依托咪酯-芬太尼类药物在老年胃镜检查应用的Meta分析*
2017-02-10严莲宋美璇李显蓉
严莲,宋美璇,李显蓉
(1.西南医科大学护理学院,四川 泸州 646000;2.西南医科大学附属医院 胃肠外科,四川 泸州 646000)
依托咪酯-芬太尼类药物在老年胃镜检查应用的Meta分析*
严莲1,宋美璇1,李显蓉2
(1.西南医科大学护理学院,四川 泸州 646000;2.西南医科大学附属医院 胃肠外科,四川 泸州 646000)
目的Meta分析依托咪酯和丙泊酚分别联合芬太尼类药物用于老年胃镜检查的麻醉效果及安全性。方法 计算机检索Cochrane图书馆、PubMed、Embase、中国生物医学文献数据库(CBM)、中国知网、维普资讯网和万方数据库等建库至2016年发表的关于依托咪酯-芬太尼类药物用于老年无痛胃镜术的随机对照试验(RCT),按照Jadad量表评价纳入研究的质量和提取资料,采用RevMan 5.3软件进行统计分析。结果11篇RCT(1 535例患者)纳入分析,依托咪酯组(E组)765例,丙泊酚组(P组)770例。依托咪酯组患者心率(HR)[加权均数差(WMD)=2.25,95%CI(0.93,3.56),P =0.001]和平均动脉压(MAP)[WMD=9.09,95%CI(7.60,10.57),P =0.000]的变化幅度较丙泊酚组小,发生低氧血症[=0.46,95%CI(0.32,0.65),P =0.000]的风险较丙泊酚组低,差异有统计学意义;不良反应的发生方面,依托咪酯组发生呼吸暂停[=0.26,95%CI(0.15,0.48),P =0.000]、注射痛[=0.02,95%CI(0.01,0.05),P =0.000]的风险较丙泊酚组低,发生恶心呕吐[=3.44,95%CI(2.03,5.84),P =0.000]、肌阵挛[=8.14,95%CI(4.18,15.87),P =0.000]的风险较丙泊酚组高,差异有统计学意义。结论依托咪酯联合芬太尼类药物用于老年无痛胃镜术能较好地保持循环系统稳定,是一种安全有效的麻醉方案。
依托咪酯;丙泊酚;胃镜;老年;Meta分析
胃镜是上消化道疾病常用辅助检查之一,老年并不是胃镜检查的绝对禁忌证,约50%~65%的老年人呼吸、循环功能减退,大多合并高血压和冠心病等循环系统疾病,传统的胃镜检查会影响患者的循环、呼吸系统,引起恶心、呕吐[1-4]。无痛胃镜是患者在麻醉药物的作用下进入镇定、睡眠的状态时进行的胃镜检查操作,能大大减轻患者的痛苦,目前常见的几种麻醉药物,包括苯二氮卓类、非巴比妥类和阿片类等药物[5-7]。依托咪酯是一类非巴比妥类药物,通过中枢神经系统的γ-氨基丁酸(γ-aminobutyric acid,GABA)受体诱导麻醉,起效迅速,有轻微的血管舒张作用,改善冠状动脉的血流量,对循环系统和呼吸系统的影响较小,是冠心病和休克患者麻醉用药较好的选择[8-12]。丙泊酚也是一类非巴比妥类药物,但其在麻醉过程中易引起呼吸抑制和低血压,在老年人群中应用的安全性值得探讨[13-15]。芬太尼类药物(芬太尼、瑞芬太尼和舒芬太尼)属于阿片类药物,常与依托咪酯或丙泊酚联用,可以减少药物剂量,减轻恶心呕吐等不良反应[15-17]。无痛胃镜应用于老年人群的安全性和有效性仍缺乏临床证据。本文采用Meta分析的方法,对已公开发表的依托咪酯与丙泊酚分别联合芬太尼类药物用于老年人群无痛胃镜的随机对照试验(ran domized controlled trial,RCT)进行比较分析,探寻老年人群胃镜麻醉的最佳方案,为临床实践提供依据。
1 资料与方法
