慢性前列腺炎及多灶型HGPIN患者再次穿刺时发展为前列腺癌风险的研究
2017-07-05李洁冰张艳华杨洪艳
李洁冰 张艳华 杨洪艳 张 翠 李 博 程 文
·临床研究·
慢性前列腺炎及多灶型HGPIN患者再次穿刺时发展为前列腺癌风险的研究
李洁冰 张艳华 杨洪艳 张 翠 李 博 程 文
目的 探讨伴有慢性前列腺炎及多灶型高级别前列腺上皮内瘤(Widespread high grade prostatic intraepithelial neoplasia,wHGPIN)患者再次活检,发展为前列腺癌风险的研究。方法 2006年7月—2014年12月收集前列腺再次穿刺活检者172例,均为初次活检病理诊断为HGPIN者,穿刺为经直肠超声引导下前列腺12点穿刺法。再次穿刺均是在初次穿刺6个月后进行的。多灶型HGPIN界定为在前列腺活检中有2针及以上检出高级别前列腺上皮内瘤,孤立型HGPIN界定为在前列腺活检中有1针检出高级别前列腺上皮内瘤。结果 初次活检172例HGPIN患者,孤立型HGPIN 102例,伴有慢性前列腺炎患者17例;多灶型HGPIN 70例,伴有慢性前列腺炎患者54例;172例HGPIN患者再次活检病理为前列腺腺癌者48例,多灶型HGPIN组检出率52.86%(37/70),孤立型HGPIN组检出率为10.78%(11/102),差异有统计学意义(P<0.001);多灶型HGPIN伴有慢性前列腺炎组前列腺腺癌检出率高于不伴有慢性前列腺炎组,差异有统计学意义(P=0.011)。经Logistic回归模型分析,慢性前列腺炎和多灶型HGPIN是再次活检为前列腺癌的独立风险因素。结论 首次活检为慢性前列腺炎与多灶型HGPIN患者是再次活检为前列腺腺癌的高风险因素,建议超声引导下经直肠前列腺再次活检。
前列腺腺癌;高级别前列腺上皮内瘤;慢性前列腺炎;前列腺穿刺
前列腺癌是欧美国家最常见的男性恶性肿瘤。据统计,2010年美国前列腺癌死亡率居男性肿瘤的第一位,超过肺癌[1],在我国前列腺癌发病率近年呈逐渐上升趋势,根据国家癌症中心最新数据显示,自2008年起,前列腺癌已成为泌尿系统中发病率最高的肿瘤[2]。近年来发现约20%的癌症由慢性炎症引起,其中包括膀胱癌、结肠癌、胃癌等[3]。慢性前列腺炎在前列腺癌形成发展中的作用也成为研究热点,而高级别前列腺上皮内瘤(High grade prostatic intraepithelial neoplasia,HGPIN)作为目前公认的前列腺癌的癌前病变[4-5],受到广泛的关注。对于穿刺活检为HGPIN的患者,其发展成为前列腺癌的潜在风险仍存在争议。本研究回顾性分析172例前列腺HGPIN患者再次穿刺活检资料,探讨慢性前列腺炎与多灶型HGPIN对再次活检为前列腺癌的影响。
1 材料与方法
1.1 一般资料
收集2006年7月—2014年12月间前列腺初次活检为HGPIN患者172例,年龄59~72岁,平均66.3岁。初次活检因血清PSA>4.0 ng/mL、直肠指检阳性(质地坚硬、触及结节)、经直肠前列腺超声或盆腔MRI检查发现异常结节者,6个月后对HGPIN患者行再次穿刺活检,筛选病理诊断、tPSA、fPSA、前列腺超声等临床资料完整者入组,并排除以下情况:(1)患有严重心脑血管疾病及凝血指标异常者;(2)泌尿系统感染者;(3)既往患有前列腺癌病史及前列腺手术史者。穿刺前将穿刺相关事项告知患者家属,签署知情同意书。
