体素内不相干运动DWI对肝脏良恶性病变的诊断价值
2016-11-26韦素岚叶枫余小多宋颖欧阳汉
韦素岚,叶枫,余小多,宋颖,欧阳汉
·腹部影像学·
体素内不相干运动DWI对肝脏良恶性病变的诊断价值
韦素岚,叶枫,余小多,宋颖,欧阳汉
目的:探讨体素内不相干运动(IVIM)扩散加权成像对肝脏良恶性病变的诊断价值。方法:搜集2014年12月-2015年7月临床怀疑为肝脏肿瘤、且经手术病理、穿刺活检、临床或随访明确诊断的92例患者(共93个病灶)的病例资料,其中恶性组69例、良性组23例(24个病灶)。所有患者均行常规MRI平扫、多期动态增强扫描及IVIM(b=0、20、50、100、200、400、600、800和1200s/mm2)。将ROI放置于肿瘤最大实性区域,采用单指数及双指数模型获得以下参数值:表观扩散系数(ADC)、慢速表观扩散系数(D)、快速表观扩散系数(D*)及快速扩散成分所占比例(f)。采用独立样本t检验比较良恶性组间各参数的差异,并采用受试者工作特征曲线(ROC)计算各参数的诊断效能。结果:良性病变的ADC、D、D*和f值分别为(1.67±0.59)×10-3、(1.23±0.34)×10-3、(36.13±17.84)×10-3mm2/s和(29.96%± 15.67%),恶性组者分别为(1.20±0.36)×10-3、(0.88±0.21)×10-3、(34.84±19.75)×10-3mm2/s和(21.77%± 10.07%)。除D*值外,ADC值、D值及f值在两组间的差异有统计学意义(P值分别为0.001、0.000及0.023),相应ROC下面积分别为0.764、0.804及0.665。以D值<1.13×10-3mm2/s为阈值,诊断肝脏恶性肿瘤的敏感度及特异度分别为85.5%和62.5%。结论:体素内不相干运动扩散加权成像有助于肝脏良恶性病变的鉴别,其中使用双指数模型计算的慢速表观扩散系数值诊断效能最高。
肝肿瘤;磁共振成像;扩散加权成像;体素内不相干运动;诊断效能
Le Bihan等[1]提出的体素内不相干加权运动(intravoxel incoherent motion,IVIM)理论旨在将组织中进行布朗运动的纯水分子扩散与进行非布朗运动的微循环灌注相关的扩散区分开来,用以反映组织的微观结构及微循环情况,目前基于此理论的体素内不相干运动扩散加权成像(diffusion-weighted imaging of intravoxel incoherent motion,IVIM-DWI)技术在肝脏疾病方面研究报道较多[2-10],但对于肝脏局灶性病变的诊断价值,各研究报道尚存在一定分歧[4-8]。因此,
本研究通过回顾性分析92例肝脏局灶性病变的临床和影像学资料,旨在探讨IVIM-DWI对肝脏良恶性病变的鉴别诊断价值及确定各有效参数的阈值。
材料与方法
1.病例搜集
2014年12月-2015年7月于我院就诊的临床怀疑为肝脏肿瘤的92例患者,均行肝脏常规MRI平扫、多期增强扫描及IVIM-DWI检查。男65例,女27例,年龄14~73岁,平均52岁。恶性组69例(69个病灶),包括肝细胞肝癌53例、肝内胆管细胞癌7例和转移瘤9例;良性组23例(24个病灶),包括海绵状血管瘤11例(12个病灶)、局灶性结节性增生5例、感染5例、囊肿1例及血管平滑肌脂肪瘤1例。92例中经手术或穿刺病理证实者共52例:肝细胞癌30例,胆管细胞癌7例,转移瘤7例,海绵状血管瘤1例,局灶性结节增生4例,感染1例,囊肿1例,血管平滑肌脂肪瘤1例;40例经临床资料、典型影像特征(CT或超声)及随访6个月以上等明确诊断,肝细胞肝癌的诊断参照《原发性肝癌诊疗规范(2011年版)》[11]临床诊断标准。
2.成像方法