1.1.1 纳入标准研究类型为RCT。研究对象为需行无痛胃镜检查的老年患者(年龄≥60岁),无重要器官功能障碍疾病及药物过敏史。干预措施:实验组(E组)依托咪酯联合芬太尼类药物实施麻醉;对照组(P组)丙泊酚(又名异丙酚)联合芬太尼类药物实施麻醉。观察指标:①心率(heart rate,HR)(心动过缓:HR<60次/min);②平均动脉压(mean
1.1 文献纳入arterial pressure,MAP);③血氧饱和度(pulse oxygen saturation,SpO2)(低氧血症:SpO2<90%);④不良反应:呼吸暂停、注射痛、恶心呕吐和肌阵挛。
1.1.2 排除标准
患者年龄小于60岁;联合使用其他麻醉药物或辅助药物;样本例数低于30例;文献中数据表述不清或不完整,无法进行Meta分析或系统评价;统计数据不符合条件;重复发表、各种原因无法获得全文的文献。
1.2 文献检索
计算机检索Cochrane图书馆、PubMed、Embase、中国生物医学文献数据库(CBM)、中国知网、维普资讯网、万方数据库,检索时限从建库至2016年。文献检索语种为英文和中文。英文检索词:etomidate;propofol;gastroscopy;aged。中文检索关键词:依托咪酯;丙泊酚;胃镜;老年。
1.3 文献筛选与资料提取
由两名评价者按照纳入和排除标准独立进行初筛,并进一步查找和阅读文献进行复筛,进行交叉比对,若遇分歧则讨论解决或交由第3位研究者裁定。提取作者及年份、研究例数、随机方法、盲法、药物的剂量及用法、结局指标等信息。
1.4 文献质量评价
按照Jadad量表对纳入研究的方法学质量进行评价,评价内容包括:①随机序列的产生;②随机化隐藏;③盲法;④退出与失访。前3项评价表示为恰当(2分)、不清楚(1分)、不恰当(0分);退出与失访表示为有(1分)或无(0分),计算总分后1~3分视为低质量,4~7分视为高质量。
1.5 统计学方法及发表偏倚的估计
采用Cochrane协作网提供的RevMan 5.3软件进行Meta分析。采用χ2检验和I2检验对纳入研究进行临床异质性检验,以α=0.1为检验水准,若各研究之间无异质性(P >0.1,I2<50%),则选择固定效应模型进行Meta分析,若各研究间异质性高(P <0.1,I2>50%),分析异质性产生的原因,采取亚组分析或采用逐个剔除法行敏感性分析,减少异质性的影响。对连续型变量采用加权均数差(weighted mean difference,WMD),计数资料采用比值比(odds ratio,)作为效应量,所有效应量均计算其95%可信区间(confidence interval,CI),以P<0.05为差异有统计学意义。若两个研究组之间存在统计学异质性而没有临床异质性或差异无统计学意义时,采用随机效应模型:如两组异质性过大或无法找寻数据来源时,采用描述性分析。
2 结果
2.1 检索结果
根据检索策略初筛文献共计329篇。英文26篇,中文303篇。阅读题目及摘要初筛剩余文献17篇,阅读全文复筛剩余文献11篇,最后共纳入文献11篇,共1 535例患者。文献筛选流程见图1。
2.2 纳入研究的基本特征及质量评价
所有研究均提及“随机”,部分研究未描述具体的随机化方法。纳入研究的基本特征见表1,质量评估结果见表2。
图1 文献筛选流程图Fig. 1 Study flowdiagram

表1 纳入研究的基本特征Table 1 Characteristics of included studies

表2 纳入研究的质量评价Table 2 Quality evaluation of included studies
2.3 Meta分析结果
