缺血性脑卒中患者氯吡格雷抵抗与颈动脉狭窄的相关性分析
2016-11-29薛森新周伯荣通讯作者宋成宪邓燕华
薛森新 周伯荣(通讯作者) 宋成宪 邓燕华
广州医科大学附属第三医院 1)康复科 2)神经内科 广州 510150
缺血性脑卒中患者氯吡格雷抵抗与颈动脉狭窄的相关性分析
薛森新1)周伯荣2)(通讯作者) 宋成宪1)邓燕华2)
广州医科大学附属第三医院 1)康复科 2)神经内科 广州 510150
目的 探讨缺血性脑卒中患者氯吡格雷抵抗与颈动脉狭窄的相关性。方法 比浊法测定缺血性脑卒中患者服用氯吡格雷(75 mg/d)前及服用2周后血小板聚集率变化。根据血小板聚集率变化将病例分为氯吡格雷抵抗(clopidogrel resistance,CR)组和氯吡格雷敏感(clopidogel sensitivity,CS)组。比较CR组和CS组相关的临床数据,并使用多变量Logistic回归分析确定CR的独立危险因素。结果 228例缺血性脑卒中患者,其中CR组54例(23.68%),CS组174例(76.32%)。单因素分析结果显示:年龄(P=0.015)、血小板数量(P=0.012)、中度颈动脉狭窄(P=0.034)、性别(P=0.049)和糖尿病(P=0.032)在CR组和CS组中均存在显著差异。多因素Logistic分析结果显示,年龄(P=0.004)、血小板数量(P=0.025)、糖尿病(P=0.026)、中度颈动脉狭窄(P=0.002)是 CR 发生的独立危险因素。结论 缺血性脑卒中患者CR与多种因素相关,其中中度颈动脉狭窄是CR的独立危险因素之一。
缺血性脑卒中;氯吡格雷抵抗;血小板聚集;颈动脉狭窄
氯吡格雷可显著降低新的缺血性事件(包括心肌梗死、缺血性脑卒中和其他血管疾病死亡)的发生率[1]。但随着氯吡格雷在临床中的大量应用,已发现患者对该药临床反应存在显著的个体差异,有部分患者存在对氯吡格雷的低反应或无反应性,这种现象在临床上被称为氯吡格雷抵抗(clopidogrel resistance,CR)[2]。本研究旨在探讨缺血性脑卒中患者CR与颈动脉狭窄的相关性。
1 资料和方法
1.1 研究对象 选择2009-03至今广州医科大学附属第三医院神经内科住院的首次或再次新发作急性缺血性脑卒中患者228例。其中CR组54例(23.68%),CS组174例(76.32%)。诊断符合中华医学会神经病学分会脑血管病学组制定的标准[3],经CT 或MRI 确诊。入选标准:(1)首次服用氯吡格雷,或以前曾服用但已停药至少2 周以上,无氯吡格雷过敏者;(2)近2 周未服用阿司匹林、双嘧达莫、噻氯匹定等对血小板功能有一定影响的药物;(3)无严重的心肝肾功能损害或合并出血、肿瘤或免疫系统、呼吸系统等疾病;(4)血小板计数>150×109/L 且<500×109/L;(5)卒中前未行较大手术或严重外伤者;(6)按要求正规服用药物者;(7) 年龄45~89岁。
1.2 资料收集 收集患者的一般情况,如年龄、性别,既往病史:如冠心病、高血压、糖尿病等;颈动脉彩超及血常规、凝血常规、血小板聚集率测定、生化常规、血脂等实验室检查,记录所有患者的高密度脂蛋白(high densitylipoproteins,HDL)、低密度脂蛋白(low density lipoproteins,LDL)、总胆固醇、甘油三酯、空腹血糖水平、血小板计数、尿酸、血压、血小板聚集率测定,统计患者颈动脉狭窄分级情况。