使用GE Discovery MR 750 3.0 TM R扫描仪和体部专用8通道相控阵线圈。检查前患者均需禁食4 h及训练呼吸,呼吸训练要求均匀自由呼吸及呼吸末屏气,检查时呈仰卧位,扫描范围包括全肝。检查序列如下。①屏气横轴面双回波T1WI;②呼吸触发脂肪抑制横轴面T2WI;③呼吸触发横轴面IVIM-DWI,扫描参数:TE 60.8 ms,TR 3529 ms,矩阵128×160,视野34.0 cm×27.2 cm~40.0 cm×32.0 cm,层厚7 mm,层间距1 mm,共选择9个b值(0、20、50、100、200、400、600、800和1200 s/mm2);④横轴面及冠状面屏气LAVA动态增强序列:使用高压注射器经手背静脉注入对比剂Gd-DTPA,剂量0.2 mL/kg,流率2 mL/s,随后采用相同流率注入20 mL生理盐水冲管,于注射对比剂后20 s、60 s、2 min及3 min分别动脉期、门脉早期、门脉晚期及延迟期图像。
3.图像后处理及数据测量
使用GE AW 4.6工作站和Function-MADC软件处理所采集的DWI图像,分别得到单指数模型和双指数模型的参数图,包括表观扩散系数(apparent diffusion coefficient,ADC),慢速表观扩散系数(slow apparent diffusion coefficient,D)、快速表观扩散系数(fast apparent diffusion coefficient,D*)及快速扩散成分所占比例(fraction of fast apparent diffusion coefficient,f)。结合脂肪抑制T2WI及多期动态增强图像,在IVIM图像上选择图像伪影较小及肿瘤坏死较少的病变层面,将感兴趣区(region of interest,ROI)放置于肿瘤最大实性区域(图1),避开出血、坏死及囊变区,测量3次,取均值,分别得到病变的ADC值、D值、D*值及f值。
4.统计分析
所测数据使用SPSS 17.0统计软件进行分析。采用独立样本t检验比较良恶性组间各参数(ADC值、D值、D*值及f值)间的差异。根据诊断结果绘制受试者工作特征曲线(receiver operating characteristic curve,ROC),比较各参数值的曲线下面积(area under curve,AUC)以评定其诊断效能,并以最大约登指数判定各参数的最佳诊断阈值。P<0.05为差异有统计学意义。
结 果
肝脏良恶性病变DWI各参数的测量值见表1、2。

表1 肝脏良性病变DWI各参数值

表2 肝脏恶性病变DWI各参数值
对于肝脏良恶性病变的鉴别诊断,ADC、D、D*及f的ROC曲线下面积分别为0.764、0.804、0.534及0.665(图2);除D*值外,肝脏良恶性病变的ADC值、D值及f值的差异有统计学意义(表3)。当ADC值、D值及f值的阈值分别为1.58×10-3mm2/s、1.13×
10-3mm2/s和31.35%时,诊断肝脏恶性病变的敏感度分别为89.9%、85.5%和89.9%,特异度分别为58.3%、62.5%和45.8%。
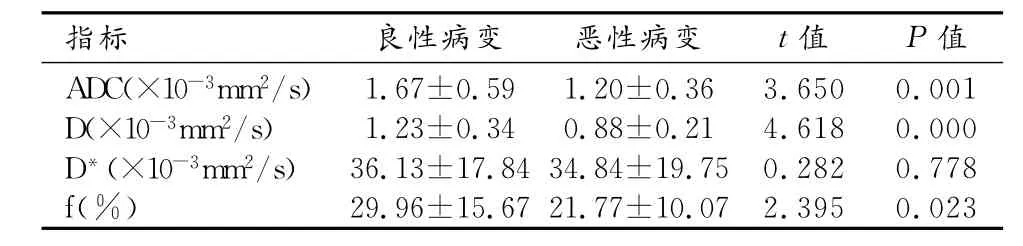
表3 肝脏良恶性病变DWI参数值比较
讨 论
扩散加权成像在肝脏肿局灶性病变的检出和定性、肝脏恶性肿瘤的疗效评估以及肝脏弥漫性病变的诊断中发挥着越来越重要的作用[12]。由于恶性肿瘤细胞密度增大,组织扩散受限,ADC值下降明显且低于良性病变,因此ADC值的定量分析可用于肝脏良恶性病变的鉴别诊断[13-16]。然而,研究表明肝脏良恶性肿瘤的ADC值存在一定范围内的重叠,不同研究获得的诊断恶性肿瘤的阈值差异也较大[17-18],一方面是因为ADC值受成像时选择的b值的影响,存在测量偏差[19];另一方面则是因为组织中非布朗运动的水分子运动成分,如血液流动,构成了表观扩散的一部分[20]。因此,Le Bihan等[1]提出IVIM理论,将组织中进行布朗运动的纯水分子扩散与进行非布朗运动的微循环灌注相关的扩散区分开来,分别测量D、D*及f值,从而得到组织中纯水分子扩散成分、微循环灌注成分及毛细血管血流量比例等方面的信息,以便于更好地反映组织的微观结构及微循环情况。本研究中肝脏良恶性病变的ADC值大于D值,与文献报道结果一致[4-6],说明组织的ADC值不仅受到反映病变细胞密度变化的D值的影响,还受到反映微循环灌注信息的D*值的影响,在临床应用时应考虑到部分恶性肿瘤的高灌注情况[1],如富血供的肝细胞癌和神经内分泌性肿瘤肝转移,以及影响肝组织灌注变化的情况(如应在肝脏检查前禁食,避免进食所导致的门脉及肝血窦灌