2.3.1HHRR11篇文献[18-28]报道了两组老年患者麻醉前后胃镜操作中和结束后的HR水平。11篇文献的患者麻醉前基础HR水平差异没有统计学意义,资料具有可比性;麻醉状态胃镜操作中,11篇文献的HR水平合并异质性较大,异质性可能来源于各研究取值的时间点不同,合并7篇[19-22,24-26]研究,发表偏倚,见图2。异质性较小(P =0.290,I2=18%),HR水平的差异有统计学意义[WMD=2.25,95%CI(0.93,3.56),P =0.001],见图3。表明依托咪酯组患者胃镜检查中HR的波动较丙泊酚组小。心动过缓的发生情况,纳入5篇文献[19-20,24,26,28]报道的心动过缓的发生例数,其差异无统计学意义。见图4。
2.3.2 MMAAPP10篇文献[18-27]报道了两组老年患者在麻醉前和麻醉起效后行胃镜术中的MAP水平。麻醉前,两组患者的基础MAP水平差异均无统计学意义,资料具有可比性;麻醉起效后,合并10篇[18-27]研究报道的胃镜操作中MAP水平异质性较大,异质性来源可能与取值时间点不同,合并8篇[19,21-27]的研究,发表偏倚,见图5。异质性较小(P =0.380,I2=6%),MAP水平差异有统计学意义[WMD=9.09,95%CI (7.60,10.57),P =0.000] ,见图6。结果表明依托咪酯组患者MAP下降的程度较丙泊酚组轻。

图2 HR的漏斗图Fig.2 Funnel plot of analyzed data on heart rate
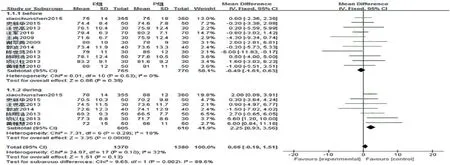
图3 HR的森林图Fig.3 Forest plot of pooled data on heart rate
2.3.3 SpO3 SpO29篇文献[18,21-28]报道了两组患者麻醉前和麻醉后胃镜操作中的SpO2水平。麻醉前的SpO2的基础值差异均无统计学意义,资料具有可比性。胃镜操作中,各研究报道的SpO2合并起来异质性较大,分析其异质性产生的原因可能与采用的吸氧浓度、给氧方式不同有关。项以柱[25]、汪军[18]、郭波[21]、黄雅慧[26]和陈明浩[24]的研究中各采用鼻导管吸氧2、3、3、3和5 L/min,结果表明两组患者SpO2差异有统计学意义,都认为依托咪酯组患者SpO2下降程度较丙泊酚组低;陈世鸿[23]和王尚[27]的研究各采用鼻导管吸纯氧3 L/min、面罩吸氧5 L/min,其结果表明两组患者SpO2水平变化差异无统计学意义。低氧血症的发生情况,合并5篇[18-20,24,26]的文献报道的低氧血症发生例数,异质性较小(P =0.180,I2=36%),结果显示差异有统计学意义[=0.46,95%CI(0.32,0.65),P =0.000],见图7。表明依托咪酯组发生低氧血症的风险较丙泊酚组低。

图4 心动过缓发生率的森林图Fig.4 Forest plot of pooled data on the incidence of bradycardia

图5 MAP的漏斗图Fig.5 Funnel plot of analyzed data on mean arterial pressure
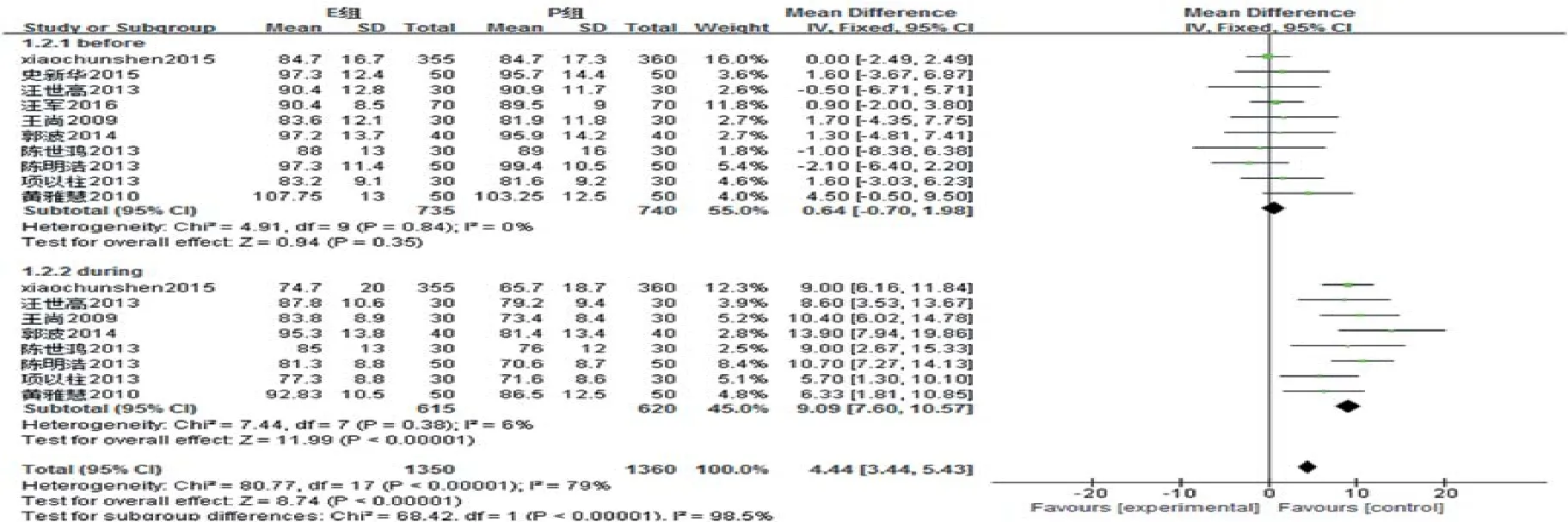
图6 MAP的森林图Fig.6 Forest plot of pooled data on mean arterial pressure
2.3.4 呼吸暂停合并5篇文献[19-20,24-26]报道的呼吸暂停发生例数,异质性较小(P =0.340,I2=12%),结果显示差异有统计学意义[=0.26,95%CI(0.15,0.48),P =0.000],见图8。表明依托咪酯组发生呼吸暂停的风险较丙泊酚组低。
2.3.5 注射痛7篇文献[18-21,24,26-27]报道了注射痛的发生例数,合并分析4篇[19-21,24]异质性较小(P =0.360,I2=6%)的文献,结果显示其差异有统计学意义[= 0.02,95%CI(0.01,0.05),P =0.000],见图9。依托咪酯组发生注射痛的风险较丙泊酚组低。
