,which eliminates the squeeze and crash when the supraspinatus is in the movement.The injury of supraspinatus muscle is closely related to the outstretch movements of the upper limb,a type of complex movement cooperated by the glenohumeral joint,the scapulothoracu,the acromioclavicular joint and the sternoclavicular joint.Good outstretch movements should include the following specific characteristics:First of all,themuscle group surround the shoulder trap should have high flexibility.The tightened shoulder trap muscle will not only lead to a worse starting position of the scapula movement but also affect the movement trail due to the imbalance between muscle strength and muscle tone.Secondly,agood outstretch movement needs good balance and stable forcesin the shoulder complex cooperation movement with respect to two aspects.The first force is a stable force in glenohumeral joint humeral head provided by the cooperation movement among subscapularis,infraspinatus,and teres minor in the rotator cuff muscle.The second force is the one that helps to keep a stable movement trail during the scapula upward rotation.This force requires high muscle strength in rhomboids,middle and lower trapezius and serratus anterior muscle.To sum up,based on the points discussed above,the shoulder joint function training plan helps to reach the purpose of treatment by improving the flexibility of shoulder joints and the motion control ability of the scapulothoracu and the glenohumeral joints to eliminate the squeeze and crash mechanism when the supraspinatus is in the movement.The combination treatment of extracorporeal shock wave therapy and shoulder function training on the supraspinatus tendinitis deserves clinical promotion due to its better clinical effect.
Supraspinatus tendinitis;Shock wave;Shoulder joint function training
2016-10-10)
(本文编辑:胡桂英;英文编辑:陈建海、张晓萌、张立佳)
10.3877/cma.j.issn.2095-5790.2017.01.003
四川省科技厅科技支撑项目(2015SZ0055)
610041 成都,四川省骨科医院运动医学科
何栩,Email:1563330129@qq.com
何栩,罗小兵,李少柏,等.冲击波联合肩关节功能训练治疗冈上肌肌腱炎的临床研究 [J/CD].中华肩肘外科电子杂志,2017,5(1):9-14.