根据首次穿刺活检中HGPIN阳性针数,将HGPIN组患者分为孤立型HGPIN(102例),多灶型HGPIN(70例)两组;并将孤立型HGPIN分亚组为伴有慢性前列腺炎和不伴有慢性前列腺炎组;多灶型HGPIN分亚组为伴有慢性前列腺炎和不伴有慢性前列腺炎组;根据再次穿刺后病理结果,将其分为前列腺腺癌、慢性前列腺炎、HGPIN三组。
所有患者穿刺前均行经直肠超声常规前列腺检查,清洁灌肠,使用抗生素预防感染,穿刺均采用经直肠超声引导下前列腺12点穿刺法,患者采取左侧卧位,两腿弯曲,常规消毒铺巾后,局部注射利多卡因麻醉,18G活检针,超声引导下进行穿刺活检,穿刺分别于前列腺右侧和左侧外周带的上、中、下三部位、移行区上、下两部位及前列腺尖部右侧和左侧共十二针,获取标本分别装入标记瓶中,并由一名病理医师诊断。
1.2 统计分析方法
采用 SPSS 16.0统计分析软件,计量数据经正态性检验,以中位数和四分位数表示,组间差异用Mann-WhitneyU检验。计数数据以频数表示,组间差异用χ2检验或连续性校正χ2检验,非条件Logistic回归用于分析再次活检时前列腺癌检出率的影响因素,P<0.05为差异有统计学意义。
2 结果
2.1 临床资料分析
孤立型HGPIN组与多灶型HGPIN组在年龄,前列腺体积,初、再次活检时PSA,初、再次活检时f/tPSA差别无统计学意义;孤立型HGPIN伴有炎症17例(23.94%),多灶型HGPIN伴有炎症54例(76.06%),差别具有统计学意义(P<0.01)(表1)。
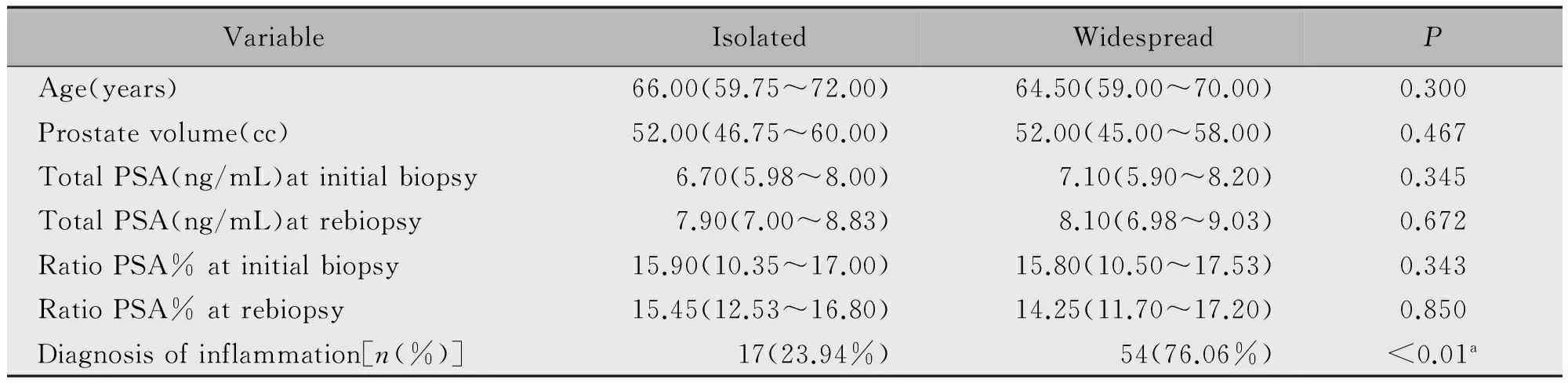
表1 HGPIN患者的临床资料
Note:a.Chi-square tests,others Mann-WhitneyUtest.
2.2 再次活检的病理结果
172例HGPIN患者再次活检的病理类型为HGPIN、慢性前列腺炎、前列腺腺癌(表2)。孤立型HGPIN与多灶型HGPIN两组间前列腺腺癌检出率分别为10.78%(11/102)、52.86%(37/70),差别具有统计学意义(P<0.001);其中孤立型HGPIN组中前列腺腺癌Gleason评分:5例为6分、4例为7分、2例为8分;多灶型HGPIN组中前列腺腺癌Gleason评分:24例为6分、10例为7分、3例为8分。

表2 172例HGPIN患者再次活检的病理类型(n,%)
2.3 慢性前列腺炎与前列腺癌的关系
多灶型HGPIN伴有慢性前列腺炎组与不伴有慢性前列腺炎组再次活检前列腺癌检率差别具有统计学意义(P=0.001),而孤立型HGPIN伴有慢性前列腺炎组与不伴有慢性前列腺炎组差别无统计学意义(P=0.1534)(表3)。经Logistic回归模型分析,首次活检为慢性前列腺炎与多灶型HGPIN患者是前列腺癌的高风险因素,建议慢性前列腺炎与多灶型HGPIN患者应行超声引下前列腺再次活检(表4)。

表3 多灶型HGPIN和孤立型HGPIN两组慢性前列腺炎再次活检病理前列腺癌检出率的关系
Note:Normal.no diagnosis of inflammation.