2.3.6 恶心呕吐8篇文献[18-21,23-24,26-27]报道了恶心呕吐的发生情况,合并分析异质性较小(P =0.270,I2=20%),结果显示其差异有统计学意义[=3.44,95%CI(2.03,5.84),P =0.000],见图10。表明依托咪酯组发生恶心呕吐风险较丙泊酚组高。
2.3.7 肌阵挛7篇文献[18-21,24,26-27]报道了的肌阵挛发生例数,合并分析异质性较小(P =0.950,I2=0%),结果显示差异有统计学意义[=8.14,95%CI(4.18,15.87),P =0.000],见图11。表明依托咪酯组发生肌阵挛的风险较丙泊酚组高。

图7 低氧血症发生率的森林图Fig.7 Forest plot of pooled data on the incidence of hypoxemia

图8 呼吸暂停发生率的森林图Fig.8 Forest plot of pooled data on the incidence of apnea
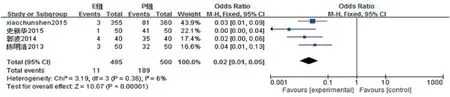
图9 注射痛发生率的森林图Fig.9 Forest plot of pooled data on the incidence of injeaction pain
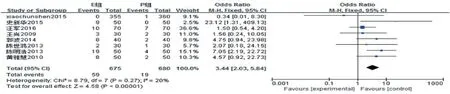
图10 恶心呕吐发生率的森林图Fig.10 Forest plot of pooled data on the incidence of nausea and vonciting
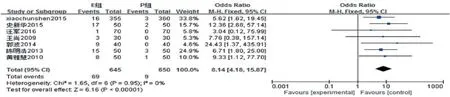
图11 肌阵挛发生率的森林图Fig.11 Forest plot of pooled data on the incidence of myoclomus
3 讨论
无痛胃镜是目前减轻患者恶心呕吐,有效提高依从性的内镜检查手段。本研究采用Meta分析的方法重点比较依托咪酯与丙泊酚分别联合芬太尼类药物在老年胃镜应用中的有效性和安全性,其结果显示依托咪酯组患者HR、MAP、SpO2的波动幅度较丙泊酚组小,发生低氧血症、呼吸暂停、注射痛的风险较丙泊酚组低,但发生恶心呕吐、肌阵挛的风险较丙泊酚组高。依托咪酯最大的药物特性是具有良好的血流动力学稳定性,起效迅速,7~14 min自然苏醒,对呼吸抑制作用较小,几乎不影响自主神经系统,对交感神经系统和压力感受器的影响较小,不影响心脏的收缩功能,临床剂量0.10~0.30 mg/kg范围内,心排血量与心脏指数稍增加,HR略减慢[1,29]。依托咪酯乳剂所使用的溶剂为20%中长链甘油三酯,接近正常人体的生理渗透浓度,对血管几乎无刺激,而丙泊酚乳剂中以长链的甘油三酯为主,对血管的刺激性较大,注射部位疼痛感明显[30-31],低血压和呼吸抑制发生率也较高[7,32-33]。恶心呕吐是依托咪酯常见的副作用之一,检查前常规禁食禁饮避免误吸,芬太尼类药物预给药可减轻其反应[13,34-35]。肌阵挛在依托咪酯应用中的发生率大约为20%~45%[7,36],与注射剂量和浓度相关,0.10~0.30 mg/kg的安全剂量范围内缓慢静脉推注,芬太尼类药物或硫酸镁预给药可一定程度上减少肌阵挛的发生[1,37-39]。此外,虽然在依托咪酯组低氧血症和呼吸暂停的发生风险不高,但麻醉过程中仍应该重视操作过程SpO2的监测和有效的氧供给,可采用面罩给氧3~5 L/min。