1.3 血小板聚集率测定 采用目前被视为血小板聚集功能测定的金标准[4]的光比浊法检测血小板聚集率,检测氯吡格雷服药前、后2周的血小板聚集率。
参照Gurbel等[4]提出的标准,使用5 μmol/L ADP作为激动剂,以百分比计算血小板聚集率,氯吡格雷给药后血小板聚集率较基线下降幅度≤10%为CR,反之为氯吡格雷敏感(clopidogel sensitivity,CS)。
1.4 颈动脉彩超检测颈动脉狭窄 动脉狭窄程度分类:按照北美症状性颈动脉内膜切除术试验协作组(NASCET)标准[5],计算公式为:NASCET狭窄=(1-最窄处的颈动脉血流宽度/狭窄远端正常颈动脉直径)×100%,分为4个等级:(1)轻度狭窄:0~29%;(2)中度狭窄:30%~69%;(3)重度狭窄:动脉内径缩小70%~99%;(4)完全闭塞:100%。

2 结果
单因素分析显示,年龄(P=0.015)、血小板计数(P=0.012)、性别(P=0.049)、糖尿病(P=0.032)、中度颈动脉狭窄(P=0.034)在CR组和CS组存在显著差异。见表1。将CR作为因变量,单因素分析中差异有统计学意义的年龄、血小板数量、糖尿病、中度颈动脉狭窄、性别作为自变量行多因素Logistic分析,结果显示,年龄(P=0.004)、血小板数量(P=0.025)、糖尿病(P=0.026)、中度颈动脉狭窄(P=0.002)是 CR 发生的独立危险因素。见表2。
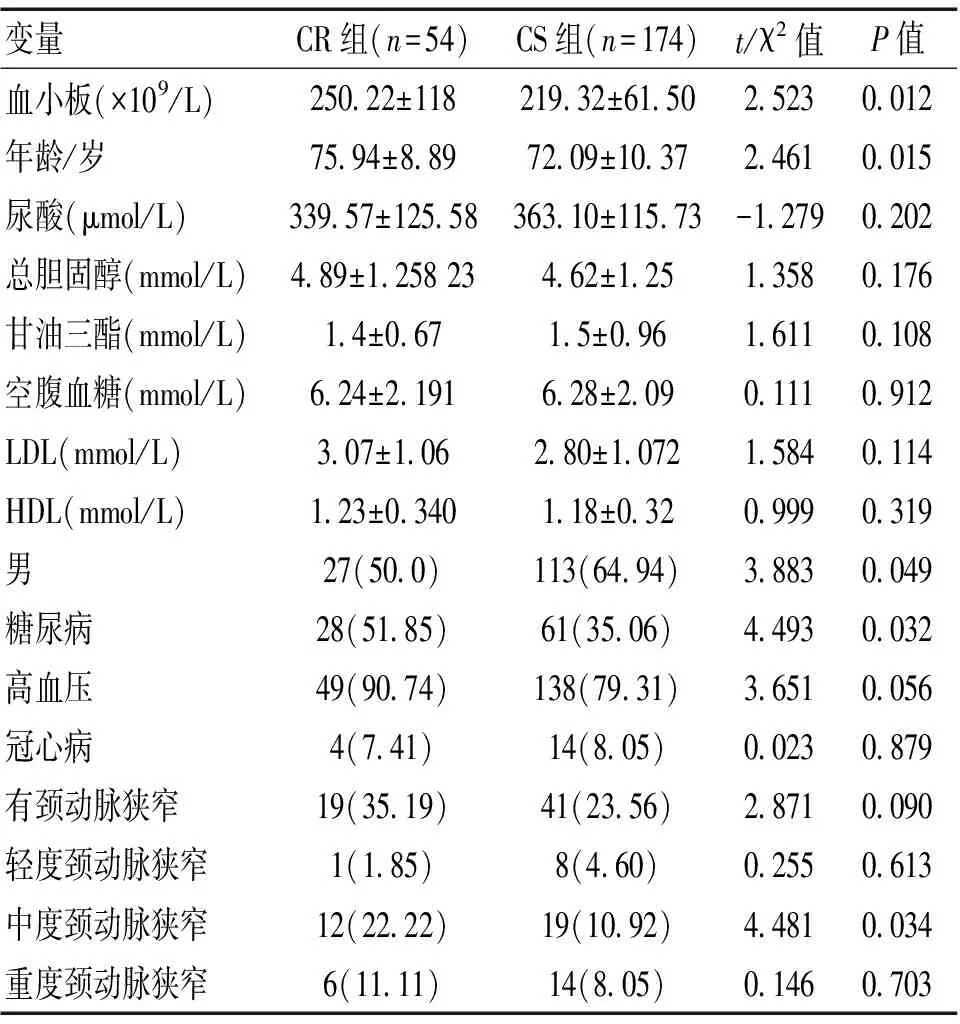
表1 2组单因素分析

表2 CR 发生的多因素Logistic回归分析
3 讨论
血小板的聚集性增加是缺血性脑卒中发生发展的重要病理基础,因此,防治缺血性脑卒中的复发及进展就是以阻止血小板活化、黏附以及聚集为目的,尤其是急性缺血性脑卒中治疗中需要迅速、有效地抑制血小板聚集[6]。而氯吡格雷作为一种不可逆抑制血小板聚集的噻吩吡啶类化合物,其活性代谢产物与位于血小板上的ADP受体P2Y12不可逆性结合,减少ADP结合位点,阻断ADP对腺苷酸环化酶的抑制作用,进而抑制血小板聚集,所以,氯吡格雷常用于缺血性脑卒中的一级及二级预防。然而,氯吡格雷的抗血小板聚集效果存在显著的个体差异,很大一部分患者存在抵抗现象。本研究显示,缺血性脑卒中患者中CR发生率为23.68%,与文献[7]报道的28%~44%相近。故监测卒中患者的血小板聚集率,及早发现CR患者,及时采取措施,有助于卒中的防治。
Geisler等[8]报道,年龄在≥65岁患者发生氯吡格雷抵抗的几率会增加。本研究也显示,年龄与CR发生显著相关。血小板数量与CR相关性显著,是 CR 发生的独立危险因素,但从血小板的数量分布来看,所有患者的血小板分布在(100~300)×109,临床意义不明确。2型糖尿病患者易出现抗血小板抵抗[9]。Westerbacka等[10]发现,在胰岛素抵抗的肥胖症患者中氯吡格雷抗血小板的作用明显受限。本研究也显示,糖尿病是CR的独立危险因素,与既往的研究[11]结果相吻合。