注增加[21])。
在本研究中,肝脏良性病变的ADC、D、D*及f值均高于恶性病变,除D*值外,ADC、D及f值在肝脏良恶性病变间的差异有统计学意义,其ROC下面积分别为0.764、0.804及0.665,提示IVIM-DWI有助于肝脏良恶性病变的鉴别诊断,其中D值的诊断效能最高。该结果与Yoon等[4]的研究结果相仿,说明在分析组织的水分子扩散信息时,剔除组织微循环灌注D*值的影响有利于反映组织的微观结构,比如部分高灌注的恶性肿瘤,剔除灌注影响后,D值能有效的反映恶性肿瘤的细胞密度、大小等微观变化。本研究结果显示,D值在肝脏良恶性病变的鉴别中诊断效能最高,其AUC为0.804,阈值为1.13×10-3mm2/s时诊断敏感度为85.5%,特异度为62.5%。这一结果与文献报道不同[4,6,8],笔者认为出现这种差异的原因可能与不同研究中所鉴别的病变类型不同有关。Yoon等[4]的研究中良性病变有海绵状血管瘤、局灶性结节增生及腺瘤,D值的阈值为1.27×10-3mm2/s;本研究纳入的良性病变包括海绵状血管瘤、局灶性结节增生、感染、囊肿及血管平滑肌脂肪瘤,D值阈值与Yoon等[4]的研究结果较为接近;而Watanabe等[6]的研究中良性病变为海绵状血管瘤及囊肿,Zhu等[4]的研究中为海绵状血管瘤,D值的阈值分别为1.54×10-3及1.66×10-3mm2/s,明显高于本研究结果。而且,研究中发现海绵状血管瘤及囊肿的D值明显高于恶性病变,提示探讨D值对肝脏良恶性病变的鉴别诊断价值时,应考虑病变类型,因为海绵状血管瘤和囊肿的高D值可能会导致鉴别肝脏良恶性病变的D值的阈值升高。
本研究中D*值在良恶性病变间的差异无统计学意义,与Watanabe[6]和Zhu等[8]的研究一致,分析原因可能为一方面虽然D*值反映的是组织的微循环灌注情况,但实际上可能还包含了组织的腺体分泌如胆汁分泌等微观水分子运动的信息[22];另一方面则是部分肝脏良恶性肿瘤间的微循环灌注情况差异可能很小[5]。并且,在分析D*值诊断价值时还应注意到D*值计算误差及其可重复性方面的问题。研究发现D*值的计算误差较高,尤其在低b值时,即使增加了b值数目,D*的重复性仍较差。Andreou等对14例结肠癌肝转移患者进行了2次肝脏多b值DWI扫描,结果显示两次扫描测量的D*及f的可重复性均较差,且转移灶的D*及f的可重复性差于正常肝实质;两次测量百分比差异的95%置信区间分别为转移灶D*(-89.0%,2,120%)、f(-75.3%,241%),正常肝实质D*(-31.2%,59.1%)、f(-24.3,25.1%)[23]。另外,Kakite等[24]的研究中则发现肝实质和肝细胞癌的灌注参数中D*和f值的可重复性差,扩散参数D、ADC的重复性好,而且肝细胞肝癌的灌注参数D*和f的可重复性要差于肝实质。
本研究的局限性有以下几点:①本研究为回顾性研究,入组的恶性病变例数多于良性病变,可能存在抽样误差及队列误差,并且部分患者没有病理证实;②IVIM双指数模型的稳定性较单指数模型差,IVIM参数的变异度比传统ADC值要高,本研究没有对IVIM参数的可重复性进行进一步的研究;③ROI为人工勾画,可能存在测量误差。
总之,本研究结果显示IVIM-DWI有助于肝脏良恶性病变的鉴别诊断,其中双指数模型的D值诊断效能最高。
[1] Le Bihan D.Intravoxel incoherent motion imaging using steadystate free precession[J].Magn Reson Med,1988,7(3):346-351.