综上所述,据现有研究的Meta分析结果表明,依托咪酯用于老年患者无痛胃镜能够降低操作刺激对HR的影响和MAP、SpO2下降的风险,具有较好的循环稳定性,较低的注射痛刺激性,但应密切关注其恶心呕吐和肌阵挛等不良反应的发生。芬太尼类药物预给药联合依托咪酯的麻醉方案应用于老年无痛胃镜术,基于对循环稳定性的考虑,特别是针对循环系统疾病的老年患者,能较好的保护心血管和脑的功能,是较有效及安全的方法。鉴于本研究纳入的11个研究,样本量小,且研究设计方案未完全阐明,笔者建议继续开展大样本、高质量、多中心的RCT进一步论证。此外,还建议开展大型的队列研究以观察依托咪酯的远期疗效及有无并发症情况。
[1] 庄心良, 曾因明, 陈伯銮. 现代麻醉学[M]. 北京: 人民卫生出版社, 2004: 1445.
[1] ZHUANG X L, ZENG Y M, CHEN B L. Modern anesthesiology[M]. Beijing: People’s Health Publishing House, 2004: 1445. Chinese
[2] JAFRI S M, MONKEMULLER K, LUKENS F J. Endoscopy in the elderly a review of the efficacy and safety of colonoscopy, esophagogastroduodenoscopy, and endoscopic retrograde cholangiopancreatography[J]. Journal of Clinical Gastroenterology, 2010, 44(3): 161-166.
[3] 陈立. 无痛胃镜与普通胃镜检查的比较[J]. 中国内镜杂志, 2012, 18(2): 220-222.
[3] CHEN L. Comparison of painless gastroscopy and common endoscopy[J]. China Journal of Endoscopy, 2012, 18(2): 220-222. Chinese
[4] 蒋远洪, 谭友果. 无痛胃镜在不同人群中的应用进展[J]. 中国内镜杂志, 2015, 21(2): 163-165.
[4] JIANG Y H, TAN Y G. Application of painless endoscopy in different population[J]. China Journal of Endoscopy, 2015, 21(2): 163-165. Chinese
[5] FANTI L, TENSTONI P A. Sedation and analgesia in gastrointestinal endoscopy: what’s new[J]. World Journal of Gastroenterology, 2010, 16(20): 2451-2457.
[6] LAPIERRE C D, JOHNSON K B, RANDALL B R, et al. A simulation study of common propofol and propofol-opioid dosing regimens for upper endoscopyimplications on the time course of recovery[J]. Anesthesiology, 2012, 117(2): 252-262.
[7] FALK J, ZED P J. Etomidate for procedural sedation in the emergency department[J]. Annals of Pharmacotherapy, 2004, 38(7-8): 1272-1277.