研究发现,氯吡格雷抵抗者的动脉粥样硬化明显高于对照组[12]。2012年Takeda等[13]通过CTA影像技术和组织病理学技术显示,服用抗血小板药物氯吡格雷的鼠在预防大动脉出现动脉粥样硬化方面,明显优于未进行抗血小板治疗预防的鼠。临床研究亦支持CR的患者,在心脏PCI手术后,出现冠脉粥样硬化和钙化的发生率明显高于非CR组[14]。2012年,Kim等[15]的研究显示,高激活状态或不充分的抗血小板治疗,导致血管造影后的静息性或腔隙性梗死明显增加。本研究结果显示,中度颈动脉狭窄是CR的独立危险因素.粥样斑块病变通过炎症反应会激活血小板的功能[16],在我们的研究中,轻度动脉狭窄在CR组和CS组中无显著差异;中度颈动脉狭窄是CR发生的独立危险因素,可能的原因是中度狭窄导致的炎症反应较强而导致血小板的激活从而导致CR。重度动脉狭窄与CR相关性无统计学意义,考虑重度狭窄血管重塑性和可塑性明显下降,血管壁和内膜明显机化,血流动力学降低,机体炎症反应可能非主要病理生理机制。而氯吡格雷抵抗会反过来导致急性颈动脉支架血栓形成[17],本研究中颈动脉中度狭窄和CR的显著相关估计是一个长期积累的过程,也可能有个体化的因素影响。
综上,中度颈动脉狭窄是缺血性脑卒中患者CR的独立危险因素之一。但目前CR尚缺乏统一的定义、诊断标准和公认的检测方法,且本次研究样本量较少,相关结果还需要今后进一步扩大样本量验证。
[1] Chen ZM,Jiang LX,Chen YP,et al.Addition of clopidogrel to aspirin in 45,852 patients with acute myocardial infarction:randomised placebo-controlled trial[J].Lancet,2005,366(9 497):1 607-1 621.
[2] Sofi F,Marcucci R,GoriA M,et al.Clopidogrel non-responsiveness and risk of cardiovascular morbidity.an updated meta-analysis[J].Thromb Haemost,2010,103(4):841-848.
[3] 中华医学会神经病学分会脑血管病学组急性缺血性脑卒中诊治指南撰写组.中国急性缺血性脑卒中诊治指南2010[J].中华神经科杂志,2010,14(12):153.
[4] Gurbel PA,Becker RC,Mann KG,et al.Platelet function monitoring in patients with coronary artery disease[J].J Am Coll Cardiol,2007,50(19):1 822-1 834.
[5] U-King-Im JM,Trivedi RA,Cross JJ,et al.Measuring carotid stenosis on contrast-enhanced magnetic resonance angiography:diagnostic performance and reproducibility of three different methods[J].Stroke,2004,8(18):2 083-2 088.