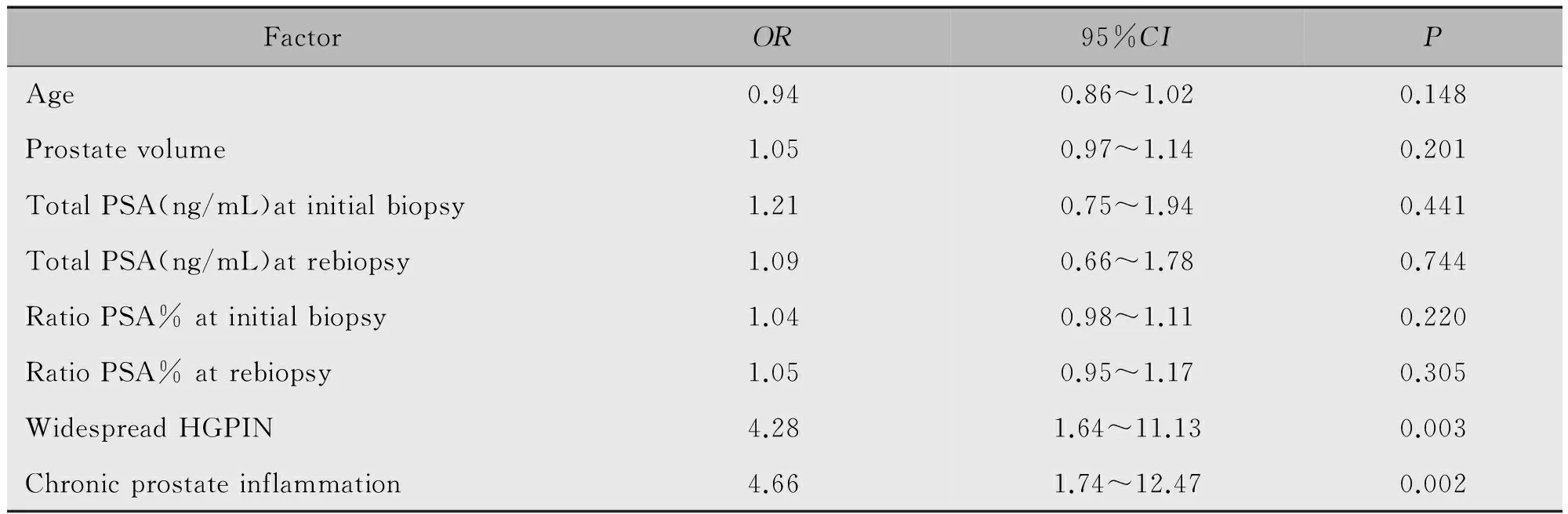
表4 再次活检为前列腺腺癌的多因素分析
3 讨论
目前HGPIN作为前列腺癌的癌前病变受到广泛的关注,以往前列腺6点穿刺法检出的HGPIN,再次活检检出前列腺癌的概率很高,但随着增加初次穿刺活检针数,再次行前列腺穿刺活检出前列腺癌的概率有所下降,对于孤立型HGPIN患者是否进行再次活检提出了质疑[6-7]。10针、12针前列腺穿刺活检方法作为首次前列腺穿刺方案,大大降低了HGPIN发展为前列腺癌的风险[6,8]。然而,有研究显示多灶型HGPIN在再次活检时具有形成前列腺癌的风险[8-10]。欧洲泌尿协会指南指出多灶型HGPIN是再次活检的必要指标[11]。再次穿刺活检HGPIN是其后续监测、治疗过程中的重要环节,正确判断再次穿刺适应症及时间的选择既可以尽早诊断出初次穿刺漏诊的前列腺癌,又可以避免不必要的再次活检损伤。但再次穿刺时间尚无定论,Adamczyk等[12]建议4~6周后行再次穿刺,De Nunzio等[8]认为6个月后行再次前列腺穿刺,在本研究中,采用12针穿刺方法对HGPIN患者6个月后进行再次活检,多灶型HGPIN患者再次穿刺前列腺癌的发病率(52.86%)与孤立型HGPIN组再次穿刺前列腺癌的发病率(10.78%)差异有统计学意义。
对于行12针等扩大穿刺诊断为孤立型HGPIN的患者,在后续诊断方面,可以定期进行PSA水平、直肠指检、经直肠前列腺超声等检查进行随诊,对多灶型HGPIN应行再次活检,这样既可以减少不必要的穿刺造成的损伤,也可以尽量避免前列腺癌的漏诊,为治疗提供可靠的依据。
慢性炎症作为一种恶性肿瘤的风险因素一直是研究的热点,炎症介质通过对细胞及基因的损害,促使血管再生及组织修复[13],使宿主编码癌基因蛋白质并具有抵制感染的能力[14]。Putzi等[15]研究表明,在HGPIN形成过程中,慢性炎症引起的增生、萎缩起到不可或缺的作用。McLennan等[16]提出炎症与HGPIN之间有密切关联,推测这可能是由于细胞和生长因子内出现一种氧化剂,导致了细胞DNA的基因改变。Sfanos等[17]研究慢性前列腺炎可能通过增生、炎性萎缩和HGPIN等组织学病变,在前列腺癌发生发展过程中发挥潜在作用。在本研究中,伴有慢性前列腺炎的多灶型HGPIN组再次穿刺前列腺癌的检出率(61.11%)与不伴有慢性前列腺炎的多灶型HGPIN组再次穿刺前列腺癌的检出率(25.00%)相比差异有统计学意义。经Logistic回归模型分析,本研究证实多灶型HGPIN和慢性前列腺炎是前列腺癌独立的风险因素。
本研究还发现HGPIN患者中再次穿刺诊断为前列腺癌的患者,Gleason评分6~7分43例,Gl-eason评分8分5例。De Nunzio等[8]研究发现HGPIN在第2次穿刺活检证实为前列腺癌的22例中,21例Gleason评分为6~7分,1例为8分,与本研究结果相似。出现Gleason评分8分5例,考虑初次活检HGPIN的患者中,可能已有部分患者发展成为前列腺癌,但穿刺未发现,发生初次穿刺漏诊前列腺癌的概率,建议初次活检方案需进行个性化穿刺,以避免漏诊,这也是本研究的局限性,另外本研究穿刺活检结果未能与大体标本病理检查结果进行对照,可能存在假阴性。