[2] Hu G,Chan Q,Quan X,et al.Intravoxel incoherent motion MRI evaluation for the staging of liver fibrosis in a rat model[J].J Magn Reson Imaging,2015,42(2):331-339.
[3] Chung SR,Lee SS,Kim N,et al.Intravoxel incoherent motion MRI for liver fibrosis assessment:a pilot study[J].Acta Radiol, 2015,56(12):1428-1436.
[4] Yoon JH,Lee JM,Yu MH,et al.Evaluation of hepatic focal lesions using diffusion-weighted MR imaging:Comparison of apparent diffusion coefficient and intravoxel incoherent motion-derived parameters[J].J Magn Reson Imaging,2014,39(2):276-285.
[5] Doblas S,Wagner M,Leitao HS,et al.Determination of malignancy and characterization of hepatic tumor type with diffusion-weighted magnetic resonance imaging:Comparison of apparent diffusion coefficient and intravoxel incoherent motion-derived measurements[J].Invest Radiol,2013,48(10):722-728.
[6] Watanabe H,Kanematsu M,Goshima S,et al.Characterizing focal hepatic lesions by free-breathing intravoxel incoherent motion MRI at 3.0 T[J].Acta Radiol,2014,55(10):1166-1173.
[7] Colagrande S,Regini F,Pasquinelli F,et al.Focalliver lesion classification and characterization in noncirrhotic liver:a prospective Comparison of diffusion-weighted magnetic resonance-related para meters[J].J Co m put Assist Tomogr,2013,37(4):560-567.
[8] Zhu L,Cheng Q,Luo W,et al.A comparative study of apparent diffusion coefficient and intravoxel incoherent motion-derived para meters for the characterization of common solid hepatic tumors [J].Acta Radiol,2015,56(12):1411-1148.
[9] Joo I,Lee JM,Grimm R,et al.Monitoring vascular disrupting therapy in a rabbit liver tumor model:relationship between tumor perfusion para meters at IVIM diffusion-weighted MR imaging and those at dynamic contrast-enhanced MR imaging[J].Radiology, 2015,278(1):104-113.
[10] Park YS,Lee CH,Kim JH,et al.Using intravoxel incoherent motion(IVIM)MR imaging to predict lipiodol uptake in patients with hepatocellular carcinoma following transcatheter arterial chemoembolization:a preliminary result[J].Magn Reson Imaging,2014,32(6):638-646.
[11] 中华人民共和国卫生部.原发性肝癌诊疗规范(2011年版)[J].临床肿瘤学杂志,2011,16(10):929-946.
[12] Lewis S,Dyvorne H,Cui Y,et al.Diffusion-weighted imaging of the liver:techniques and applications[J].Magn Reson Imaging Clin N Am,2014,22(3):373-395.
[13] Miller FH,Hammond N,Siddiqi AJ,et al.Utility of diffusion-weighted MRI in distinguishing benign and malignant hepatic lesions[J].J Magn Reson Imaging,2010,32(1):138-147.
[14] Demir OI,Obuz F,Sagol O,et al.Contribution of diffusion-weighted MRI to the differential diagnosis of hepatic masses[J]. Diagn Interv Radiol,2007,13(2):81-86.
[15] Taouli B.Diffusion-weighted MR imaging for liver lesion characterization:a critical look[J].Radiology,2012,262(2):378-380.
[16] Xia D,Jing J,Shen H,et al.Value of diffusion-weighted magnetic resonance images for discrimination of focal benign and malignant hepatic lesions:a meta-analysis[J].J Magn Reson Imaging, 2010,32(1):130-137.
[17] Taouli B,Vilgrain V,Dumont E,et al.Evaluation of liver diffusion isotropy and characterization of focal hepatic lesions with two single-shot echo-planar MR imaging sequences:prospective study in 66 patients[J].Radiology,2003,226(1):71-78.