[8] SONG J C, LU Z J, JIAO Y F, et al. Etomidate anesthesia during ercp caused more stable haemodynamic responses compared with propofol: a randomized clinical trial[J]. International Journal of Medical Sciences, 2015, 12(7): 559-565.
[9] AGGARWAL S, GOYAL V K, CHATURVEDI S K, et al. A comparative study between propofol and etomidate in patients under general anesthesia[J].Revista Brasileira Journal De Anesthesiologia, 2016, 66(3): 237-241.
[10] DMELLO D. Supplemental corticosteroids after intubation using etomidate in severe sepsis and septic shock[J]. Critical Care Medicine, 2012, 40(6): 2003-2004.
[11] MOREL J, SALARD M, CASTELAIN C, et al. Haemodynamic consequences of etomidate administration in elective cardiac surgery: a randomized double-blinded study[J]. British Journal of Anaesthesia, 2011, 107(4): 503-509.
[12] AKCABOY Z N, AKCABOY E Y, ALBAYRAK D, et al. Can remifentanil be a better choice than propofol for colonoscopy during monitored anesthesia care[J]. Acta Anaesthesiologica Scandinavica, 2006, 50(6): 736-741.
[13] 汪世高, 万行荣, 张艳琴,等. 靶控输注依托咪酯与异丙酚在肠镜检查中的应用[J]. 中国内镜杂志, 2011, 17(5): 495-498.
[13] WANG S G, WAN H R, ZHANG Y Q, et al. Application of etomidate or propofol given by target controlled infusion in colonoscopy sedation[J]. China Journal of Endoscopy, 2011, 17(5): 495-498. Chinese
[14] 裘剑波, 齐超, 林家燕, 等. 依托咪酯与丙泊酚复合咪哒唑仑及芬太尼麻醉在老年患者无痛结肠镜检查治疗中的比较[J].中国内镜杂志, 2014, 20(3): 313-316.
[14] QIU J B, QI C, LIN J Y, et al. Application of etomidate combined with midazolam and fentanyl to anesthesia in joint painless gastroscopy and colonoscopy[J]. China Journal of Endoscopy, 2014, 20(3): 313-316. Chinese
[15] TOKLU S, IYILIKCI L, GONEN C, et al. Comparison of etomidate-remifentanil and propofol-remifentanil sedation in patients scheduled for colonoscopy[J]. European Journal of Anaesthesiology, 2009, 26(5): 370-376.
[16] ZHANG L, BAO Y, SHI D. Comparing the pain of propofol via different combinations of fentanyl, sufentanil or remifentanil in gastrointestinal endoscopy[J]. Acta Cirurgica Brasileira, 2014, 29(10): 675-680.
[17] 刘振伟, 曹刚. 小剂量芬太尼联合丙泊酚静脉麻醉在胃镜检查中的应用[J]. 中国内镜杂志, 2015, 21(7): 746-748.
[17] LIU Z W, CAO G. Effect of small doses fentanyl combined with propofolintravenous anesthesia on patients undergoing gastroscopy[J]. China Journal of Endoscopy, 2015, 21(7): 746-748. Chinese
[18] 汪军. 三种静脉全麻方法在高龄患者无痛胃镜检查中的应用及效果比较[J]. 现代消化及介入诊疗, 2016, 21(1): 17-20.
[18] WANG J. The effects of three general anesthesia methods in elderly patients receiving painless gastroscopy[J]. Modern Digestion & Intervention, 2016, 21(1): 17-20. Chinese
[19] SHEN X C, AO X, CAO Y, et al. Etomidate-remifentanil is more suitable for monitored anesthesia care during gastroscopy in older patients than propofol-remifentanil[J]. Medical Science Monito, 2015, 21: 1-8.
[20] 史新华, 傅启英, 倪俊, 等. 利多卡因联合依托咪酯在老年人无痛胃镜中的应用[J]. 世界临床药物, 2015, 36(4): 256-260.
[20] SHI X H, FU Q Y, NI J, et al. Application of lidocaine plus etomidate for elderly painless gastroscopy[J]. World Clinic Drugs, 2015, 36(4): 256-260. Chinese
[21] 郭波, 张树兵, 肖永忠, 等. 丙泊酚复合依托咪酯用于老年患者无痛胃镜检查效果观察[J]. 西南军医, 2014, 16(6): 654-655.