综上所述,本研究中多灶型HGPIN发展成为前列腺癌的概率远高于孤立型HGPIN,同时伴有慢性前列腺炎多灶型HGPIN发展为前列腺癌的概率也高于不伴有慢性前列腺炎多灶型HGPIN,故应于首次穿刺后4~6周行再次穿刺以明确诊断。孤立HGPIN患者应定期进行PSA水平、直肠指检、经直肠前列腺超声等检查随诊,若出现异常,需行再次穿刺活检明确诊断。
1 Jemal A,Siegel R,Ward E,et al.Cancer statistics,2009[J].CA Cancer J Clin,2009,59(4):225-249.
2 韩苏军,张思维,陈万青,等.中国前列腺癌发病现状和流行趋势分析[J].临床肿瘤杂志,2013,18(4):330-334.
3 Nguyen DP,Li J,Tewari AK.Inflammation and prostate cancer:the role of interleukin 6[J].BJU Int,2014,113(6):986-992.
4 Di Francesco S,Tenaglia RL.Obesity,diabetes and aggressive prostate cancer hormone-naive at initial diagnosis[J].Cent European J Urol,2014,66(4):423-427.
5 Bastaros J,Placer J,Celma A,et al.Current significance of the finding of high grade prostatic intraepithelial neoplasia in the prostate biopsy[J].Actas Urol Esp,2014,38(4):270-275.
6 Montironi R,Mazzucchelli R,Lopez-Beltran A,et al.Prostatic intraepithelial neoplasia:its morphological and molecular diagnosis and clinical significance[J].BJU Int,2011,108(9):1394-1401.
7 Lee D,Lee C,Kwon T,et al.Clinical features and prognosis of prostate cancer with high-grade prostatic intraepithelial neoplasia[J].Korean J Urol,2015,56(8):565-571.
8 De Nunzio C,Trucchi A,Miano R,et al.The number of cores positive for high grade prostatic intraepithelial neoplasia on initial biopsy is associated with prostate cancer on second biopsy[J].J Urology,2009,181(3):1069-1074.