[6] 张华平,朱红丽,闫素华.临床药师对脑梗死患者应用阿司匹林进行二级预防的影响[J].医学信息,2010,23(23):2 331-2 332.
[7] Lee JM,Park S,Shin DJ,et al.Relation of genetic polymorphisms in the cytochrome P450 gene with clopidogrel resistance after drug-eluting stent implantation in Koreans[J].Am J Cardiol,2009,104(1):46-51.
[8] Gilard M,Arnaud B,Cornily JC,et al.Influence of omeprazole on the antiplatelet action of clopidogrel associated with aspirin:A randomized,double-blind OCLA(Omeprazole Clopidogrel Aspirin) Study[J].J Am Coll Cardiol,2008,12(31):256-260.
[9] Matsuno H,Tokuda H,Ishisaki A,et al.P2Y12 receptors play a significant role in the development of platelet microaggregation in patients with diabetes[J].J Clin Endocrinol Metab,2005,90(2):920-927.
[10] Westerbacka J,Yki-Järvinen H,Turpeinen A,et al.3.Inhibition of platelet-collagen interaction:an in vivo action of insulin abolished by insulin resistance in obesity[J].Arterioscler Thromb Vasc Biol,2002,22(1):167-172.
[11] 石红婷,周伯荣,王融,等.缺血性卒中患者氯吡格雷抵抗的危险因素:前瞻性病例系列研究[J].国际脑血管病杂志,2012,20(6):731-733.
[12] Sierra C.Cerebral small vessel disease,cognitive impairment and vascular dementia[J].Panminer va Med,2012,54(3):179-182.
[13] Takeda M,Yamashita T,Shinohara M,et al.Beneficial effect of anti-platelet therapies on Atheroscleroticlesion formation assessed by phase-contrast X-ray CT imaging[J].Int J Cardiovasc Imaging,2012,19(28):1 181-1 191.
[14] Chirumamilla AP,Maehara A,Mintz GS,et al.High platelet reactivity on clopidogrel therapy correlates with increased coronary atherosclerosis and calcification:a volumetric intravascular ultrasound study[J].JACC Cardiovasc Imaging,2012,5(5):540-549.
[15] Kim BJ,Lee SW,Park SW,et al.Insufficient platelet inhibition is related to silent embolic cerebral infarctions after coronary angiography[J].Stroke,2012,43(3):727-732.
[16] 陈熤,李剑,施海明.血小板致动脉粥样硬化斑块形成的相关研究[J].国际心血管病杂志,2010,27(13):234-236.
[17] Köklü E,Arslan S,Yüksel IO,et al.Acute Carotid Artery Stent Thrombosis Due to Dual Antiplatelet Resistance[J].Cardiovasc Intervent Radiol,2014,13(29):541-543.
(收稿2015-11-02)
Correlation of clopidogrel resistance and carotid artery stenosis in ischemic stroke patients
Xue Senxin*,Zhou Borong,Song Chengxian,Deng Yanhua
*DepartmentofRehabilitation,theThirdAffiliatedHospitalofGuangzhouMedicalUniversity,Guangzhou510150,China
Objective To investigate the correlation between clopidogrel resistance(CR) and carotid artery stenosis in patients with ischemic stroke.Methods Turbidimetry was used to measure the changes of platelet aggregation rate after the included patients with ischemic stroke taking 75 mg of clopidogrel per day for two weeks.The patients were divided into either CR or clopidogrel sensitivity(CS) group according to the changes of platelet aggregation rate.The demographic and clinical data of both groups were compared.Multivariate logistic regression analysis was used to identify the independent risk factors for CR.Results A total of 228 patients with ischemic stroke were included,among whom 54 cases(23.68%) were in the CR group and 174(76.32%) were in the CS group.Single factor analysis showed that there were statistical differences between the two groups in terms of age(P=0.015),platelet count(P=0.012),moderate carotid stenosis(P=0.034),gender(P=0.049) and diabetes(P=0.032).Multiariable logistic analysis results presented that age(P=0.004),platelet count(P=0.025),diabetes(P=0.026) and moderate carotid stenosis(P=0.002) were the independent risk factors for CR.Conclusion CR existing in patients with ischernic stroke may be associated with a variety of factors,in which moderate carotid artery stenosis is one of the risk factors for CR.
Ischemic stroke;Clopidogrel resistance;Platelet aggregation;Carotid artery stenosis
R743.33
A
1673-5110(2016)21-0008-03