[21] GUO B, ZHANG S B, XIAO Y Z, et al. Application of propofol plus etomidate for elderly painless gastroscopy[J]. Journal of Military Surgeon in Southwest China, 2014, 16(6): 654-655. Chinese
[22] 汪世高, 李荆钟, 万行荣, 等. 靶控输注依托咪酯或异丙酚在老年患者胃镜检查中的应用[J]. 中国内镜杂志, 2013, 19(2): 161-163.
[22] WANG S G, LI J Z, WANG H R, et al. Application of etomidate or propofol given by target controlled infusion in aged gastroscopy sedation[J]. China Journal of Endoscopy, 2013, 19(2): 161-163. Chinese
[23] 陈世鸿. 依托咪酯乳剂和丙泊酚分别复合舒芬太尼在老年患者门诊无痛胃镜检查的观察[J]. 医药前沿, 2013, 3(14): 117-118.
[23] CHEN S H. Etomidate emulsion composite sufentanil and propofol painless gastroscopy in elderly patients with clinic observation[J]. Journal of Frontiers of Medicine, 2013, 3(14): 117-118. Chinese
[24] 陈明浩, 孟庆涛, 夏中元. 依托咪酯在门诊老年患者无痛胃镜诊疗中应用的效果分析[J]. 热带医学杂志, 2013, 13(9): 1109-1112.
[24] CHEN M H, MENG Q T, XIA Z Y. Efficacy of etomidate in the painless gastroscopy in the elderly[J]. Journal of Tropical Medicine, 2013, 13(9): 1109-1112. Chinese
[25] 项以柱. 依托咪酯复合低剂量舒芬太尼在门诊老年患者无痛胃镜中的应用[J]. 海峡药学, 2013, 25(4): 161-162.
[25] XIANG Y Z. Etomidate composite low doses sufentanil in clinic the application of the elderly patients with painless gastroscope[J]. Strait Pharmaceutical Journal, 2013, 25(4): 161-162. Chinese
[26] 黄雅慧, 金梅生, 孙洁, 等. 依托咪酯、芬太尼静脉麻醉在老年人胃镜检查中的应用[C] // 第三届全国老年消化内镜及消化病学术会议暨2010年新疆3E论坛论文集, 2010: 93-95.
[26] HUANG Y H, JIN M S, SUN J, et al. Application of etomidate and fentanyl intravenous anesthesia in the endoscopy of the elderly[C] // The Third national conference on endoscopy and digestive endoscopy of the elderly and 2010, Xinjiang, China 3E Forum Proceedings, 2010: 93-95. Chinese
[27] 王尚, 郑秀英. 依托咪酯联合瑞芬太尼在老年患者无痛胃镜检查中的应用[J]. 中国医药, 2009, 4(7): 524-526.
[27] WANG S, ZHENG X Y. Effect of etomidate combined with remifentanil during painless gastroscopy in elderly patients[J]. China Medicine, 2009, 4(7): 524-526. Chinese
[28] 谢翠英. 依托咪酯用于老年病人无痛胃镜检查的麻醉效果及安全性分析[J]. 临床医药实践, 2009, 18(20): 1883-1884.
[28] XIE C Y. Etomidate used in painless gastroscopy of elderly patients anesthesia effi cacy, and safety analysis [J]. Proceeding of Clinical Medicine, 2009, 18(20): 1883-1884. Chinese
[29] FORMAN S A. Clinical and molecular pharmacology of etomidate[J]. Anesthesiology, 2011, 114(3): 695-707.
[30] VINSON D R, BRADBURY D R. Etomidate for procedural sedation in emergency medicine[J]. Annals of Emergency Medicine, 2002, 39(6): 592-598.
[31] NYMAN Y, VON HOFSTEN K, PALM C, et al. Etomidate-® Lipuro is associated with considerably less injection pain in children compared with propofol with added lidocaine[J]. British Journal of Anaesthesia, 2006, 97(4): 536-539.
[32] YAGAN Ö, TAS N, KÜÇÜK A, et al. Haemodynamic responses to tracheal intubation using propofol, etomidate and etomidatepropofol combination in anaesthesia induction[J]. Journal of Cardiovascular & Thoracic Research, 2015, 7(4): 134-140.