9 Lee MC,Moussa AS,Yu C,et al.Multifocal high grade prostatic intraepithelial neoplasia is a risk factor for subsequent prostate cancer[J].J Urology,2010,184(5):1958-1962.
10 Cicione A,Cantiello F,De Nunzio C,et al.Patients with metabolic syndrome and widespread high grade prostatic intraepithelial neoplasia are at a higher risk factor of prostate cancer on re-biopsy:a prospective single cohort study[J].Urol Oncol,2014,32(1):27-31.
11 Heidenreich A,Aus G,Bolla M,et al.EAU guidelines on prostate cancer[J].Actas Urol Esp,2009,33(2):113-126.
12 Adamczyk P,Wolski Z,Butkiewicz R,et al.Significance of atypical small acinar proliferation and extensive high-grade prostatic intraepithelial neoplasm in clinical practice[J].Cent European J Urol,2014,67(2):136-141.
13 Caruso C,Balistreri CR,Candore G,et al.Polymorphisms of pro-inflammatory genes and prostate cancer risk:a pharmacogenomic approach[J].Cancer Immunol Immun,2009,58(12):1919-1933.
14 De Nunzio C,Kramer G,Marberger M,et al.The controversial relationship between benign prostatic hyperplasia and prostate cancer:the role of inflammation[J].European Urol,2011,60(1):106-117.
15 Putzi MJ,De Marzo AM.Morphologic transitions between proliferative inflammatory atrophy and high-grade prostatic intraepithelial neoplasia[J].Urology,2000,56(5):828-832.
16 MacLennan GT,Eisenberg R,Fleshman RL,et al.The influence of chronic inflammation in prostatic carcinogenesis:a 5-year followup study[J].Urology,2006,176(3):1012-1016.
17 Sfanos KS,De Marzo AM.Prostate cancer and inflammation:the evidence[J].Histopathology,2012,60(1):199-215.
(收稿:2016-02-17)
Development of prostate cancer risk in patients with chronic prostate inflammation and wHGPIN during puncture rebiopsy
LIJiebing,ZHANGYanhua,YANGHongyan,ZHANGCui,LIBo,CHENGWen
Department of Ultrasound,Harbin Medical University Cancer Hospital,Harbin 150081,China
Objective The objective of this study was to investigate a risk of prostate cancer(PCa)at a repeat biopsy in patients with chronic prostate inflammation and widespread high grade prostatic intra epithelial neoplasia(wHGPIN).Methods From July 2006 to December 2014,172 cases of prostate biopsy were collected.All of them were diagnosed as HGPIN for the first biopsy,punctured by transrectal ultrasound for 12 points.After the first puncture for 6 months,patients were punctured for rebiopsy.Multi-focal wHGPIN was defined as a high-grade prostate intraepithelial neoplasia with 2 or more cores detection in a prostate biopsy.Isolated HGPIN was defined as a high-grade prostate intraepithelial neoplasia with only one core detection in a prostate biopsy.Results Seventy-two patients with HGPIN were isolated from primary HGPIN,102 patients with isolated HGPIN,17 patients with chronic prostatitis,70 with multifocal HGPIN and 54 with chronic prostatitis.Forth-eight of 172 patients initial diagnosis of HGPIN was diagnosed as PCa at rebiopsy.The detection rate of wHGPIN was 52.86%(37/70)and isolated HGPIN for 10.88%(11/102).They showed a statistically difference between two groups(P<0.001).The detection rate of PCa in HGPIN patients with chronic prostatitis was higher than that in patients without chronic prostatitis(P=0.011).Chronic prostatitis and multifocal wHGPIN were a risk factor for prostate cancer independent by rebiopsy,confirmed by the logistic regression model.Conclusion Rebiopsy is a high risk factor of prostate adenocarcinoma for patients with chronic prostatitis and multifocal HGPIN initially diagnosed by the first biopsy.Therefore,these patients are recommended under ultrasound induced by rectal prostate rebiopsy.
Prostate cancer(PCa);High grade prostatic intraepithelial neoplasia(HGPIN);Chronic prostate inflammation;Prostate biopsy
黑龙江省卫生厅科研课题(659)
哈尔滨医科大学附属肿瘤医院超声科(哈尔滨 150081)
李洁冰,女,(1974-),硕士,主治医师,从事超声诊断及超声介入的研究。
李洁冰,E-mail:lijiebing06@126.com
R737.25
A
10.11904/j.issn.1002-3070.2017.03.005