[18] Bruegel M,Holzapfel K,Gaa J,et al.Characterization of focal liver lesions by ADC measurements using a respiratory triggered diffusion-weighted single-shot echo-planar MR imaging technique[J].Eur Radiol,2008,18(3):477-485.
[19] Goshima S,Kanematsu M,Kondo H,et al.Diffusion-weighted imaging of the liver:optimizing b value for the detection and characterization of benign and malignant hepatic lesions[J].J Magn Reson Imaging,2008,28(3):691-697.
[20] Yamada I,Aung W,Himeno Y,et al.Diffusion coefficients in abdominal organs and hepatic lesions:evaluation with intravoxel incoherent motion echo-planar MR imaging[J].Radiology,1999, 210(3):617-623.
[21] Hollingsworth KG,Lo mas DJ.Influence of perfusion on hepatic MR diffusion measurement[J].NMR Biomed,2006,19(2):231-235.
[22] Koh DM,Collins DJ,Orton MR.Intravoxel incoherent motion in body diffusion-weighted MRI:reality and challenges[J].AJR, 2011,196(6):1351-1361.
[23] Andreou A,Koh DM,Collins DJ,et al.Measurement reproducibility of perfusion fraction and pseudodiffusion coefficient derived by intravoxel incoherent motion diffusion-weighted MR imaging in normal liver and metastases[J].Eur Radiol,2013,23 (2):428-434.
[24] Kakite S,Dyvorne H,Besa C,et al.Hepatocellular carcinoma: short-term reproducibility of apparent diffusion coefficient and intravoxel incoherent motion para meters at 3.0 T[J].J Magn Reson Imaging,2015,41(1):149-156.
Intravoxel incoherent motion diffusion weighted imaging in differentiation between benign and malignant lesions of liver
WEI Su-lan,YE Feng,YU Xiao-duo,et al.Department of Diagnostic Radiology,Cancer Hospital,Peking Union Medical College, Chinese Academy of Medical Sciences,Beijing 100021,China
Objective:To determine the value of intravoxel incoherent motion(IVIM)diffusion weighted imaging (DWI)in differentiation between benign and malignant lesions of liver.Methods:From December 2014 to July 2015,92 patients with 93 liver lesions proved by postsurgical pathology,aspiration biopsy,clinical data or follow-up results were enrolled in our study,and were divided into two groups:malignant group(69 lesions in 69 patients)and benign group(24 lesions in 23 patients).All patients underwent conventional non-enhanced and contrast-enhanced MRI and IVIM-DWI(b=0, 20,50,100,200,400,600,800 and 1200s/mm2).ROIs were placed on the largest solid part of the lesions and parameters (ADC,D,D*and f)were measured with monoexponential model and biexponential model respectively.The values of these parameters in the two groups were analyzed and compared using independent samples t-test,and receiver operating characteristic curve(ROC)was used to determine the diagnostic efficacy of these parameters in diagnosis of malignant liver lesions.Results:The values of ADC,D,D*and f in benign group were(1.67±0.59)×10-3,(1.23±0.34)×10-3,(36.13± 17.84)×10-3mm2/s and(29.96%±15.67%),and those in malignant group were(1.20±0.36)×10-3,(0.88±0.21)× 10-3,(34.84±19.75)×10-3mm2/s and(21.77%±10.07%)respectively.Significant inter-group difference was observed in ADC,D and f(P=0.001,0.000 and 0.023,respectively),the correlated areas under the ROC curve of ADC,D and f were 0.764,0.804 and 0.665.With the cut-off of 1.13×10-3mm2/s,the sensitivity and specificity of D in diagnosis of malignant lesions of liver were 85.5%and 62.5%respectively.Conclusion:IVIM-DWI is useful to distinguish benign and malignant lesions of liver,and the D value in biexponential model has the best diagnostic efficacy for differentiation.
Liver neoplasms;Magnetic resonance imaging;Diffusion weighted imaging;Intravoxel incoherent motion;Diagnostic efficacy
R445.2;R735.7
A
1000-0313(2016)04-0364-05
10.13609/j.cnki.1000-0313.2016.04.019
2016-01-11
2016-03-05)
100021 北京,北京协和医学院中国医学科学院肿瘤医院影像诊断科
韦素岚(1987-),女,广西河池人,硕士研究生,主要从事腹部肿瘤的影像诊断工作。