[33] ZHOU X, LI B X, CHEN L M, et al. Etomidate plus propofol versus propofol alone for sedation during gastroscopy: a randomized prospective clinical trial[J]. Surgical Endoscopy,2016, 30(11): 5108-5116.
[34] FORMAN S A. Clinical and molecular pharmacology of etomidate[J]. Anesthesiology, 2011, 114(3): 695-707.
[35] RUTH W J, BURTON J H, BOCK A J. Intravenous etomidate for procedural sedation in emergency department patients[J]. Academic Emergency Medicine, 2001, 8(1): 13-18.
[36] MINER J R, DANAHY M, MOCH A, et al. Randomized clinical trial of etomidate versus propofol for procedural sedation in the emergency department[J]. Annals of Emergency Medicine, 2007, 49(1): 15-22.
[37] DOENICKE A W, ROIZEN M F, KUGLER J, et al. Reducing myoclonus after etomidate[J]. Anesthesiology, 1999, 90(1): 113-119.
[38] RI H S, SHIN S W, KIM T K, et al. The proper effect site concentration of remifentanil for prevention of myoclonus after etomidate injection[J]. Korean Journal of Anesthesiology, 2011, 61(2): 127-132.
[39] 汪伟, 吕洁, 钱燕宁, 等. 羟考酮或芬太尼预给药对依托咪酯所致肌阵挛的影响[J]. 临床麻醉学杂志, 2015, 31(7): 707-708.
[39] WANG W, LV J, QIAN Y N, et al. Oxycodone or fentanyl dose of etomidate in advance due to the influence of myoclonus[J]. Journal of Clinical Anesthesiology, 2015, 31(7): 707-708. Chinese
(吴静 编辑)
Etomidate plus Fentanyl-class drugs applied in older patients undergoing gastroscopy: a meta-analysis*
Lian Yan1, Mei-xuan Song1, Xian-rong Li2
(1.Nursing College, Southwest Medical University, Luzhou, Sichuan 646000, China; 2. Department of Gastrointestinal Surgery, the Affi liated Hospital of Southwest Medical University, Luzhou, Sichuan 646000, China)
ObjectiveTo make a systematical review of the safety and effi cacy of Etomidate plus Fentanylclass drugs and Propofol plus Fentanyl-class drugs in older patients undergoing gastroscopy. Methods We searched the Cochrane library, PubMed, Embase, China Biology Medicine (CBM), CNKI, VIP, Wanfang Database for all randomized controlled trials (RCTs) about the effi cacy of Etomidate plus Fentanyl-class drugs(Fentanyl, Sufentanil, remifentanil) in older patients undergoing gastroscopy. The quality of the studies was evaluated by the method recommended by the Jadad scale. Meta-analysis was conducted using the Cochrane Collaboration’s RevMan 5.3 software.Results11 RCTs involving 1 535 patients were analyzed. Meta-analysis showed that patients in the Etomidate group had a lower heart rate [Weighted Mean Difference (WMD)=2.25, 95%CI(0.93, 3.56), P = 0.001] and mean arterial pressure [WMD = 9.09, 95%CI (7.60, 10.57), P = 0.000] fl uctuation than whose of the Propofol group.The hypoxemia occurrence [=0.46, 95% CI (0.32, 0.65), P = 0.000] in Etomidate group is also lower than which of the Propofol group. For side effects aspects, the risk of apnea[=0.26, 95%CI(0.15, 0.48), P = 0.000] and injectionpain [= 0.02, 95%CI (0.01, 0.05), P = 0.000] in the Etomidate group is much lower than the Propofol group ,while the myoclonus [=8.14, 95%CI (4.18, 15.87), P = 0.000], nausea and vomiting [=3.44, 95%CI (2.03, 5.84),P = 0.000] were more incidental than the Propofol group.ConclusionEtomidate plus Fentanyl-class drugs can effectively maintain circulatory system for the old undergoing painless gastroscopy, demonstrated to be a safe and valid anesthesia method.
Etomidate; Propofol; gastroscopy; aged; meta-analysis
R619
: A
10.3969/j.issn.1007-1989.2017.01.002
1007-1989(2017)01-0006-09
2016-07-27
四川省科技厅资助项目(No:2016SZ0062)
李显蓉,E-mail:1204987356@qq.com
